Keywords
Dry mouth; Gentleness; Moisturization; Mouthwashes; Sjögren’s syndrome, Water
Abbreviations
AE: Adverse Event; ANCOVA: Analysis of Covariance; ANOVA: Analysis of Variance; CPC: Cetylpyridinium Chloride; ITT: Intent-to-Treat; OHT: Oral Hard Tissue; OST: Oral Soft Tissue; PP: Per Protocol; PPUQ: Post-Product Use Questionnaire; PPUSQ: Post-Product Use Sensory Questionnaire; PPAQ: Product Performance Attribute Questionnaire; SD: Standard Deviation; SS: Sjögren’s Syndrome; TEAE: Treatment-Emergent AE; VAS: Visual Analogue Scale
Introduction
Dry mouth may affect nearly half of the adult population at some point in their lives, with prevalence varying depending on the diagnostic criteria used [1,2]. Oral dryness may be a consequence of an underlying medical condition such as Sjögren’s syndrome (SS) [3,4], other congenital or iatrogenic salivary gland dysfunction [5], a side effect of some medications/chemotherapy, radiation to the head and neck region [6-10], or due to graft versus host disease [11].
A dry mouth accompanied by salivary hypofunction can negatively affect mastication, deglutition, and speaking [12]. Furthermore, low salivary flow can contribute to dental erosion and caries, halitosis, and periodontitis [3]. Oral mucosal surfaces consequently become desiccated, friable, and more susceptible to abrasion [3]. As a result, many everyday oral hygiene treatments may not be gentle enough for individuals with dry mouth. In an observational study, Chevalier et al. [13] concluded that mouth rinses, predominantly containing quaternary ammonium compounds, may exacerbate xerostomia and cause further mucosal irritation. It is therefore essential that any treatment used by a person with dry mouth is gentle on the oral mucosa.
Frequent sipping of water is one of the most common strategies to relieve the sensation of dry mouth, particularly in individuals with severe salivary hypofunction [14,15]. While water temporarily hydrates the oral cavity, it does not contain the moisturizers and lubricants necessary to provide longer-lasting relief and may dilute salivary minerals, proteins, and buffers, which help maintain oral tissue health, pH, and enamel remineralization [12,16]. Other available remedies include chewing gum, overthe- counter topical lubrication treatments, and prescription sialogogues such as parasympathomimetic drugs [3,6,14,17,18].
Several studies have indicated that moisturizing mouthwash formulations may be beneficial in individuals with dry mouth symptoms [19,20]. In a recent 8-day trial (containing further results from the current Study 2), an experimental moisturizing mouthwash formulation with a preservative system incorporating cetylpyridinium chloride (CPC) instead of parabens was associated with a greater subjective relief of self-reported dry mouth symptoms when compared to water [21].
Given the importance of the availability of a gentle, nonirritating oral treatment for people with dry mouth symptoms, two randomized clinical trials were conducted to evaluate the sensory perception of the same experimental mouthwash as above (containing CPC) in participants with dry mouth symptoms, including those with SS. The primary aim of Study 1, a single-use study, was to investigate the perception of the experimental mouthwash versus water as related to gentleness, as assessed by question 1 of the Post-Product Use Questionnaire (PPUQ)1. Secondary objectives included other perception features assessed by the PPUQ and comparison of the ability of the experimental mouthwash versus water to relieve dry mouth symptoms immediately after use, as assessed by the Product Performance Attribute Questionnaire (PPAQ). Several exploratory objectives were also assessed including perception of gentleness with the experimental mouthwash versus water using a Visual Analogue Scale (VAS); objective assessment of mucosal wetness and saliva film thickness before and after treatment using a micro-moisture meter electronic instrument; and subjective assessment of moistness before and after treatment using a questionnaire.
Study 2 was an 8-day study, the primary efficacy results of which have previously been reported [21]. The sensory attributes of the experimental mouthwash (plus water as needed) compared with ‘Water-only’, evaluated with a Post-Product Use Sensory Questionnaire (PPUSQ) on Days 1, 3, and 8, are reported here.
Methods
These two randomized, examiner blind, stratified (by SS status) studies were conducted at Tufts University School of Dental Medicine, Boston, MA, USA. Study protocols were approved by the Tufts Health Sciences Institutional Review Board (#12013 and #12052, respectively) and procedures were performed in accordance with the Declaration of Helsinki, the International Conference on Harmonization Good Clinical Practices, and relevant local laws and regulations. All participants provided voluntary written informed consent and demonstrated the ability to understand and comply with study protocols before procedures commenced. The trials were registered at clinicaltrials.gov (NCT03005041 and NCT02641912, respectively). Primary data from Study 2 has been published previously [21]; therefore, methodology details will be provided only in brief.
In Study 2, there were amendments to the Statistical Analysis Plan after study unblinding to include additional summary tables and include sub-group analysis. Additionally, as the site was not able to recruit the planned number of SS participants to achieve a 2:3 ratio as specified in the protocols, the missing SS participants were replaced with non-SS participants. These changes had no impact on safety or the scientific quality of the study.
Participants
In both studies, eligibility criteria included participants aged 18 to 84 years who were in good general health (no clinically significant and relevant abnormalities in medical history or upon oral examination), had subjective reporting of dry mouth, and had an ability to read and write in English to answer the questionnaires. Stimulated (with inert gum base) and unstimulated salivary flow rates were also assessed at screening. Participants in Study 1 were required to have an unstimulated whole salivary flow rate of ≤0.1 mL/min; simulated and unstimulated flow rates were assessed in Study 2 for exploratory purposes only. Medical records were reviewed for confirmation of SS diagnosis based on the positivity of salivary gland biopsy, SS-A (anti-Ro antibody), SS-B (La antibody), or a letter from a physician (if diagnosis was made more than 3 years previously). The diagnosis of SS was based on American-European Consensus Group criteria for classification in prevalence at that time [22]. Study 1 and 2 included two and three participants respectively who were considered to have SS based on positive SS-B but who may not be considered to have SS based on the more recent ACR/EULAR consensus criteria and a pathologist-led consensus paper [23,24].
Oral dryness was assessed using a modification of the Dry Mouth Screening Questionnaire taken from the Dry Mouth Inventory. Participants rated each of the following statements on a six-point scale from ‘Strongly disagree’ to ‘Strongly agree’: 1) No moisture in the mouth; 2) Lips sticking to teeth; 3) Tongue sticking to roof of mouth; 4) Throat dry. To be eligible for randomization, participants had to answer at least two of the questions with ‘Agree a little’, ‘Agree’, or ‘Strongly agree’. Participants were al. so assessed using the Clinical Oral Dryness Score which evaluates 10 signs of dryness as being present or absent (e.g. ‘mirror sticks to tongue’, ‘altered gingival architecture’, and ‘cervical caries’) giving a total score of 1 (least severe) to 10 (most severe) [25]. These assessments were for confirmation of dry mouth only and were not used as study measures.
Participants were excluded if they wore complete dentures; were using variable doses of prescription sialagogues; were pregnant or breast-feeding; were receiving chemo- and/or radiotherapy; or had: significant medical comorbidities; oral abnormalities that could interfere with study conduct; gross intra-oral neglect; need for extensive dental therapy; known or suspected intolerance or hypersensitivity to study materials; and use of any investigational drugs or participation in another clinical trial within 14 days of screening.
Study treatments
In both studies, participants who met all eligibility criteria were randomized according to a schedule generated by the Biostatistics Department of GSK Consumer Healthcare using validated internal software. Randomization was stratified based on confirmed SS status (yes/no); randomization numbers were assigned in ascending numerical order as each participant was determined to be fully eligible.
Study treatments were an experimental mouthwash (with ingredients including glycerin, xylitol, sorbitol, propylene glycol, poloxamer 407, potassium sorbate, natrosol 250-M, sodium phosphate monobasic anhydrous, CPC, and disodium phosphate anhydrous) or water (Volvic® Natural Spring Water [pH 7.0; Danone Eaux France, Lyon, France]) at study center visits; water of their choice at home for Study 2.
The dental examiner, study statistician and employees of the sponsor who could influence study outcomes were not aware of treatment allocation or sequence. Participants were dispensed study treatment in rinsing cups and instructed not to discuss which group they thought they were allocated to with the examiner. While participants were not directly informed of their group allocation, inferences of such could be made due to the sensory and treatment regimen differences between the Mouthwash and Water groups.
Study 1: Study 1 was a single-use crossover study. At the screening/treatment visit, full oral soft tissue (OST) and oral hard tissue (OHT) examinations were performed and dry mouth status was objectively confirmed as above. Prior to treatment use, the dental examiner used a micro-moisture meter electronic instrument (Periotron 8010®; Oraflow Inc., New York, NY, USA) to objectively assess mucosal wetness and saliva film thickness [25]. Participants were asked to rate the level of moistness in their mouth from ‘poor’ to ‘excellent’ on a questionnaire.
Participants were initially randomized (1:1) to single use of the experimental mouthwash (Mouthwash group) or of Volvic® Natural Spring Water (Water group). A wash-out period of 1 to 7 days separated study visits with the groups crossed-over on the second visit such that each participant received the alternative treatment at the second visit.
Following the above assessments, participants used their assigned study treatment under supervision of trained site staff. They rinsed their mouth for 30 seconds with 15 mL of the study treatment then expectorated. PPUQ1 was completed within 2 minutes of supervised treatment use, PPAQ within 5 minutes of treatment use, and PPUQ2 at 30 (±5) minutes after treatment use (Table 1 for details of these questionnaires). Periotron® assessment of moisturization and subjective rating of moistness were repeated at 30 (±5) minutes after treatment use. For the questionnaire administration schedule see Supplemental Table 1.
Table 1 The post-product use questionnaire (PPUQ) and post-product use sensory questionnaire (PPUSQ).
| PPUQ1: Immediately post-use (Study 1 only) |
1) How much do you agree or disagree with the statement: This product is gentle? ‘Disagree strongly’, ‘Disagree’, ‘Neither agree or disagree’, ‘Agree’ or ‘Agree strongly’ |
| 2) How gentle do you think this product is? Score on a 100 mm visual analogue scale from ‘Not at all gentle’ to ‘Extremely gentle’ |
| 3) Which of the following statements best describes how much you liked the product overall? ‘Liked it extremely’, ‘Liked it very much’, ‘Liked it somewhat’, ‘Liked it slightly’, ‘Did not like it that much’, or ‘Did not like it at all’ |
| PPUQ2: 30 minutes’ post-use (Study 1 only) |
1) Are you experiencing any of the following sensations in your mouth and how strong is the sensation: moisturizing, soothing, refreshing, tingling, numbing, burning, drying out? ‘None’, ‘Mild’, ‘Moderate’ or ‘Severe’ |
| 2) Would you continue use of the product? Yes/No |
| PPAQ: Within 5 minutes’ use (Study 1 only) |
Score on a five-point scale where 1=poor, 2=fair, 3=good, 4=very good, and 5=excellent:
1) Having an immediate dry mouth relief; |
| 2) Having an immediate lubricating feeling; and |
| 3) Having an immediate moisturizing effect |
| 4) Which of the following statements best describes how much you liked the overall flavor of the rinse? ‘Liked it extremely’, ‘Liked it very much’, ‘Liked it somewhat’, ‘Liked it slightly’, ‘Did not like it that much’, or ‘Did not like it at all’ |
| 5) How would you rate the flavor intensity of the oral rinse? ‘Strongest flavor imaginable’, ‘Very strong’, ‘Strong’, ‘Moderate’, ‘Weak’, ‘Barely detectable’, or ‘No flavor at all’ |
| 6) Did you experience any of the following sensations in your mouth and how strong was the sensation: moisturizing, soothing, refreshing, tingling, numbing, burning, drying out? ‘None’, ‘Mild’, ‘Moderate’ or ‘Severe’ |
| 7) When did you experience each of the following sensations in your mouth: moisturizing, soothing, refreshing, tingling, numbing, burning, drying out? ‘Initially – first contact with mouth’, ‘During use – whilst swishing in the mouth’, ‘After use – after spitting out the product’ |
| PPUSQ: Immediately post-use, Days 1, 3, 8 (Study 2 only) |
1) Which of the following statements best describes how much you liked the product overall? ‘Like it very much’, ‘Like it somewhat’, ‘Like it slightly’, ‘Did not like it that much’, or ‘Did not like it at all’ |
| 2) How pleasant would you say the flavor of the product was? ‘Extremely pleasant’, ‘Very pleasant’, ‘Moderately pleasant’, ‘Slightly pleasant’, or ‘Not pleasant at all’ |
| 3) How gentle would you say the product was? ‘The most gentle product imaginable’, ‘Extremely gentle’, ‘Very gentle’, ‘Moderately gentle’, ‘Slightly gentle’, ‘Barely gentle’, or ‘Not gentle at all’ |
| 4) How fresh would you say your mouth felt after using the product? ‘Extremely fresh’, ‘Very fresh’, ‘Somewhat fresh’, ‘Not very fresh’, or ‘Not at all fresh’ |
An OST examination was performed at the end of each treatment visit and an OHT examination was performed after Visit 2, prior to participants leaving the clinical site. Throughout the study period, participants were permitted to use their regular toothbrush and toothpaste (including any prescription toothpaste) and to continue their current prescription sialagogues with no changes in dose/frequency. Participants were required to record treatment details and frequency on diary cards.
Study 2: Study 2 was a parallel group study conducted over 8 days. At the screening/treatment visit, SS and dry mouth status was confirmed as above and participants underwent OST and OHT examinations. Participants were randomized (1:1) to one of two treatment groups: 8 days’ use of the mouthwash or 8 days’ use of water only (Volvic® Natural Spring Water at study center visits; water of their choice at home). At each treatment visit, participants used their assigned treatment under supervision whereby the Mouthwash group rinsed with 15 mL of the study treatment for 30 seconds before expectorating; the Water group took one measured 15 mL drink of water (non-expectorated). At home, Mouthwash group participants used a maximum of two mouthwash doses per day. Both Mouthwash group and Wateronly group participants could drink water (not supplied) as often as required.
On study center visit days (1,3 [±1 day], and 8 [±1 day]), participants completed the PPUSQ within 2 minutes after supervised treatment use (questionnaire details in Table 1). At all visits, an OST examination was performed before and after supervised treatment use at site. An OHT examination was performed on Days 1 and 3. Participants used their own toothbrush and toothpaste during the study and were provided with a diary card and instructions to take home. Participants refrained from using all oral care products for dry mouth relief from screening until study completion except prescription sialogogues if the dose was stable.
Safety
In both studies, safety was assessed based on any oral adverse events (AEs) including treatment-emergent abnormalities in the OST examination, spontaneously reported AEs and AEs recorded in the participants’ diaries. AEs were recorded from the start of the study for each participant until 5 days following last administration of the study treatment.
Statistical analysis
In both studies, the safety population was defined as all randomized participants who received at least one dose of study treatment. The efficacy analysis was performed on the intent-totreat (ITT) population, defined as all participants who received the study treatment and had at least one post-baseline efficacy measurement. The per protocol (PP) population was defined as those in the ITT population who had at least one assessment of efficacy considered unaffected by protocol violations.
Study 1
Approximately 70 participants were planned to be screened to ensure that 55 were randomized with at least 50 completing the study. While no formal sample size calculations were performed, this sample size was considered sufficient to provide a reasonable estimate of the percentage of participants who ‘agreed strongly’ or ‘agreed’ that the experimental product was ‘gentle’, based on Study 2 [21].
The primary efficacy variable was response to Question 1 on PPUQ1 – ‘This product is gentle’ – on a five-item Likert scale. No formal statistical comparisons between treatments were performed. Secondary efficacy variables were responses to PPUQ1 Questions 3–7, PPUQ2 Questions 1 and 2, and PPAQ Questions 1–4. For the PPAQ, each question was analyzed using an analysis of variance (ANOVA) model with factors for period, treatment and confirmed SS status (Yes/No) as fixed effects and participant as random effect. Exploratory efficacy variables included response to PPUQ1 Question 2 and change from pretreatment use to post-treatment use in mucosal wetness, saliva film thickness and subjective level of moistness. Change was analyzed using an analysis of covariance (ANCOVA) model with factors for period, treatment and SS (yes/no) as fixed effects, participant as a random effect, and participant-level pre-treatment and period minus participant-level pretreatment values as covariates. No comparison was made between treatment groups.
Post-hoc analysis of summaries of the PPUQ 1 and PPUQ 2 endpoints, the PPAQ and assessment of the exploratory endpoints are also presented separately for each stratum (confirmed SS status [yes/no]). For the PPAQ, comparisons were made within each subgroup (confirmed SS status [yes/no]). Subgroup analyses were achieved by including a treatment*SS interaction term in the ANOVA model. For mucosal wetness, saliva film thickness and level of moistness, changes from pre- to post-treatment use were obtained for each treatment within each subgroup with no comparisons between treatments. For all analyses, the assumptions of normality and homogeneity of variance were investigated, and no gross deviations were found.
Study 2
No formal sample size calculations were performed. Approximately 150 participants were planned to be screened to ensure 100 completed the study. Primary efficacy and some secondary efficacy variables were described and reported in a previous study [21]. The secondary efficacy value reported here is response to the PPUSQ on Days 1, 3 and 8. Each question was analyzed separately using an ANOVA model with factors for treatment and confirmed SS status (yes/no) stratification using Observed Margin option. For each treatment group, adjusted means, p-value and 95% CIs were calculated. The assumption of normality and homogeneity of variance were investigated and no gross deviations were found.
Results
For Study 1, the first participant was enrolled in August 2016 and the final participant completed the study in October 2016. Of the 58 participants screened, 55 were randomized to treatment and completed the study. In Study 2, the first participant was enrolled in March 2016 and the final participant completed the study in April 2016. Of the 104 participants screened, 100 were randomized to treatment and completed the study. All randomized participants across both studies were included in the ITT, PP and safety populations (Figure 1). Participant demographics are shown in Table 2. In Study 1, mean baseline Clinical Oral Dryness Score was 3.5 points (SD 1.80), indicating mild–moderate oral dryness; in Study 2, mean score was 2.19 points (SD 2.057) in the Mouthwash group and 2.43 (SD 2.093) in the Water-only group, indicating mild oral dryness for both. All Study 1 participants had an unstimulated whole salivary flow rate of ≤0.1 mL/min. For Study 2, the stimulated/unstimulated salivary flow rates at baseline were 0.93 (SD 0.875)/0.16 (SD 0.269) mL/min for those without SS and 0.58 (SD 0.518)/0.14 (SD 0.269) mL/min for those with SS.
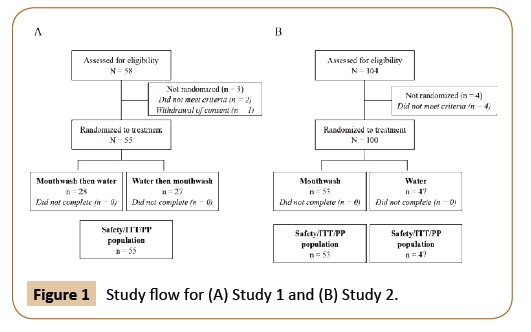
Figure 1: Study flow for (A) Study 1 and (B) Study 2.
Table 2 Participant demographics (safety population).
| |
Study 1 (N=55) |
Study 2 |
| Mouthwash (N=53) |
Water-only (N=47) |
| Gender, n (%) |
Female |
15 (27.3) |
36 (67.9) |
28 (59.6) |
| Male |
40 (72.7) |
17 (32.1) |
19 (40.4) |
| Race, n (%) |
White |
42 (76.4) |
35 (66.0) |
29 (61.7) |
| Black/African-American |
7 (12.7) |
11 (20.8) |
16 (34.1) |
| Asian |
1 (1.8) |
4 (7.6) |
1 (2.1) |
| American Indian/Alaska Native |
1 (1.8) |
0 |
0 |
| Native Hawaiian/other Pacific Islander |
1 (1.8) |
0 |
0 |
| Multiple |
2 (3.6) |
0 |
0 |
| Missing |
1 (1.8) |
3 (5.7) |
1 (2.1) |
| Mean age, years (SD) |
54.2 (14.5) |
50.7 (14.4) |
51.6 (14.1) |
| Confirmed SS, n (%) |
22 (40.0) |
14 (26.4) |
14 (29.8) |
SD: Standard Deviation; SS: Sjögren's Syndrome.
Study 1
Primary efficacy variable: Response to PPUQ1 Question 1 – ‘This product is gentle’ (Table 3). Overall, the majority of participants ‘Agreed’ or ‘Strongly agreed’ that both the Mouthwash and Water were gentle (78.2 and 89.1%, respectively). Similar results were observed when participants were analyzed according to whether or not they had confirmed SS.
Table 3 Study 1: Response to PPUQ1 Question 1 – ‘This product is gentle’ (primary efficacy variable; ITT population).
| |
All participants (N=55) |
Participants with SS (N=22) |
Participants without SS (N=33) |
| Mouthwash |
Water |
Mouthwash |
Water |
Mouthwash |
Water |
| Agree/strongly agree, n (%) [95% confidence interval] |
43 (78.2) [65.0, 88.2] |
49 (89.1) [77.8, 95.9] |
15 (68.2) [45.1, 86.1] |
22 (100.0) [84.6, 100.0] |
28 (84.8) [68.1,94.9] |
27 (81.8) [64.5, 93.0] |
| Agree strongly, n (%) |
17 (30.9) |
28 (50.9) |
3 (13.6) |
14 (63.6) |
14 (42.4) |
14 (42.4) |
| Agree, n (%) |
26 (47.3) |
21 (38.2) |
12 (54.5) |
8 (36.4) |
14 (42.4) |
13 (39.4) |
| Neither agree or disagree, n (%) |
6 (10.9) |
5 (9.1) |
4 (18.2) |
0 |
2 (6.1) |
5 (15.2) |
| Disagree, n (%) |
5 (9.1) |
0 |
3 (13.6) |
0 |
2 (6.1) |
0 |
| Disagree strongly, n (%) |
1 (1.8) |
1 (1.8) |
0 |
0 |
1 (3.0) |
1 (3.0) |
SS: Sjögren's Syndrome
PPUQ1 Question 2 (exploratory efficacy variable): Overall, mean VAS score (SD) regarding perception of gentleness was 71.0 (24.17) in the Mouthwash group and 84.5 (19.50) in the Water group. Similar results were observed for participants with SS (65.6 [24.53] and 88.5 [12.53], respectively) and without SS (74.7 [23.61] and 81.8 [22.79], respectively).
Secondary efficacy variables PPUQ1 Questions 3-5: Overall, 72.7% and 61.8% of participants liked the Mouthwash or its flavor, respectively, ‘Extremely’/‘Very much’. In the Mouthwash group, 50.9% rated the flavor as ‘Strongest flavor imaginable’/‘Very strong’/‘Strong’, whereas only 1.8% rated Water as such. Similar results were observed for participants with and without SS (Figure 2 and Supplemental Table 2).
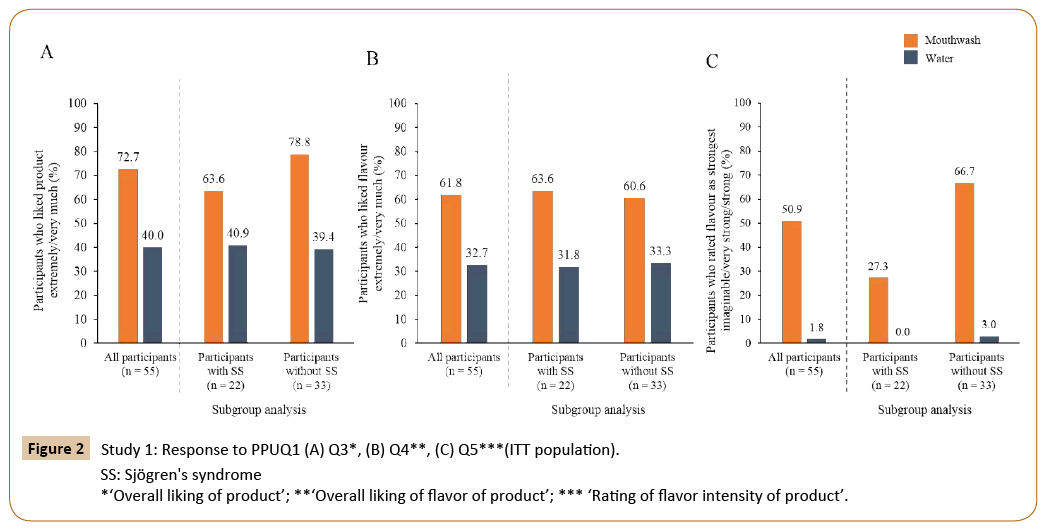
Figure 2: Study 1: Response to PPUQ1 (A) Q3*, (B) Q4**, (C) Q5***(ITT population).
PPUQ1 Questions 6–7, PPUQ2 Question 1-2: Within 2 minutes of Mouthwash use, over 90% of participants in each category experienced moisturizing, soothing, and refreshing sensations; more than 80% experienced these sensations at 30 minutes after use. Water was experienced as moisturizing, soothing, and refreshing by more than 70% of participants in each category within 2 minutes, which decreased to 51%, 26% and 22%, respectively at 30 minutes (Figure 3 and Supplemental Table 3).
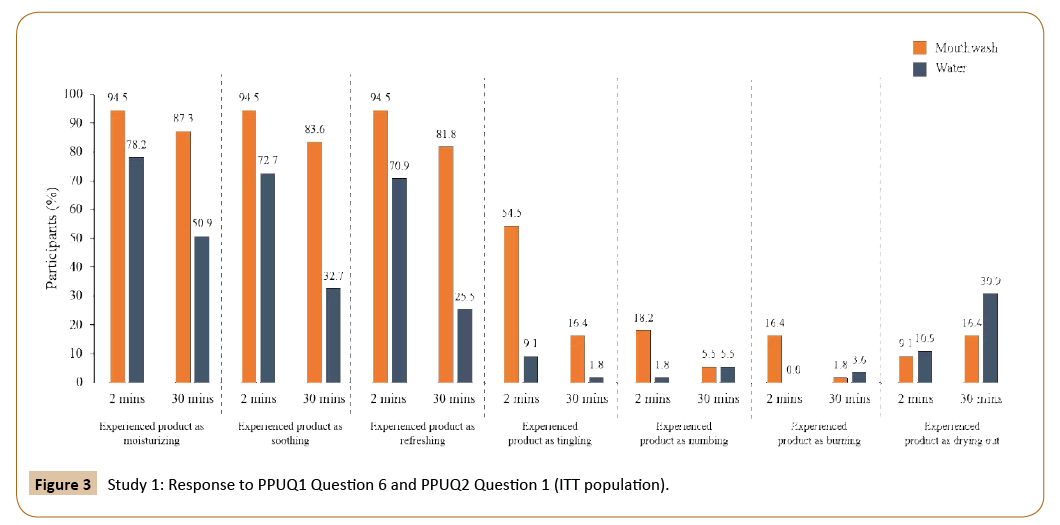
Figure 3: Study 1: Response to PPUQ1 Question 6 and PPUQ2 Question 1 (ITT population).
In the Mouthwash group, of those who experienced moisturizing, soothing or refreshing sensations at 2 mins (n=52 for all), this was reported respectively as being experienced initially (58%/44%/58%), during (58%/65%/62%), and after (65%/54%/62%) treatment, respectively. For the Water group, these initial/during/after use percentages were, 70%/63%/39% for moisturizing (n=43), 55%/75%/27.5% for soothing (n=40) and 51%/56%/33% for refreshing (n=39).
Within 2 minutes of Mouthwash use, 54% of participants reported a tingling sensation, which decreased to 16% at 30 minutes after use. A minority of participants within 2 or at 30 minutes after Mouthwash use report numbing (18%/5%), burning (16%/2%) or drying out (9%/16%) sensations, which most categorized as ‘mild’. Of those who experienced tingling, numbing, burning or drying out sensations at 2 minutes, this was reported respectively as being experienced initially/during/after use by 33%/57%/40% for tingling (n=30), 30%/20%/40% for numbing (n=10), 22%/44%/33% for burning (n=9) and 20%/20%/100% for drying out (n=5).
As expected, at 2 or 30 minutes after Water use, few participants reported tingling (9%/2%), numbing (2%/5%) or burning (0%/4%); however, 11% within 2 minutes and 31% at 30 minutes reported drying out. Initial/during/after use percentages for those who experienced these sensations were, 0%/80%/20% for tingling (n=5), 100%/100%/0% for numbing (n=1) and 33%/17%/67% for drying out (n=6).
The majority of participants (n=43 [78%]) stated that they would continue to use the Mouthwash, while only 20 participants (36%) would continue using Water.
PPAQ: There was a statistically significant between-treatment difference of around 1 point (good–very good rating for Mouthwash as opposed to fair–good for Water in all cases) in favor of the Mouthwash for all questions (immediate dry mouth relief, lubricating effects, moisturizing effects) (p<0.0001 for all comparisons). Consistent results were observed for participants with and without SS (p<0.005 for all comparisons) (Table 4).
Table 4 Study 1 PPAQ: Difference in adjusted mean score between Mouthwash and Water (ITT population).
| Questions |
All participantsa,b (N=55) |
Participants with SSa,c (N=22) |
Participants with SSa,c (N=33) |
| Difference in score, 95% CI, p-value |
| 1. Having an immediate dry mouth relief |
0.9 (0.5, 1.3) p<0.0001 |
1.1 (0.5, 1.7) p=0.0008 |
0.8 (0.3, 1.3) p=0.0020 |
| 2. Having an immediate lubricating effect |
1.1 (0.7, 1.5) p<0.0001 |
1.1 (0.5, 1.7) p=0.0011 |
1.2 (0.7, 1.7) p<0.0001 |
| 3. Having an immediate moisturizing effect |
1.1 (0.7, 1.6) p<0.0001 |
1.4 (0.7, 2.1) p=0.0001 |
0.9 (0.4, 1.5) p=0.0012 |
Scale is measured from 1 (poor) – 5 (excellent).
aDifference is Mouthwash minus Water, such that a positive difference favors the Mouthwash.
bOverall group estimates obtained from ANOVA with factors for period, treatment as fixed effects and participant as a random effect.
cSubgroup estimates obtained from ANOVA with factors for period, treatment, SS and treatment by SS interaction as fixed effects and participant as a random effect.
Exploratory efficacy variables: Mucosal wetness, saliva film thickness, and level of moistness (Table 5 and Figure 4) Overall, there were no statistically significant changes in mucosal wetness and saliva film thickness in either group from pretreatment use to post-treatment use. However, for participants with SS receiving water, mucosal wetness and saliva film thickness significantly decreased post-treatment use (p=0.0307 and p=0.0308, respectively), whereas for those without SS receiving water, mucosal wetness and saliva film thickness significantly increased post-treatment use (p=0.0025 for both variables). There were statistically significant differences in the subjective level of moistness before and after the Mouthwash use in the overall population and both the SS and non-SS subgroups (p<0.0001 for all). There were no statistically significant betweentreatment differences in the water group overall and for those with SS, but there was a significant increase for participants without SS (p=0.0183).
Table 5 Study 1: Change in mucosal wetness, saliva film thickness and moistness (ITT population).
| |
All participantsa,b (N=55) |
Participants with SSb,c (N=22) |
Participants without SSb,c (N=33) |
| Mouthwash |
Water |
Mouthwash |
Water |
Mouthwash |
Water |
| |
Adjusted mean of change from pre- to post-treatment use (SE) [95% CI] p-value |
| Mucosal wetness (μl) |
0.083 (0.0660)
[-0.048, 0.214]
p=0.2129 |
0.037 (0.0642)
[-0.090, 0.165]
p=0.5641 |
0.084 (0.1103)
[-0.135, 0.303]
p=0.4489 |
-0.228 (0.1038)
[-0.434, -0.022]
p=0.0307 |
0.140 (0.0828)
[-0.025, 0.304]
p=0.0947 |
0.257 (0.0828)
[0.093, 0.421]
p=0.0025 |
| Saliva film thickness (μm) |
2.1 (1.65)
[-1.2, 5.4]
p=0.2102 |
0.9 (1.61)
[-2.3, 4.1]
p=0.5667 |
2.1 (2.77)
[-3.4, 7.6]
p=0.4540 |
-5.7 (2.61)
[-10.9, -0.5]
p=0.0308 |
3.5 (2.08)
[-0.6, 7.7]
p=0.0906 |
6.4 (2.08)
[2.3, 10.6]
p=0.0025 |
| Level of moistnessd |
1.1 (0.13)
[0.9, 1.4]
p<0.0001 |
0.2 (0.13)
[-0.1, 0.4]
p=0.1327 |
1.2 (0.20)
[0.8, 1.6]
p<0.0001 |
-0.1 (0.20)
[-0.4, 0.3]
p=0.7733 |
-
- (0.16)
[0.8, 1.4]
p<0.0001 |
0.4 (0.16)
[0.1, 0.7]
p=0.0183 |
aOverall group estimates obtained from ANCOVA with factors for period, treatment and SS status as fixed effects, participant as a random effect, and participant-level pre-treatment and period minus participant-level pre-treatment values as covariates.
bP-value testing for a non-zero change.
cSubgroup estimates obtained from ANCOVA with factors for period, treatment, SS status and treatment by SS status interaction as fixed.
effects, participant as a random effect, and participant-level pre-treatment and period minus participant-level pre-treatment values as covariates. dLevel of moistness measured on a scale from Scale is measured 1 (poor) to 5 (excellent).
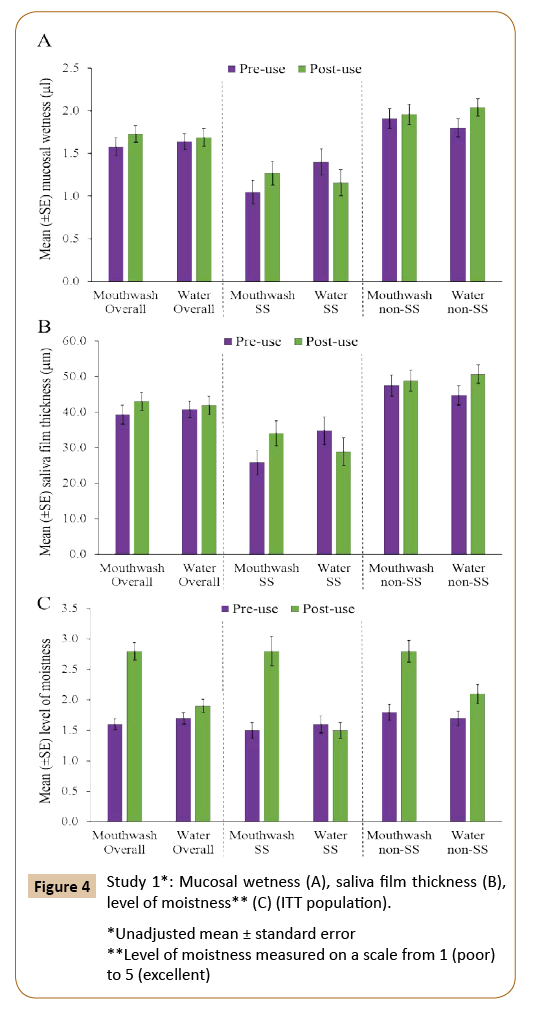
Figure 4: Study 1*: Mucosal wetness (A), saliva film thickness (B), level of moistness** (C) (ITT population).
Study 2
PPUSQ: On Days 1, 3 and 8, there were statistically significant between-treatment differences in favor of Water in response to Question 3 (gentleness; p<0.05) and in favor of Mouthwash in response to Question 4 (freshness; p<0.005). There were almost no statistically significant between-treatment differences in response to Questions 1 (overall liking) and 2 (pleasantness) except for the pleasantness of the treatment in favor of Mouthwash on Day 3 (p=0.0170) (Table 6).
Table 6 Study 2 PPUSQ: Difference in adjusted mean score between Mouthwash and Water-only (ITT population).
| |
Day 1a,b |
Day 3a,b |
Day 8a,b |
| |
Difference (95% PI) p-value |
| 1. How much you liked the product overall |
-0.21 (-0.67, 0.25) p=0.3595 |
0.11 (-0.36, 0.58)
p=0.6347 |
0.03 (-0.42, 0.48)
p=0.8883 |
| 2. How pleasant would you say the flavor of the product was? |
0.23 (-0.27, 0.73)
p=0.3634 |
0.58 (0.11, 1.05)
p=0.0170 |
0.16 (-0.32, 0.65)
p=0.5014 |
| 3. How gentle would you say the product was? |
-0.56 (-1.06, -0.05)
p=0.0306 |
-0.54 (-1.00,-0.08)
p=0.0206 |
-0.57 (-1.03,-0.11)
p=0.0161 |
| 4. How fresh your mouth felt after using the product? |
0.73 (0.29, 1.17)
p=0.0013 |
0.71 (0.26, 1.16)
p=0.0021 |
0.89 (0.46, 1.33)
p<0.0001 |
CI: Confidence Interval; PPUSQ: Post-Product Use Sensory Questionnaire; SS: Sjögren's Syndrome.
aDifference is Mouthwash minus Water such that a positive difference favors the Mouthwash.
bFrom ANOVA model with factors for treatment and confirmed Sjögren’s syndrome status stratification using Observed Margins option.
Safety: In Study 1, the only reported treatment-emergent AE (TEAE) was a non-oral cyst in one participant in the Mouthwash group, which was considered unrelated to study treatment and mild in intensity; this was resolved by study completion. In Study 2, there were 19 TEAEs in the Mouthwash group, reported by 12 participants, 16 of which were oral TEAEs. There were eight treatment-related TEAEs: three reports of ‘paresthesia oral’ in two participants, three reports of ‘oral discomfort’ in one participant, and two reports of ‘throat irritation’ in one participant. In the Water-only group, there were six TEAEs reported by four participants, three of which were oral; none of the TEAEs were considered treatment-related. All AEs were mild or moderate in intensity.
Discussion
Despite wide inter-individual variation in salivary flow rates in medication-induced salivary hypofunction, it has been shown that dry mouth symptoms develop when the unstimulated salivary flow rate decreases to approximately one-half of the baseline value [26]. In the wider population, decline in salivary flow usually occurs gradually, making the affected person less aware and more likely to accommodate their oral dryness. This necessitates professional intervention to manage and prevent further oral complications. A recent Sjögren’s Syndrome Foundation survey of their members reported that 74% of 2692 individuals with SS encounter significant emotional burden to their life and 96% want additional treatment for their disease [27].
Stimulation alone will not provide enough saliva to protect the oral mucosa. People with severe salivary hypofunction, especially those with SS and those treated with head and neck radiation therapy, use water as their most frequent means of relieving dryness [14,15]. While water may provide some immediate symptomatic relief, frequent use may dilute the salivary proteins, buffers, and minerals necessary for maintaining pH, oral tissue health, and enamel remineralization [12,16]. Approaches that moisturize the mouth and decrease discomfort can be synergistic with therapeutic agents that increase gland secretion, such as secretogogues and polyol chewing gum [28]. When a protective layer of saliva is reduced or absent or the salivary composition is altered, the oral mucosa can become friable and atrophic, thereby increasing its vulnerability to irritation, abrasion and infection [29,30]. It is therefore important to consider the oral vulnerability of individuals with dry mouth when developing treatments for symptom relief. One observational study found that in a group of people with xerostomia using antiseptic mouthwashes predominantly containing quaternary ammonium compounds, the symptoms of xerostomia worsened after 2 weeks’ use [13].
The two studies reported here evaluated subjective sensory perception of an experimental mouthwash formulated with moisturizing ingredients including CPC as a preservative in relieving dry mouth symptoms. While CPC is used extensively as a preservative in mouth rinses, there is very limited clinical data on its acceptability within the population of individuals with dry mouth. This study population included healthy individuals with a subjective complaint of dry mouth as well as those with confirmed SS and self-reported dry mouth. Efficacy was assessed in Study 1 using the PPAQ immediately after treatment exposure. The results were consistent with those previously reported from Study 2 [21], demonstrating that the Mouthwash was significantly more effective than Water-only at providing immediate dry mouth relief, lubrication and moisturization.
Overall, most participants found that the gentleness of the experimental Mouthwash was similar to Water (primary endpoint) and the majority liked the Mouthwash and its flavor and would continue using it. This is important, as flavor is an aspect that influences treatment perception regarding gentleness [31,32]. In general, subgroup analyses performed according to confirmed SS status in Study 1 were consistent with the overall study population; however, it is interesting that a smaller proportion of those with SS than those without SS ‘Agreed’ or ‘Strongly agreed’ that the Mouthwash was gentle. This may be reflective of the oral sensitivity and mucosal alterations seen specifically in SS [3].
Most participants found that the experimental Mouthwash was associated with moisturizing, soothing, and refreshing sensations immediately and after 30 minutes of use, consistent with results previously reported [21]. Just over half of participants had a tingling sensation immediately after Mouthwash use, but fewer than 20% experienced the treatment as numbing, burning or drying out. As mentioned earlier, hyposalivation could make the oral mucosa susceptible to experiencing tingling, numbing and burning sensations. These sensations have previously been reported as AEs with the mouthwash formulations so were not unexpected here.
The sensory attributes of the Mouthwash were further confirmed in Study 2, using the PPUSQ. On Day 8 of use, there were no significant differences between groups randomized to Mouthwash or Water-only in terms of how much they liked the treatment or how pleasant they considered the flavor to be. Water, as expected, was shown to be gentler than the Mouthwash. A possible explanation for this is that water does not contain any additives that could be deemed as potentially irritating to the oral mucosa in contrast to the Mouthwash, which has additional excipients that may cause possible irritation to the oral mucosa such as the preservative system and the flavor. Participants did consider the Mouthwash to give a greater feeling of freshness than Water.
Study 1 additionally looked at objective measures of mucosal wetness and saliva film thickness but did not find any overall statistically significant changes after use of either treatment. However, following Water use statistically significant decreases were seen in those with SS with increases seen in those without SS. In contrast, moistness level increased with Mouthwash, overall and in both subgroups, but only in the non-SS group with Water. Further investigation could be carried out to examine why there were differences according to SS status.
Based on the AE profile of the Mouthwash in both the studies, this treatment can be considered as generally well tolerated. One limitation of these studies is that, although participants were not directly informed of the treatment they were given, blinding was not fully possible due to the observed differences between the Mouthwash and Water.
Conclusion
In conclusion, these studies indicate that individuals with a subjective feeling of dry mouth, both with and without a diagnosis of SS, perceived the experimental moisturizing Mouthwash to be gentle, moisturizing, soothing and refreshing, with most participants indicating that they would continue to use the Mouthwash.
Acknowledgements
The authors thank all participants and study site staff. They also thank Guillaume Frappin of GSK Consumer Healthcare for assistance with manuscript data checking. Statistical analysis was provided by Avinash Patil of Syneos Health and Darren Targett of GSK Consumer Healthcare. Editorial assistance with the preparation of manuscript drafts was provided by Juliette Allport of Leading Edge Medical Communications Ltd, Loudwater, UK and Eleanor Roberts of Beeline Science Communications, Ltd., UK, both funded by GSK Consumer Healthcare.
Funding
This study was funded by GSK Consumer Healthcare.
Competing Interests
Jose A and Varghese R are employees of GSK Consumer Healthcare. Singh M, Magnuson B, Farag A, Kafasis N, Tzavaras E and Papas A are employees of Tufts University School of Dental Medicine, which has received funding from GSK Consumer Healthcare.
References
- Orellana MF, Lagravere MO, Boychuk DG, Major PW, Flores-Mir C (2006) Prevalence of xerostomia in population-based samples: a systematic review. J Public Health Dent 66: 152-158.
- Thomson WM (2005) Issues in the epidemiological investigation of dry mouth. Gerodontology 22: 65-76.
- Cartee DL, Maker S, Dalonges D, Manski MC (2015) Sjogren's syndrome: oral manifestations and treatment, a dental perspective. J Dent Hyg 89: 365-371.
- Fox RI (1996) Sjogren's syndrome: immunobiology of exocrine gland dysfunction. Adv Dent Res 10: 135-140.
- Wiener RC, Wu B, Crout R, Wiener M, Plassman B, et al. (2010) Hyposalivation and xerostomia in dentate older adults. J Am Dent Assoc 141: 279-284.
- Garg AK, Malo M (1997) Manifestations and treatment of xerostomia and associated oral effects secondary to head and neck radiation therapy. J Am Dent Assoc 128: 1128-1133.
- Wolff A, Joshi RK, Ekstrom J, Aframian D, Pedersen AM, et al. (2017) A guide to medications inducing salivary gland dysfunction, xerostomia, and subjective sialorrhea: A systematic review sponsored by the World Workshop on Oral Medicine VI. Drugs R D 17: 1-28.
- Cappetta K, Beyer C, Johnson JA, Bloch MH (2017) Meta-analysis: Risk of dry mouth with second generation antidepressants. Prog Neuropsychopharmacol Biol Psychiatry 84: 282-293.
- Tan EC, Lexomboon D, Sandborgh-Englund G, Haasum Y, Johnell K (2017) Medications that cause dry mouth as an adverse effect in older people: A systematic review and metaanalysis. J Am Geriatr Soc 66: 76-64.
- Singh ML, Papas A (2014) Oral implications of polypharmacy in the elderly. Dent Clin North Am 58: 783-796.
- Torres SR (2014) Oral features of graft-versus-host disease. Rev Bras Hematol Hemoter 36: 9-11.
- Cassolato SF, Turnbull RS (2003) Xerostomia: clinical aspects and treatment. Gerodontology 20: 64-77.
- Chevalier M, Sakarovitch C, Precheur I, Lamure J, Pouyssegur-Rougier V (2015) Antiseptic mouthwashes could worsen xerostomia in patients taking polypharmacy. Acta Odontol Scand 73: 267-273.
- Frost PM, Shirlaw PJ, Walter JD, Challacombe SJ (2002) Patient preferences in a preliminary study comparing an intra-oral lubricating device with the usual dry mouth lubricating methods. Br Dent J 193: 403-408.
- Simons D (1996) Chewing gum: trick or treat? A review of the literature. Dent Update 23: 162-169.
- Kaidonis J, Townsend G (2016) The 'sialo-microbial-dental complex' in oral health and disease. Ann Anat 203: 85-89.
- Papas AS, Sherrer YS, Charney M, Golden HE, Medsger Jr. TA, et al. (2004) Successful treatment of dry mouth and dry eye symptoms in Sjögren’s syndrome patients with oral pilocarpine: a randomized, placebo-controlled, dose-adjustment study. J Clin Rheumatol 10: 169-177.
- Fox PC, Singh ML, Papas AS (2011) Treatment of Dry Mouth. In: Wallace (ed.) The Sjögren’s book. Oxford: Oxford University Press. pp. 210-209.
- Jose A, Atassi M, Shneyer L, Cronin M (2017) A randomized clinical trial to measure mouth moisturization and dry mouth relief in dry mouth subjects using dry mouth products. J Clin Dent 28: 32-38.
- Jose A, Siddiqi M, Cronin M, DiLauro TS, Bosma ML (2016) A randomized clinical trial in subjects with dry mouth evaluating subjective perceptions of an experimental oral gel, an oral rinse and a mouth spray compared to water. Am J Dent 29: 58-64.
- Jose A, Singh ML, Magnuson B, Farag A, Varghese R, et al. (2018) A randomized controlled study to evaluate an experimental moisturizing mouthwash formulation in participants experiencing dry mouth symptoms.
- Vitali C, Bombardieri S, Jonsson R, Moutsopoulos HM, Alexander EL, et al. (2002) Classification criteria for Sjögren’s syndrome: a revised version of the European criteria proposed by the American-European Consensus Group. Ann Rheum Dis 61: 554-558.
- Shiboski CH, Shiboski SC, Seror R, Criswell LA, Labetoulle M, et al. (2017) 2016 American College of Rheumatology/European League Against Rheumatism classification criteria for primary Sjögren’s syndrome: A consensus and data-driven methodology involving three international patient cohorts. Ann Rheum Dis 76: 9-16.
- Fisher BA, Jonsson R, Daniels T, Bombardieri M, Brown RM, et al. (2017) Standardisation of labial salivary gland histopathology in clinical trials in primary Sjogren's syndrome. Ann Rheum Dis 76: 1161-1168.
- Osailan S, Pramanik R, Shirodaria S, Challacombe SJ, Proctor GB (2011) Investigating the relationship between hyposalivation and mucosal wetness. Oral Dis 17: 109-114.
- Wolff M, Kleinberg I (1998) Oral mucosal wetness in hypo- and normosalivators. Arch Oral Biol 43: 455-462.
- Sjögren’s Syndrome Foundation (2017) Living with Sjögren’s. Summary of major findings.
- Zero DT, Brennan MT, Daniels TE, Papas A, Stewart C, et al. (2016) Sjögren’s Syndrome Foundation clinical practice guidelines. Clinical practice guidelines for oral management of Sjögren disease: Dental caries prevention. J Am Dent Assoc 147: 295-305.
- Fox PC, van der Ven PF, Sonies BC, Weiffenbach JM, Baum BJ (1985) Xerostomia: evaluation of a symptom with increasing significance. J Am Dent Assoc 110: 519-525.
- Sreebny LM, Valdini A (1987) Xerostomia. A neglected symptom. Arch Int Med 147: 1333-1337.
- Glass BJ, Kuhel RF, Langlais RP (1986) Treatment of common orofacial conditions. Dent Clin North Am 30: 421-446.
- Ettinger RL (1981) Xerostomia--a complication of ageing. Aust Dent J 26: 365-371.