Virendra Sehgal N2*, Naresh Sehgal2, Ruchi Sehgal2, Deepa Sehgal2 and Ananta Khurana1
1Dermato-Venereology (Skin/VD) Center, Sehgal Nursing Home, Panchwati, Delhi, India
2Department of Dermatology, Dr RML Hospital and Postgraduate Institute of Medical Education and Research (PGIMER), New Delhi, India
*Corresponding Author:
Virendra Sehgal N
Department of Dermatology
Dr RML Hospital and Postgraduate Institute of Medical Education and Research (PGIMER)
New Delhi, India
E-mail: drsehgal@ndf.vsnl.net.in (or) sehgalvn@yahoo.co.in
Received date: April 26, 2016; Accepted date: May 23, 2016; Published date: May 30, 2016
Citation: Virendra Sehgal N, Sehgal N, Sehgal R, et al. Role of Pro-Anthocyanidin in Gynecomastia and Related Oligospermia and Asthenospermia. Clin Pediatr Dermatol. 2016, 2:2 Doi: 10.21767/2472-0143.100019
Keywords
Asthenospermia; Gynecomastia; Oligospermia
Introduction
Gynecomastia [1] /?ga?n?k?'mæsti?/ is a common endocrine disorder in which there is a benign enlargement of breast tissue in males [2,3]. Most adolescent boys, up to 70%, [4,5] have some breast development during puberty [2]. Newborn and adolescent males frequently experience temporary gynecomastia due to the influence of maternal hormones and hormonal changes during puberty, respectively. The treatment options [5] are too few and far between, proanthocyanidin seems a plausible alternative.
Patient and methods
A 15 year-old-student had reported on March 28, 2009 with asymptomatic, insidiously enlarging swelling in and around both the nipples for the past couple of years so much so it acquired the size of the breast or gynecomastia (Figure 1). There were neither nocturnal emissions of seminal fluid while asleep nor was there semblance of any hair growth. Weak orgasm was not pleasurable. There was absence of hair above the upper lip and chin, the secondary sexual characters. Pubic hairs were scanty. The penis was small. Testes too were small and soft. His height was 170.18 centimeter while weight was 65 Kg.
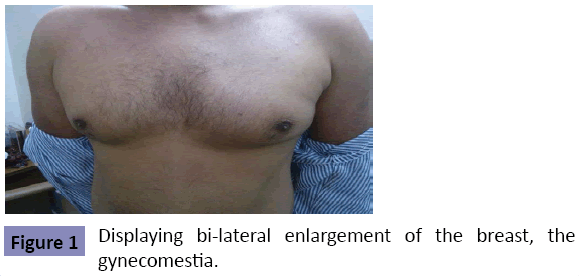
Figure 1: Displaying bi-lateral enlargement of the breast, the gynecomestia.
Ultrasonography of the scortum: Right testes measured 50 × 24.8 mm, while left testes measured 48 × 20.7 mm. Both the testes had uniformaly reduced echogenecity. Neither calcification nor para-testicular fluid was seen in either of the testes, suggesting bilatral testicular atrophy.
The semen analysis [5] and hormonal profile [6] was done on regular interval starting from the day of reporting to evaluate its status, the synopsis of which are portrayed in the adjoining Tables 1 and 2. He was administered proanthocyanidin (GRAVINOl) orally in the doses of 150 mg a day in two equal divided doses of 75 mg each for a period of three months. Follow up was done every month for first 3 months, every three months for 6 months, every six months for a year, every year for 2, 3 and 4 years respectively. During the period in addition to physical checkup semen analysis and hormonal profile was also undertaken at regular intervals (Tables 1 and 2) at the end of 4 years treatment, a substantial change in his phyque was apparent. The growth of hair on the upper lip, chin, beard and pubic area were striking so also was his current height (190.5 centimeter) and weight (95 kg). There was marked improvement in gynecomastia, low sperm count (oligospermia) and low motility (asthenospermia) on semen analysis (Table 1).
Period of Abstinence
<3 days |
Results
2009 |
Results
2012 |
Results
2014 |
Range |
Units |
Biological Reference Interval |
| Time of collection |
2:52 PM |
13:55 PM |
3:50PM |
- |
- |
- |
| Volume |
4.5 |
4.0 |
3.5 |
- |
ml |
1.5-6.8 |
| PH |
Alkaline |
Alkaline |
8.0 |
7.0-8.0 |
|
> or =7.2 |
| Color |
Whitish |
Whitish |
Gray-white |
- |
- |
- |
| Liquifaction |
30 |
- |
70 |
|
Minutes |
High 15-60 |
| Viability |
Low 40 |
- |
72 |
50-100 |
% |
> or =58 |
| Motility |
50 |
50 |
42 |
50-100 |
|
> or = 40 |
| Motility-Grade 0 |
50 |
50 |
28 |
|
% |
Low 32-72 |
| Motility-Grade 1&2 |
40 |
20 |
14 |
- |
% |
1-18 |
| Motility-Grade 3&4 |
10 |
30 |
58 |
- |
% |
22-59 |
| Sperm Count |
Low 02 |
45 |
38 |
20.0-150.0 |
Mill/ml |
15-213 |
| Abnormal Forms |
10 |
- |
13 |
0-20 |
% |
- |
| Head |
05 |
- |
8 |
- |
% |
- |
| Pin Heads |
02 |
- |
2 |
- |
% |
- |
| Giant Heads |
02 |
- |
1 |
- |
% |
- |
| Double Heads |
01 |
- |
0 |
- |
% |
- |
| Neck |
02 |
02 |
- |
- |
|
- |
| Bent |
01 |
01 |
- |
- |
% |
- |
| CYT(Cytoplasm) |
01 |
01 |
- |
- |
% |
- |
| Tail |
03 |
03 |
5 |
- |
% |
- |
| Short Tail |
01 |
01 |
1 |
- |
% |
- |
| Curled Tail |
02 |
02 |
- |
- |
% |
- |
| Red Cells |
0-1 |
- |
Not Detected |
Not detected |
/hpf |
Not Detected |
| Pus Cells |
2-3 |
3-5 |
0-1 |
0-5 |
/hpf |
0-5 |
| Epithelial cells |
0-1 |
1-2 |
Not Detected |
0-5 |
/hpf |
0-5 |
| Crystal |
- |
- |
Not Detected |
- |
- |
Not Detected |
| Amorphous Deposit |
- |
- |
Not Detected |
- |
- |
Not Detected |
| Bacteria |
- |
- |
Not Detected |
- |
- |
Not Detected |
Table 1: Semen Analysis.
| Hormones Method: Chemiluminescence |
March.28, 2009 |
Aug. 4, 2010 |
Dec.30, 2014 |
Biological Reference Interval |
| Follicle Stimulating Hormone(F.S.H) |
3.58 mIµ/ml |
2.36 mIµ/ml |
2.76 mIµ/ml |
1.40-18.10 |
| Luteinising Hormone(L.H) |
3.16 mIµ/ml |
8.06 mIµ/ml |
6.01 mIµ/ml |
1.50-9.30 |
| Prolactin |
14.09 ng/ml |
12.40 ng/ml |
6.30 ng/ml |
2.10-17.70 |
| Testosterone |
12.76 ng/ml |
207.78 ng/ml |
467.40 ng/ml |
241.00-827.00 |
Table 2: Hormonal Profile.
Discussion
Pharmacokinetics
Proanthocyanidins (pycnogenol), are a class of polyphenols, discovered, developed and patented for the extraction of oligomeric proanthocyanidins from pine bark and grape seeds for the first time in the year 1947 by Jacques Masquelier [7]. They are oligomeric flavonoids [8], many of which are catechin and epicatechin, and their gallic acid esters. Colorless proanthocyanidins are a strictly defined group of 3 flavanols naturally occurring as a mix of monomers, di-mers, and tri-mers of the catechin building block, which is a 4 × -hydroxylation of the flavan-3-olcore.
Mode of action
Proanthocyanidin (Pycnogenol), a type of flavonoid and antioxidant is found in the skin of fruits and vegetables. It plays an important role in blood vessels, and helps in stabilizing collagen [9,10] and maintenance of elastin [11] within the body. Collagen and elastin are the two principle proteins, which are used in the formation of connective tissue in the body. In addition, it inhibits platelet aggregation and vascular constriction; thus preventing stroke [12-15]. Furthermore, it increases intracellular vitamin c levels, scavenges oxidants and free radicals. Hence it inhibits destruction of collagen. Besides, sleepiness, loss of appetite, skin rashes, nausea and itching are its adverse reactions. It is contraindicated in those with known hypersensitivity to grape seed. Its safety and efficacy in pregnancy and lactation is lacking. Concomitant administration of Proanthocyanidin, and vitamin C should be avoided in hypertensive, for it may result in increase in blood pressure.
However, the precise mode of action of proanthocyanidin is speculative in gynaecomestia and related changes in the semen and hormonal undertones. It seems to be a vital growth factor in which interplay of some or all modes of action (vide supra) may participate. Further research on its probable mode of action at the molecular level, may provide a promising treatment option for gynecomastia and delayed puberty in males. Besides, it might prove useful in hair growth in male [16] and female [17] pattern androgenetic alopecia and erectile dysfunction (ED) [18]. The combine therapy of pro-anthrocynidin and L-arginine [19], in erectile dysfunction, in particular, is currently a topic of intriguing dialogue, warranting perspective studies.
References
- Oxford Dictionary (2016) Gynaecomastia -definition of gynaecomastia in English from the Oxford dictionary. Accessed on: 2016-01-20.
- Niewoehner CB, Schorer AE (2008) Gynaecomastia and breast cancer in men. BMJ 29: 709-713.
- Shulman DI, Francis GL, Palmert MR Eugster EA (2008) Use of aromatase inhibitors in children and adolescents with disorders of growth and adolescent development. Pediatrics 121: e975-983.
- Launow E, Kettler M, Slanetz PJ (2011) Spectrum of disease in the male breast. AJR 196: W247-259.
- Narula HS, Carlson HE (2014) Gynaecomastia-pathophysiology, diagnosis and treatment. Nat Rev Endocrinol 10:684-698.
- Cooper TG, Noonan E, Auger J, Baker HW, Behre HM, et al. (2010) World Health Organization reference values for human semen characteristics. Human reproduction updates 16: 231-245.
- Rauhut R, Michael M (1985) Chemiluminescence Kirk-Othmer Concise Encyclopedia of Chemical Technology. John Wiley and Sons, p: 247.
- Masquelier J, Michaud J, Laparra J, Dumon MC (1979) Flavonoids and pycnogenols. Int J Vitam Nutr Res49:307-311.
- Masquelier J, Dumon MC, Dumas J (1981) Stabilization of collagen by procyanidolic oligomers. Acta Ther7:101-105.
- Kuttan R, Donnelly PV, Di Ferrante N (1981) Collagen treated with (+)-catechin becomes resistant to the action of mammalian collagenase. Experientia 15:221-223.
- Tixier JM, Godeau G, Robert AM, Hornebeck W (1984) Evidence by in vivo and in vitro studies that binding of pycnogenols to elastin affects its rate of degradation by elastases. Biochem Pharmacol 15: 3933-3939.
- Sonia de Pascual-Teresa, Diego MorenoA, Cristina García-Viguera (2010)Flavanols and Anthocyanins in Cardiovascular Health: A Review of Current Evidence. Int J Mol Sci 11: 1679-1703.
- Maffei Facino R, Carini M, Aldini G (1994) Free radicals scavenging action and anti-enzyme activities of procyanidines from Vitis vinifera. A mechanism for their capillary protective action. Arzneimittelforschung44:592-601.
- Bagchi D, Kuszynski C, Balmoori J (1998) Hydrogen peroxide-induced modulation of intracellular oxidized states in cultured macrophage J774A.1 and neuroactive PC-12 cells, and protection by a novel grape seed proanthocyanidin extract 12:8-568.
- Preuss HG, Wallerstedt D, Talpur N, Tutuncuoglu SO, Echard B, et al. (2000) Effects of niacin-bound chromium and grape seed proanthocyanidin extract on the lipid profile of hypercholesterolemic subjects: a pilot study. J Med 31:227-246.
- Sehgal VN, Aggarwal AK, Srivastava G, Rajput P (2006) Male Pattern Androgenetic Alopecia. Skin med 5:128-135
- Sehgal VN, Srivastava G, Aggarwal AK, Midha R (2013) Hair biology and its comprehensive sequence in female pattern baldness: diagnosis and treatment modalities-Part I. Skinmed 11:39-45.
- Sehgal VN, Srivastava G (2003)Erectile dysfunctions. Skinmed2:350-356.
- Stanislavov R, Nikolova V (2003) Treatment of erectile dysfunction with Pycnogenol and L-arginine. J Sex Marital Ther 29: 207-213.

