Marianna K Baum1, Adriana Campa1, J Bryan Page4, Shenghan Lai5, Lesedi Tsalaile2, Sabrina Sales Martinez1, Patricia Burns3, O’Dale Williams1, Yinghui Li1, Erik van Widenfelt2, Herman Bussmann2, Moyo Sikhulele2, Joseph Makhema2, Myron Essex3, Richard Marlink3, Dikotlana Study Team2
Florida International University, Robert Stempel College of Public Health and Social Work, Miami, Florida, USA
Botswana Harvard Partnership, Gaborone, Botswana
Harvard School of Public Health, Boston, Massachusetts, USA
University of Miami, School of Medicine, Miami, Florida, USA
Johns Hopkins University, School of Medicine, Baltimore, Maryland, USA
*Corresponding Author:
Marianna K Baum
Florida International University
Robert Stempel College of Public Health and Social Work
11200 SW 8 Street, AHC-5 Room 327
Miami, Florida 33199, USA.
Tel: 305-348-2871
Fax: 305-348-0383
E-mail: baumm@fiu.edu.
Received date: November 21, 2015 Accepted date: December 01, 2015 Published date: December 08, 2015.
Citation: Baum MK, Campa A, Page JB, et al. Recruitment, Follow-Up and Characteristics of HIV Infected Adults who Use Illicit Drugs in Southern Africa. J Drug Abuse. 2015, 1:1.
Keywords
Marijuana; Benzodiazepines; Botswana; HIV; Recruitment; Nutritional status, HIV disease progression
Introduction
The majority of the world’s current HIV infected cases occur in Sub-Saharan Africa, which is reporting hyperendemic proportions of the epidemic; in particular, Botswana has one of the worst HIV prevalence rates estimated at 25% [1,2]. Great strides have been made in stemming the epidemic with the introduction of universal antiretroviral therapy (ART) [3], decreasing the death rates in some of the hardest-hit countries in Africa [4]. Various HIV prevention strategies have been used successfully, but populations who use illicit drugs are difficult to reach, particularly in developing countries, due to stigma associated with both HIV positivity and illicit drug use. Therefore, these populations are of particular interest [1]. Drug use has not been adequately studied in Sub-Saharan Africa, especially in countries such as Botswana where the effect of drug use on HIV transmission has been considered minimal [5]. While the illegality of cannabis in most countries precludes an accurate estimation of its use, Sub-Saharan Africa has one of the lowest prevalence rates in the world [6,7]. Use of cannabis however, contributes to HIV transmission [8,9], disability, and is associated with higher mortality, and thus, needs to be considered [6]. Benzodiazepines, on the other hand, are the most commonly prescribed medication for a range of medical conditions [10], are also available over the counter in Southern Africa, and are frequently misused [11]. Benzodiazepines are frequently the primary drug of abuse, primarily in females aged older than 40 years [11], and their use is associated with psychological and physiological dependence [12].
The theme of the 20th International AIDS conference was “Stepping up the Pace” reflecting the principle of inclusiveness of key affected populations in “hotspots,” which were defined as geographic areas of high HIV incidence and prevalence [13]. Botswana is one of the HIV “hotspots” and the first resourcelimited country in Africa that was involved in a large-scale effort to provide universal ART [2]. Nevertheless, to conquer the HIV epidemic in Botswana, it is critical to reach all groups who are at high risk for HIV infection. HIV infected persons in the general population have largely been identified and have been receiving ART [14,15]. One of the factors that has impeded greater coverage has been the difficulty in reaching and engaging persons who use illicit drugs [16-19], due to criminalization and a dual stigma associated with HIV positive status and the use of illegal drugs [20,21]. Illicit drug use is related to unsafe sexual practices and an increased risk for HIV infection [8]. In addition, the stigma associated with drug use is a powerful barrier to accessing healthcare, and for recruitment into scientific studies which are designed to address health and welfare issues of this population [22].
Marijuana contains a psychoactive ingredient, tetrahydrocannabinol (THC), which has been shown to suppress immune function [23] and may affect HIV disease progression, directly or indirectly [24,25]. The use of marijuana has also been reported to increase the risk for contracting HIV-infection [9]. A derivative of the drug has been recommended as an appetite stimulant in HIV infection, but, its effects on nutritional status and HIV disease progression are still controversial [25]. Over the counter use of benzodiazepines is of interest as its misuse was the primary problem for which patients sought substance abuse treatment service in South Africa [11]. The purpose of this study was to assess the recruitment, follow-up, HIV disease progression, nutritional status and retention of HIV–infected persons who use illicit drugs and were enrolled in a trial of micronutrient supplementation among HIV positive treatment-naïve patients in Botswana.
Method
Recruitment strategies
Several strategies were used to enhance outreach of the hard-toreach HIV-infected population that used illicit drugs. We obtained written assurances from the Botswana Ministry of Health to safeguard the confidentiality of the drug use reported by the study participants. Other strategies to identify HIV–infected persons who use illicit drugs included defining behavioral and geographic characteristics of the population, conducting focus-groups with health-care professionals from areas known for illicit drug use to evaluate the recruitment materials, utilizing mass media advertising for recruitment, and referrals from detoxification programs. Incentives for participation and adherence to study visits included free laboratory testing, clinical follow-up, and reimbursement for transportation.
The research team conducted a rapid assessment strategy [26] to target HIV-infected drug users in which we partnered with health-care workers serving a population known to include HIVinfected persons who used marijuana in Botswana, including a rural area of Mochudi and the capital of Botswana, Gaborone. These health care workers shared their local knowledge about the populations of interest and helped to develop and evaluate recruitment materials. Separately, HIV-infected persons who used illicit drugs also evaluated the recruitment strategy devised by the research team. The formulation of the strategy involved developing a profile of the HIV-infected drug-using population, including their locations, means of contacting them, and determining appropriate incentives for their participation. Mass media campaigns advertised the study recruitment within identified marijuana user clusters many of whom were likely to be HIV-infected, emphasizing confidentiality and benefits of HIV testing. Liaisons within the communities who used marijuana were identified to facilitate recruitment, and incentives for participation were provided. The identified HIV-infected persons who used illicit drugs were evaluated for eligibility to participate in a 2-year follow-up clinical trial of micronutrient supplementation described elsewhere [27].
Participants who did not use marijuana were recruited from the clinics where HIV testing and treatment occurs. All participants were eligible for the study if they were HIV seropositive, their CD4 cell count was >350 cells/μL and they were ART-naïve. Other criteria were a body mass index (BMI) >18 Kg/m2 for women and 18.5 Kg/m2 for men, age 18 years or older, and no current AIDSdefining conditions or history of AIDS-defining conditions. Women were excluded if pregnant or becoming pregnant during the study. When the participants became eligible for ART according to the standards in Botswana at the time, their study participation was discontinued and they were referred for antiretroviral treatment.
The study was conducted by the Florida International University in collaboration with the Harvard School of Public Health and the Botswana-Harvard Partnership in Gaborone, Botswana, from December 2004 until July 2009. The investigation was approved by the Institutional Review Boards of all three institutions, and monitored by a Data Safety Monitoring Board [27].
Assessments
To identify active drug users, we used two main strategies: (1) urine toxicology and history of drug and alcohol use with validated questionnaires [28,29] were performed at baseline and every 6 months in all the participants, and (2) use of the active outreach strategies described above to access the drug-user clusters. Illicit drugs were those that were detected in the urine of the participants but were not prescribed by physicians as confirmed by the medical charts.
At baseline and every three months, physical examination and medical history were performed by a trained nurse or physician, blood was drawn for assessment of CD4+ cell count, and dietary intake was determined using 24-hour food recalls conducted by trained interviewers. Quantitative estimates, using several 24- hour recalls, provided an estimate of a person’s diet. At baseline and every six months, blood was also drawn to evaluate HIV viral load, blood chemistry and plasma micronutrients. Medical history included inter-current health events and currently prescribed medications; a review of medical charts was used to verify prescriptions and determine changes in health status. Morbidity information was collected by questionnaires at screening, and at every monthly visit, and confirmed by documentation in the medical chart.
To take in account the difference in required caloric intake due to gender and age, we used a formula that estimates basal metabolic rate (BMR) [30] from bioimpedance measures, which takes into consideration gender, age, weight and height. Individual caloric requirement was estimated by multiplying BMR x Activity factor of 1.55 for asymptomatic HIV people [31,32]. We calculated the ratio of actual intake to individual requirement to create a variable that shows adequacy (≥ 1), or inadequacy (<1) and compared men who used THC with men who did not use drugs, and for women who used benzodiazepine compared to women who did not use drugs to investigate whether the differences between groups were due to gender, individual caloric requirements or types of drugs.
Biochemical assays
Urine was collected under observation at baseline and every six months. The American Biomedica Rapid Drug kits were used to determine the presence of amphetamines, barbiturates, benzodiazepines, cannabinoids, cocaine, methadone, methamphetamines, opiates, morphine, and tricyclic antidepressants.
Lymphocyte phenotype was determined with a four-color immunophenotyping panel of monoclonal antibodies. Differential counts were determined using a Sysmex XE-2100hematology instrument and corroborated with cytocentrifuge smears.
HIV-viral load was determined using an in-vitro nucleic acid amplification test (Amplicor reagents and protocol, Roche- Diagnostics, Branchburg, NJ). For quality assurance we used standard reference materials, and 5% of the samples underwent duplicate testing blinded to the laboratory personnel.
Plasma zinc (Zn) and selenium (Se) levels were determined by flame atomic absorption spectrophotometry [33,34]. Plasma vitamins A and E were determined by high performance liquid chromatography (HPLC) [35]. Folate levels were determined by microbiological assay using standardized procedures employing Lactobacillus casei [36].
Statistical analysis
Statistical analyses were performed with the use of SAS software (SAS 9.3, SAS Institute, Cary, NC). At baseline, the participants who used drugs were compared to those who did not use drugs for continuous variables with the Student t-test, non-parametric ANOVA and Wilcoxon rank-sum test, and for categorical variables with the Chi-Square and logistic regressions. Over time analyses used the Mixed Linear Models procedure controlling for age, gender, baseline CD4 cell count, baseline HIV viral load (log10 scale), and baseline BMI. All P-values reported were two-sided; statistical significance was defined as P<0.05. The data was censored on July 24, 2009, when the last scheduled 24-month visit was completed.
Results
This is a descriptive study of targeted outreach for HIVinfected persons who use illegal drugs from the Micronutrient Supplementation Study in Botswana, Africa [27]. Using the community outreach strategies for HIV-infected persons who use drugs, 138 HIV-infected marijuana users were identified who were willing to be pre-screened for eligibility for the study (Table 1). From this group, only 52 qualified for the study. The main two reasons for ineligibility among the HIV-infected persons who used marijuana were a CD4 cell count ≤ 350 cells/μL (18.1%), and BMI<18 Kg/m2 for women and 18.5 Kg/m2 for men (39.9%) as the goal of the study was to supplement micronutrients to those who were early in the HIV disease progression and were not wasting. Those who did not qualify for the study or were not willing to participate (4.3%) were referred for follow-up and treatment according to the Botswana’s guidelines at the time of the study. The great majority (92%) of the marijuana users admitted readily to using drugs and the reported frequency of weekly use was median 5.00 (IQR=2.0-12.0).
In comparison, participants who did not use marijuana were selected from HIV screening and treatment clinics in Botswana and at the time of screening for this study their HIV status and CD4 cell count were known; thus all of the participants who did not use drugs were HIV positive with CD4 cell count >350 cells/ μL, and BMI >18 Kg/m2 for women and 18.5 Kg/m2 for men. None of the participants considered drug non-users admitted using marijuana and were negative by urine screens for drugs.
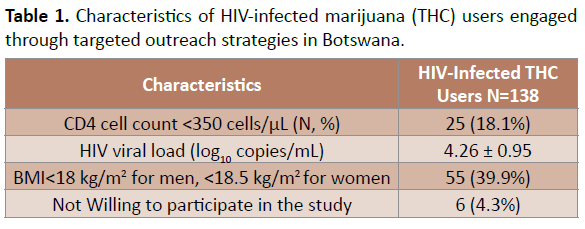
Table 1. Characteristics of HIV-infected marijuana (THC) users engaged through targeted outreach strategies in Botswana.
Several substances were identified during the follow-up of the study participants recruited from the HIV screening clinics. The urine drug screens identified use of benzodiazepines among 57 participants, 13 participants used opiates, 12 used tricyclic antidepressants, 7 used methamphetamine, 4 used amphetamines, and one participant used methadone. Review of the medical charts indicated that none of these substances were prescribed by physicians. None of the participants who were not specially recruited for their drug use however, used marijuana. Only two participants were positive for three types of drugs and one participant was positive for two illicit drugs, but neither one of these individuals were positive for marijuana. In the group that used benzodiazepines, three participants were excluded from the analyses because they used other drugs, mainly opiates.
As shown in Table 2, multivariate analyses indicate that participants who used marijuana were predominantly men (90.3% vs. 23.5% among drug non-users, P<0.001), and compared to those who did not use illicit drugs, had significantly lower BMI (21.8kg/m2 ± 3.7 vs. 24.3 kg/m2 ± 5.3, P=0.004), higher HIV viral load (4.36 log10 ± 0.89 vs. 4.09 log10 ± 0.89, P=0.018), higher kilocalorie intake (1924 Kcalories ± 1055 vs. 1620 Kcalories ± 926, P=0.025), consumed fewer number of meals/day (2.5 ± 0.5 vs. 2.8 ± 0.5, P=0.005, not shown in the table), tended to have higher protein intake (85.6 gm ± 59.1 vs. 72.9 gm ± 60.7, P= 0.15), had higher plasma levels of selenium (0.068 mg/dL ± 0.03 vs. 0.048 mg/dL ± 0.01, P= 0.032), and folate (14.5 ng/mL ± 5 vs. 10.6 ng/mL ± 9.8, P=0.009), and tended to have higher plasma zinc levels (0.85 mg/dL ± 0.47 vs. 0.60 mg/dL ± 1.14, P=0.092). Lower percentage of those who used marijuana were engaged in exercise or other physical activity than drug non-users (65.38% vs. 79.5%, P=0.016). Marijuana users were similar to drug non-users in age (33.5y ± 7.8 vs. 33.2y ±7.9, P =0.45), serum albumin levels (41.3mg/dL ± 4.9 vs. 41.19 mg/dL ± 4.7, P =0.842), CD4 cell count (477cell/μL ± 153 vs. 461 cell/μL ± 180, P=0.595), and plasma vitamins A (41.5 μg/dL ± 13 vs. 45.32 μg/dL ± 16.0, P=0.262) and E (8.1 μg/mL ± 1.9 vs. 9.8 μg/mL ± 5.1, P=0.075).
Among marijuana users, HIV viral load was significantly and inversely correlated with plasma albumin (r=-0.33, P=0.0047), and those with low plasma zinc (Zn<0.75 mg/L), and selenium levels (Se<0.065 mg/L) had significantly higher HIV viral load (P=0.004 and, P=0.036, respectively). When marijuana users were compared to non-users at different age ranges using nonparametric t-test, marijuana users who were 40 years or older had significantly more AIDS defining conditions (7/10) 71% than non-users (126/434) 29%, P=0.020 in the same age range. Alcohol use did not significantly affect these analyses.
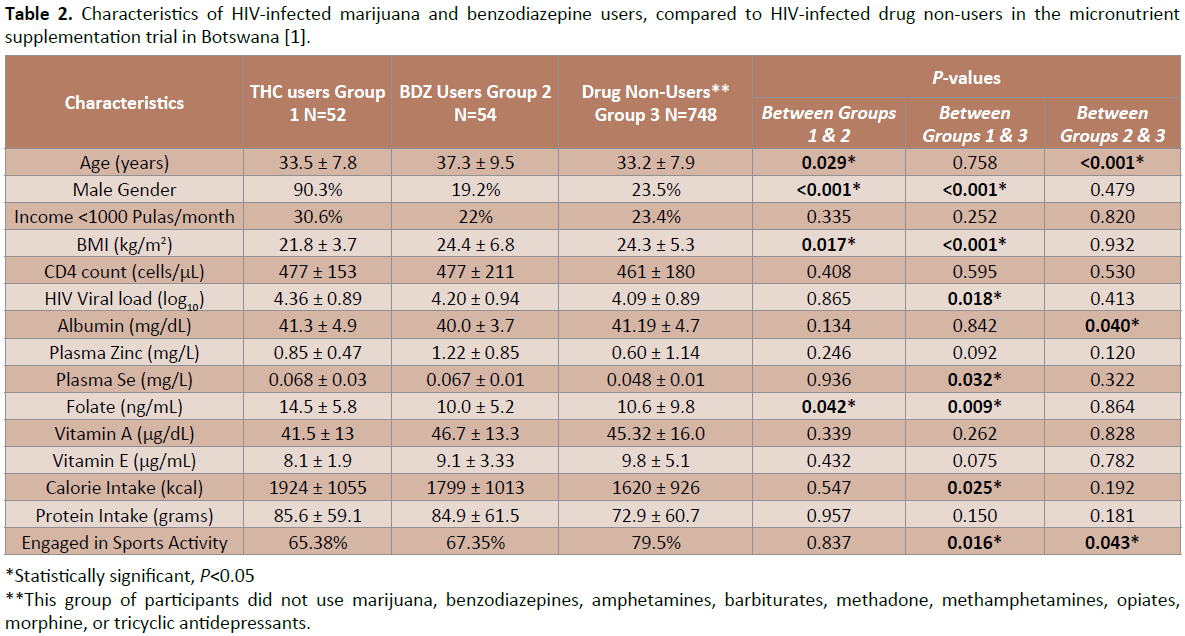
Table 2. Characteristics of HIV-infected marijuana and benzodiazepine users, compared to HIV-infected drug non-users in the micronutrient supplementation trial in Botswana [1].
Table 2 also shows that the participants who used benzodiazepines, as evidenced by a routine screening of urine for drugs during the study visits, were mainly females (80.8%), they were older than marijuana users (37.3 years ± 9.5 vs. 33.5 years ± 7.8, P<0.029), and were also older than drug non-users (37.3 years ± 9.5 vs. 33.2 years ± 7.9, P<0.001). Benzodiazepine users had higher BMI than marijuana users (24.4 kg/m2 ± 6.8 vs. 21.8 ± 3.7 kg/ m2, P=0.017), but the BMI of the benzodiazepine users was not different from the participants who did not use illicit drugs (24.4 kg/m2 ± 6.8 vs. 24.3 kg/m2 ± 5.3, P=0.923). Plasma levels of folate were significantly lower among the benzodiazepine users than among the marijuana users (10.0 ng/mL ± 5.2 vs. 14.5 ng/mL ± 5.8, P=0.042) but similar to those of drug non-users (10.0 ng/mL ± 5.2 vs. 10.6 ng/mL ± 9.8, P=0.864). The benzodiazepine users were also less engaged in sports activities than the drug nonusers (67.35% vs. 79.5%, P=0.043). The participants who used non-prescription benzodiazepines did not perceive themselves as drug users.
Table 3 shows longitudinal analyses, using the Mixed Linear Models. Marijuana users had consistently lower BMI over time compared to participants who did not use drugs (β=-0.75, P=0.04), indicating that every unit increase in marijuana use was associated with 0.75 units decrease in BMI. The energy intake of those who used marijuana remained higher over time than that among drug non-users (β=278, P=0.04, not shown), indicating that every unit increase in marijuana use was associated with 278 Kcalorie increase in energy intake. Marijuana users also had higher HIV viral load over time (β=0.29, P=0.013) than drug nonusers, indicating that every unit increase in marijuana use was associated with 0.29 log10 increase in viral load after controlling for micronutrient supplementation, baseline CD4 cell count, and baseline HIV viral load. Marijuana users aged 40 years or older had significantly higher morbidity than participants who did not use any illicit drugs of the same age range (P=0.02). Marijuana users had the same rate of CD4 cell count decline as non-users. After 2 years of follow-up, marijuana users were not significantly different from non-users in adherence to study supplement, but showed a trend towards non-adherence at the end of the study (P=0.075) (Table 4). Comparing adherence rates between men who used marijuana and men who did not use drugs, no significant differences were found between those who used drugs and those who did not use drugs in adherence. These results suggest that the possible lack of adherence among men who are marijuana users appears to be due to gender rather than due to marijuana use.
When we compared women who used benzodiazepine, with women who did not use drugs, those using benzodiazepine were significantly older (36.5 vs. 32.3 years, P=0.008), and the ratio of caloric intake to requirement was higher (0.911 ± 0.503 vs. 0.761 ± 0.459, P=0.053), but did not reach significance. However, the two female groups did not have significantly different BMI (24.3 ± 7.2 vs. 24.8 ± 5.5, P=0.618) or levels of reported physical activity by Chi-Square test (P=0.128).
When we compared men who used marijuana with men who did not use drugs, however, those who used marijuana had significantly lower BMI (21.5 kg/m2 ± 3.8 vs.22.8 kg/m2 ± 3.7, P=0.044) but their age, caloric intake, or the ratio of caloric intake to caloric requirement were not different. We also examined if age was an independent factor from gender and drug use in predicting BMI, and found that both, men and women older than 40 had significantly higher BMI (23.7 kg/m2 ± 4.2 vs. 22.1 kg/m2 ± 3.6, P=0.01 for men, and 26.6 kg/m2 ± 7.0 vs. 24.4 kg/m2 ± 5.3, P<0.002 for women) regardless of drug use. Women more than 40 years of age also had higher plasma folate (14.3 vs. 8.7 ng/mL, P=0.045) than younger women.
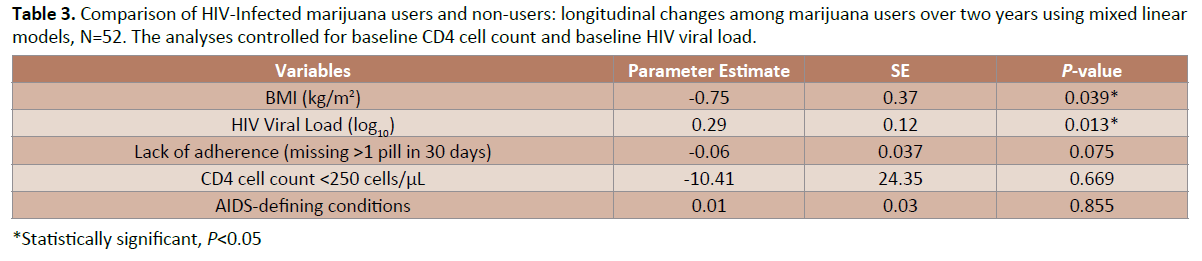
Table 3.Comparison of HIV-Infected marijuana users and non-users: longitudinal changes among marijuana users over two years using mixed linear models, N=52. The analyses controlled for baseline CD4 cell count and baseline HIV viral load.
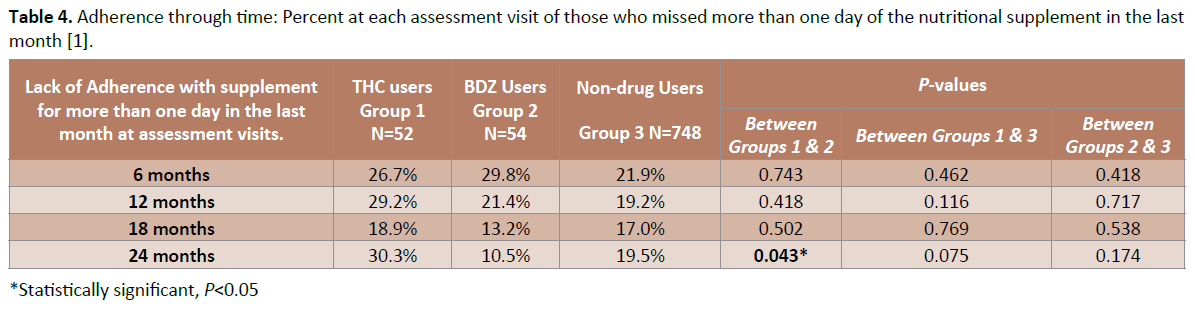
Table 4.Adherence through time: Percent at each assessment visit of those who missed more than one day of the nutritional supplement in the last month [1].
Discussion
Marijuana users in Botswana did not attend the HIV testing clinics, most likely due to stigma and discrimination associated with HIVpositivity and with use of illicit drugs [2]. However, to conquer the HIV epidemic, it is critical to reach all groups who are at high risk for HIV infection, including persons who use illicit drugs who may be at a higher risk for HIV transmission [2,37]. To identify HIV-infected participants who use marijuana and bring them for HIV testing, it was necessary to develop and implement specific targeted outreach strategies, address perceived barriers to testing, establish trust, and conduct network-based recruitment and retention activities. Frequent (monthly) follow-up was critical to ensure a significant retention of this hard-to-reach population in the research study. Although there was no significant difference in adherence to the study supplement between the marijuana users and non-users in this two-year study, adherence decreased among the marijuana users towards the end of the study, and it was necessary to reinforce adherence counselling. This is an important factor to consider when HIV-positive persons who use marijuana are initiated on ART, which requires more than 95% adherence [38]. Comparing adherence rates between men who used marijuana and men who did not use drugs, and between women who used benzodiazepine and women who did not used drugs, no significant differences were found between the stratified gender groups in adherence. This suggests that the differences between the two groups of drug users in adherence are indeed related to gender and not to drug use.
The targeted outreach was successful in identifying HIV-infected participants who used marijuana. Once identified, a large proportion (58%) of the HIV-infected marijuana users was not eligible for the study due to either low CD4 cell count or low BMI at the time of recruitment. The study-eligible participants with CD4 cell count >350 cells/μL at recruitment, had significantly lower BMI despite higher calorie intake throughout the study, and better plasma levels of some micronutrients than drug non-users, most likely due to the higher food intake. Lower BMI in marijuana users is consistent with previous findings [39], and may be related to the consistently higher HIV viral load compared to marijuana non-users. Higher HIV viral load was particularly pronounced in those with overly low levels of plasma zinc and selenium. This is consistent with our previous findings with zinc supplementation preventing immune failure [40], and selenium supplementation reducing HIV viral load in HIV infected drug users [41]. Moreover, an animal study showed that exposure to THC significantly enhanced HIV replication [42], and an epidemiological study indicated that THC may be associated with faster HIV disease progression in men who have sex with men [43]. In contrast, a 21-day placebo-controlled cannabinoid trial in patients on stable ART did not show increase in HIV viral load [44]. In a simian model however, cannabinoids slowed SIV disease progression in males, but not in females [45,46]. Further research is needed to establish whether long-term regular use of marijuana impacts HIV disease progression.
The older marijuana users (age 40 or older) also had significantly more opportunistic diseases than non-users in the same age ranges. There were no differences in CD4 cell count between the drug using and non-using groups. When we compared men who used marijuana with men who did not use drugs, however, those who used marijuana had significantly lower BMI but their age, caloric intake, or the ratio of caloric intake to caloric requirement were not different. However, the lower BMI, higher HIV viral load, more opportunistic diseases among the older marijuana users, and the late presentation into the healthcare system, potentially places them at a higher risk for faster HIV disease progression and for HIV transmission.
In contrast, benzodiazepine users were among the participants recruited from the HIV testing clinics. However, review of their medical charts indicated that benzodiazepines identified in urine were not prescribed by their physicians. Their characteristics were very similar to those of the participants who did not use drugs, and by self-report, did not consider themselves drug users. This perception has been observed previously with benzodiazepine use as anxiolytics both with and without medical prescription [47]. These diverse attitudes between the marijuana and benzodiazepine users may be derived from the fact that marijuana production, trade and possession are criminalized in Botswana, while benzodiazepines may be prescribed by physicians or obtained over the counter in pharmacies [48,49]. Due to lack of self-admission, it was difficult to assess if the number of cases of positive non-prescribed benzodiazepines was due to illegal use of Mandrax, an anxiolytic manufactured in South Africa and widely available in this region that contains both benzodiazepines and methaqualone [50], or to benzodiazepines dispensed in pharmacies without prescription. Marijuana use was an activity usually done by males while the use of benzodiazepines, was mostly found among females. The use of marijuana in the rural areas of Botswana is known, but the use of benzodiazepines was surprising, and the finding of opioid use was also unexpected.
Conclusion
This study demonstrates that a population stigmatized by drug use and HIV-infection can be brought into a clinical and research setting using targeted recruitment strategies in Southern Africa. HIV-infected participants who used marijuana in Botswana were at risk for higher HIV viral load, and very low BMI at diagnosis compared to those who did not use marijuana. HIV-infected marijuana users, despite significantly higher energy intake than non-users over time, had lower BMI and among older users, more opportunistic diseases than HIV-infected marijuana non-users. Adherence to the nutritional supplement was not different between marijuana users and non-users, although a sustained trend towards decreased adherence towards the end of the follow-up was observed, suggesting a need to reinforce adherence at each visit. Benzodiazepine use was detected among 57 participants, mostly females, and they had higher BMI than marijuana users (24.4 kg/m2 ± 6.8 vs. 21.8 ± 3.7 kg/m2, P=0.017). To contain the HIV epidemic, it is critical to develop programs that can outreach to this difficult-to-reach group, and provide medical treatment and nutritional interventions.
Acknowledgment
We thank Jag Khalsa, PhD, Chief, Division of Pharmacotherapies and Medical Consequences of Drug Abuse at the National Institute on Drug Abuse, NIH, for his leadership, advice and support. Dr Khalsa received no compensation for his role in the study. We thank the government of Botswana and the Botswana- Harvard Partnership for the support and cooperation with our study. We thank all of the participants in the study without whom advancement of the management of the HIV disease would not be possible.
This study was funded by the National Institute on Drug Abuse (R01-DA-016551). The sponsor did not participate in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
References
- Piot P, Quinn TC (2013) Response to the AIDS pandemic--a global health model. N Engl J Med 368: 2210-2218.
- Botswana National AIDS Coordinating Agency. Botswana 2012 global AIDS response, Botswana.
- Global report: UNAIDS report on the global AIDS epidemic (2012) Geneva: Joint United Nations Programme on HIV/AIDS (UNAIDS), United Nations.
- Bendavid E, Holmes CB, Bhattacharya J, Miller G (2012) HIV development assistance and adult mortality in Africa. JAMA 307: 2060-2067.
- Hill A, Pozniak A, Raymond A, Heath K, Ford N (2014) Higher antiretroviral treatment coverage is associated with lower HIV infection rates, analysis of 51 low and middle-income countries. Abstract LBPE29. 20th International AIDS Conference, Melbourne, Australia.
- Degenhardt L, Hall W (2012) Extent of illicit drug use and dependence, and their contribution to the global burden of disease. Lancet 379: 55-70.
- Degenhardt L, Ferrari AJ, Calabria B, Hall WD, Norman RE, et al. (2013) The global epidemiology and contribution of cannabis use and dependence to the global burden of disease: results from the GBD 2010 study. PLoS One 8: e76635.
- Kalichman SC, Simbayi LC, Cain D (2010) HIV transmission risk behaviours among HIV seropositive sexually transmitted infection clinic patients in Cape Town, South Africa. Eur J Public Health 20: 202-206.
- Andrade LF, Carroll KM, Petry NM (2013) Marijuana use is associated with risky sexual behaviors in treatment-seeking polysubstance abusers. Am J Drug Alcohol Abuse 39: 266-271.
- Longo LP, Johnson B (2000) Addiction: Part I. Benzodiazepines--side effects, abuse risk and alternatives. AmFam Physician 61: 2121-2128.
- Myers B, Siegfried N, Parry CD (2003) Over-the-counter and prescription medicine misuse in Cape Town--findings from specialist treatment centres. S Afr Med J 93: 367-370.
- Pétursson H (1994) The benzodiazepine withdrawal syndrome. Addiction 89: 1455-1459.
- AIDS 2014 Programme (2014) 20th International AIDS Conference, Melbourne, Australia.
- Murray CJ, Ortblad KF, Guinovart C, Lim SS, Wolock TM, et al. (2014) Global, regional, and national incidence and mortality for HIV, tuberculosis, and malaria during 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 384: 1005-1070.
- Stoneburner R, Korenromp E, Lazenby M, Tassie JM, Letebele J, et al. (2014) Using health surveillance systems data to assess the impact of AIDS and antiretroviral treatment on adult morbidity and mortality in Botswana. PLoS One 9: e100431.
- Sunday Standard (2012) Has Botswana lost the battle against drugs and alcohol abuse? Online Edition.
- Botswana Alcohol AIDS Project (2004) Substance Abuse in Botswana. Tripod, Botswana.
- Kip E, Ehlers VJ, van der Wal DM (2009) Patients' adherence to anti-retroviral therapy in Botswana. J NursScholarsh 41: 149-157.
- Botswana Student Network (2013) Abuse of alcohol and drugs in schools worrisome. Workshop organized by the Mochudi Police. Mochudi, Botswana.
- Dos Santos MM, Kruger P, Mellors SE, Wolvaardt G, van der Ryst E (2014) An exploratory survey measuring stigma and discrimination experienced by people living with HIV/AIDS in South Africa: the People Living with HIV Stigma Index. BMC Public Health 14: 80.
- Marsicano E, Dray-Spira R, Lert F, Aubrière C, Spire B, et al. (2014) Multiple discriminations experienced by people living with HIV in France: results from the ANRS-Vespa2 study. AIDS Care 26 Suppl 1: S97-97S106.
- UNAIDS (2013) AIDS by the numbers.
- Cabral GA, Jamerson M (2014) Marijuana use and brain immune mechanisms. Int Rev Neurobiol 118: 199-230.
- Qian HZ, Mitchell VJ, Bebawy S, Cassell H, Perez G, et al. (2014) Current drug use and lack of HIV virologic suppression: point-of-care urine drug screen versus self-report. BMC Infect Dis 14: 508.
- Molina PE, Amedee A, LeCapitaine NJ, Zabaleta J, Mohan M, et al. (2011) Cannabinoid neuroimmune modulation of SIV disease. J NeuroimmunePharmacol 6: 516-527.
- Page JB, Singer M (2010) Comprehending Drug Use: Ethnographic Research at the Social Margins. New Brunswick, NJ: Rutgers University Press, USA.
- Baum MK, Campa A, Lai S, Sales Martinez S, Tsalaile L, et al. (2013) Effect of micronutrient supplementation on disease progression in asymptomatic, antiretroviral-naive, HIV-infected adults in Botswana: a randomized clinical trial. JAMA 310: 2154-2163.
- Bordi R, Zeidan J, Fonseca S, Stafova P, Filali A, et al. (2012) Impact of Cocaine Use on the Immune System in HIV Positive Adults on Stable Antiretroviral Therapy (ART): A Systems Biology Approach. XXI International HIV/ AIDS Conference abstract, Washington D.C.
- Baum MK, Rafie C, Lai S, Sales S, Page B, et al. (2009) Crack-cocaine use accelerates HIV disease progression in a cohort of HIV-positive drug users. J Acquir Immune DeficSyndr 50: 93-99.
- Grande F, Keys A (1980) Body weight, body composition, and calorie status. In R. S. Goodhart, M. E. Shils, 6theds, Modern nutrition in health and disease, Lea &Febiger, Philadelphia.
- BMI Calculator. Harris-Benedict Equation.
- Schofield WN (1985) Predicting basal metabolic rate, new standards and review of previous work. Hum NutrClinNutr39: 5–41.
- Milne DB, Ralston NV, Wallwork JC (1985) Zinc content of cellular components of blood: methods for cell separation and analysis evaluated. ClinChem 31: 65-69.
- Olson OE, Palmer IS, Whitehead EI (1973) Determination of selenium in biological materials. Methods Biochem Anal 21: 39-78.
- Bieri JG, Tolliver TJ, Catignani GL (1979) Simultaneous determination of alpha-tocopherol and retinol in plasma or red cells by high pressure liquid chromatography. Am J ClinNutr 32: 2143-2149.
- Scott JM, Ghanta V, Herbert V (1974) Trouble-free microbiologic serum and red cell folate assays. Am J Med Technol 40: 125-134.
- Browne FA, Wechsberg WM (2010) The intersecting risks of substance use and HIV risk among substance-using South African men and women. CurrOpin Psychiatry 23: 205-209.
- Kabore L, Muntner P, Chamot E, Zinski A, Burkholder G, et al. (2015) Self-Report Measures in the Assessment of Antiretroviral Medication Adherence: Comparison with Medication Possession Ratio and HIV Viral Load. J IntAssocProvid AIDS Care.
- Ostadhadi S, Rahmatollahi M, Dehpour AR, Rahimian R (2015) Therapeutic potential of cannabinoids in counteracting chemotherapy-induced adverse effects: an exploratory review. Phytother Res 29: 332-338.
- Baum MK, Lai S, Sales S, Page JB, Campa A (2010) Randomized, controlled clinical trial of zinc supplementation to prevent immunological failure in HIV-infected adults. Clin Infect Dis 50: 1653-1660.
- Hurwitz BE, Klaus JR, Llabre MM, Gonzalez A, Lawrence PJ, et al. (2007) Selenium Supplementation Suppresses HIV Viral Load Over 9 Months: A Randomized, Double-Blind, Placebo Controlled Trial. Arch of Intern Med 167:148-154.
- Roth MD, Tashkin DP, Whittaker KM, Choi R, Baldwin GC (2005) Tetrahydrocannabinol suppresses immune function and enhances HIV replication in the huPBL-SCID mouse. Life Sci 77: 1711-1722.
- Tindall B, Cooper DA, Donovan B, Barnes T, Philpot CR, et al. (1988) The Sydney AIDS Project: development of acquired immunodeficiency syndrome in a group of HIV seropositive homosexual men. Aust N Z J Med 18: 8-15.
- Abrams DI, Hilton JF, Leiser RJ, Shade SB, Elbeik TA, et al. (2003) Short-term effects of cannabinoids in patients with HIV-1 infection: a randomized, placebo-controlled clinical trial. Ann Intern Med 139: 258-266.
- Amedee AM, Nichols WA, LeCapitaine NJ, Stouwe CV, Birke LL, et al. (2014)Chronic ??-tetrahydrocannabinol administration may not attenuate simian immunodeficiency virus disease progression in female rhesus macaques. AIDS Res Hum Retroviruses 30:1216-1225.
- Chandra LC, Kumar V, Torben W, VandeStouwe C, Winsauer P, et al. (2015)Chronic administration of Δ9-tetrahydrocannabinol induces intestinal anti-inflammatory microRNA expression during acute simian immunodeficiency virus infection of rhesus macaques. J Virol 89:1168-1681.
- McCabe SE, West BT (2014) Medical and nonmedical use of prescription benzodiazepine anxiolytics among U.S. high school seniors. Addict Behav 39: 959-964.
- Drugs and related substances act no. 18 of 1992. Government of Botswana.
- Jackson Rautenbach (2012) Is Dagga the healing of a nation?
- Living with mental health illness

