N Hanna1*, T Smaira2, A Fenianos1, O Safi1 and Z Saliba1
Pediatric Cardiology unit, Department of pediatrics, Hotel Dieu de France Hospital, Beirut, Lebanon
Radiology Department, Hotel Dieu de France Hospital, Beirut, Lebanon
*Corresponding Author:
N Hanna
Pediatric cardiology unit
Department of pediatrics
Hotel Dieu de France Hospital
Beirut, Lebanon
E-mail: najibhanna@gmail.com
Received date: December 07, 2015; Accepted date: December 17, 2015; Published date: December 24, 2015
Citation: Hanna N, Smaria T, Fenianos A, et al. Recanalisation of Totally Occluded Modified Blalock Taussig Shunt by Balloon Angioplasty 48 Hours after its Construction. j intensive & Crit Care 2015, 2:1.
Keywords
Fallot; Catheter canalisation; Blalock–taussig shunt; Shunt occlusion; Respiratory syncytial virus
Abbreviations
TOF: Tetralogy of Fallot; BTS: Blalock Taussig Shunt; RSV: Respiratory Syncytial Virus; LAD: Left Anterior Descending Coronary; VSD: Ventricular Septal Defect; WBC: White Blood Cell; CRP: C Reactive Protein; ACT: Activated Clotting Time
Case Report
An 18 months old boy with TOF and deep cyanosis was admitted for a palliative surgery. The cardiac catheterization had shown a hypoplastic pulmonary tree and an abnormal LAD crossing the infundibulum. He was well vaccinated but no Palivizumab injection was performed.
The laboratory tests showed minor thalassemia and iron deficiency. No hemostasis disorder was documented. A 4 mm Gore-Tex tube was inserted between the arterial brachiocephalic trunk (ABCT) and the proximal right pulmonary artery. Immediate heparin therapy (500 UI/Kg/day) was initiated as well as oral Aspirin (5 mg/Kg/day). An Adequate ACT level (64 seconds) was rapidly achieved and the shunt patency was documented by echocardiography and color Doppler 24 hours later. At 36 hours after surgery, the SpO2 suddenly dropped from 83 to 60%. Continuous flow profile of the shunt could not be identified by Doppler echocardiography. At catheterization, a 5F femoral arterial short introducer was inserted. A selective angiogram in the ABCT, using a 5F mammary catheter (Cordis), confirmed complete shunt occlusion at 5mm of the aortic connection (Figure 1). Using a 0.014” “Cross It” guide wire (Abott), the shunt was crossed to place the wire (Figure 1-3) distally in the right pulmonary branch. A 4F Right Judkins cathter (Cordis special) was used to cross the shunt over the 0.014” wire and then, a 0.035” exchange wire was used to introduce a multipurpose 5F guiding catheter in the right pulmonary artery. After that, the 0.014” was replaced in the guiding catheter and using a 4 mm × 20 mm coronary TREK balloon (Abott) multiple hand inflations in the shunt were repeated to reestablish the shunt patency (Figure 2). At the final angiogram, aortic and pulmonary shunt’s ends were free of narrowing or kinking (Figure 3). The SpO2 increased to 85% and heparin therapy with oral Aspirin was continued and oral Clopidogrel (1 mg/Kg/d) was added. He was extubated the next day and fed normally. Repeated Doppler echocardiography showed the patency of the shunt. Three days later, high grade fever and cough appeared. The nasopharyngeal secretions tests showed the presence of RSV. The Chest X-ray showed bilateral infiltrates (Figure 4) and WBC count was 3500 (N36%; L69%), CRP 26 mg/dL. The dyspnea exacerbated and tracheal bleeding followed by anuria occurred. Although no bacterial super infection was documented, a large spectrum anti-biotherapy was started. High frequency ventilation was used but despite all therapeutic measures the hypoxia and hypercapnia worsened and the child died on the 8th day after the surgery. Cardiac ultrasound performed 2 hours before death showed the patency of the shunt (Figure 4).
Discussion
Surgery is the only curative treatment for TOF and should be electively performed in infancy. However, in some instances, e.g. low weight, severe pulmonary branches hypoplasia, abnormal coronary arteries and multiple VSD, a palliative surgery should be undertaken.
The classic BTS, first performed in 1944 [1] is nowadays replaced by a gore-tex tube between the aorta and the pulmonary branch. Despite early anticoagulation and anti-aggregant therapy, the early or late shunt occlusion rate is still high [2]. The usual cause of shunt obstruction is a thrombus formation closing the narrow lumen of the graft, which in a majority of cases is additionally narrowed by coexisting distal stenosis present at the junction of the BT graft and the narrow pulmonary artery branch. Total occlusion in the early postoperative period is not a contraindication to catheter treatment. The freshly constituted thrombus can be crossed using some special wires and maneuvers. The mammary catheter is adapted to the right angled aorto-shunt connection. After that, the “off label” use of a 0.014” wire, conceived for coronary occlusions, permits a shunt recanalisation. Then, progressive or one step ballooning, depending on balloon tractability, may restore the shunt patency. Additionally, some advocate the use of local or systematic thrombolytic therapy combined with a successful balloon angioplasty procedure [3-7]. Stenting may be needed particularly in distant from surgery interventions and residual narrowing.
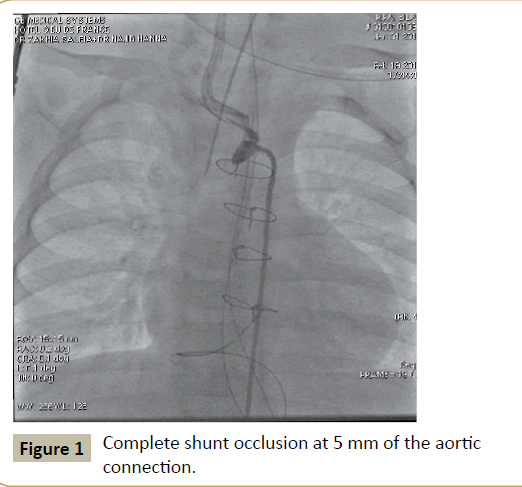
Figure 1: Complete shunt occlusion at 5 mm of the aortic connection.
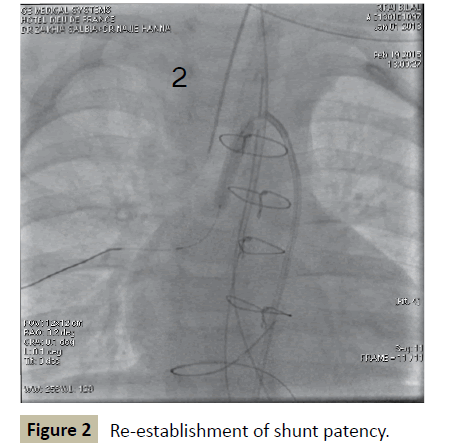
Figure 2: Re-establishment of shunt patency.
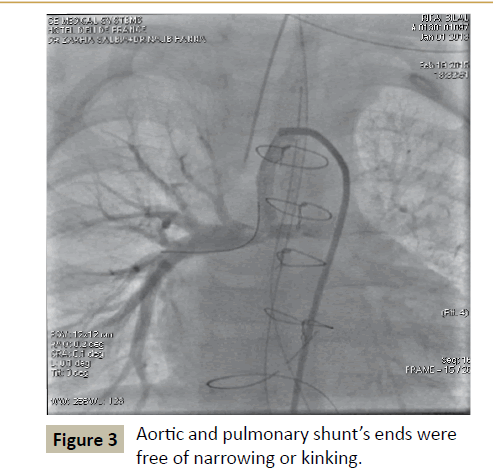
Figure 3: Aortic and pulmonary shunt’s ends were free of narrowing or kinking.
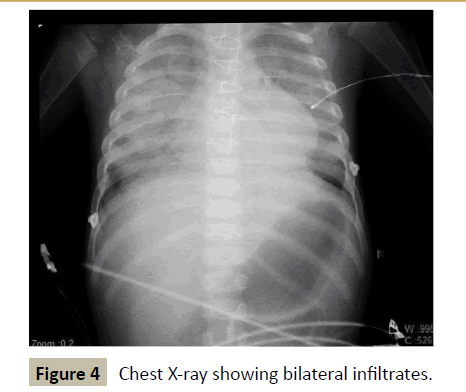
Figure 4: Chest X-ray showing bilateral infiltrates.
Transcatheter balloon dilatation of stenosed shunts has been proposed as an alternative to surgical revision. Most have been performed for stenosed classical BTS, where direct end-to-side anastomosis of the subclavian artery to the pulmonary artery has been performed [2].
In our case, we performed only a balloon angioplasty with total recanalisation of the modified shunt, without thrombolytic therapy.
Even with the success of the procedure, the child died most likely of his RSV pneumopathy. Palivizumab has reduced the incidence of respiratory syncytial virus hospitalization in infants and children with congenital heart disease by 45%. Although the mortality rate of children with congenital heart disease hospitalized with respiratory syncytial virus infection has declined from 37% to approximately 3% over the past 3 decades and there are recommendations for providing palivizumab up to age 24 months in children with congenital heart disease [8]. Ribavirin therapy, not available in our country, would have been an indication in this case.
Conclusion
Percutaneous emergency recanalisation of occluded BTS is a safe and effective method and can avoid redo risky surgery.
Palivizumab prophylaxis may help preventing severe pneumopathy in these patients and thus improving the outcome.
References
- Blalock, Taussig H (1945)The surgical treatments of malformations of the heart. Journal of the American medical association 128: 189-202.
- Moszura T, Zubrzycka M, Michalak KW, Rewers B, Dryzek P, et al. Acute and late obstruction of a modified Blalock–Taussig shunt: a two-center experience in different catheter-based methods of treatment. Interactive CardioVascular and Thoracic Surgery 10: 727-731.
- Mathilde Bonnet, Jérôme Petit, Virginie Lambert, Philippe Brenot,Jean-Yves Riou, et al. (2015)Catheter-Based Interventions for Modified Blalock–Taussig Shunt Obstruction: A 20-Year Experience.Pediatr Cardiol 36: 835-841.
- Narayanswami Sreeram, Kevin Walsh, Ian Peart (1993)Recanalisation of an occluded modified Blalock-Taussig shunt by balloon dilatation. Br Heart J 70:474-475.
- Gillespie MJ, Rome JJ (2008) Transcatheter treatment for systemic-to-pulmonary artery shunt obstruction in infants and children. Catheter Cardiovasc Interv 71:928-935.
- Rao PS, Levy JM, Chopra PS. Balloon angioplasty of stenosed Blalock–Taussig anastomosis: role of balloon-on-a-wire in dilating occluded shunts. Am Heart J 120:1173-1178.
- Wang JK, Wu MH, Chang CI, Chiu IS, Lue HC (2001) Balloon angioplasty for obstructed modified systemic-pulmonary artery shunts and pulmonary artery stenoses. J Am Coll Cardiol 37:940-947.
- Geskey JM, Thomas NJ, Brummel GL (2007)Palivizumab in congenital heart disease: should international guidelines be revised? Expert Opin Biol Ther7: 1615-1620.

