Keywords
Cholesterol; Triglyceride; Sepsis; Non-septic patient
Introduction
Sepsis is the most common cause of admission to the Intensive Care Unit (ICU) [1]. The incidence of sepsis is increasing in spite of the advanced efforts for management of sepsis [2]. Sepsis is associated with severe metabolic alterations, including insulin resistance and increased levels of Triglycerides (TGs) and lower level of both high and Low-density Lipoproteins (LDL) [3].
Several mechanisms could explain hypocholesterolemia in critical illness and sepsis as the disturbance between synthesis and utilization of plasma lipids, usage of lipids to restore damaged cell membranes, and the interaction of bacterial toxins with lipids [1]. The levels of High-density Lipoproteins (HDLs) are reduced in sepsis/septic shock, and the magnitude of this reduction is positively correlated with the severity of the illness [4]. Lipopolysaccharide (LPS) is the major component of the outer membrane of Gram-negative bacteria has a crucial role in the initiation of sepsis [5,6]. It was suggested that serum cholesterol might be a useful prognostic marker of sepsis [7]. The prognostic value of changes in lipoprotein profile is still not confirmed [8]. The inclusion of lipid values in clinical risk assessment scores of critically ill patients has been advocated [9]. There are controversies related to the concentration of lipids because most of these studies were conducted in Western populations [5,10,11].
An early prognostic indicator to identify patients at highest risk for mortality in the ICU was recommended [12] also there are controversies between the results of previous studies in critically ill patients about the value of changes in cholesterol levels, and HDL as predictors of severity of illness by some investigators [10,13,14,] while other studies could not confirm this association [6,15].
The aim of the study
This observational study was designed to evaluate the difference between the level of serum cholesterol and triglyceride in septic and non-septic patients in the surgical ICU and to find correlation between the level of serum cholesterol and triglyceride and both Acute Physiology And Chronic Health Evaluation Score (APACHE) II and quick Sequential Organ Failure Assessment (qSOFA) score and their relation to mortality in Egyptian population.
Materials and Methods
Study design
This study was conducted in the surgical intensive care unit (SICU) of Beni-Suef University hospital between January 2018 and December 2018 after approval of the local ethics and research committee (The FM-BSU REC) and obtaining consents from the patients or their guardians. This study was registered at ClinicalTrials.gov, ClinicalTrials.gov Identifier: NCT03359369.
Eligibility criteria
The study population included the patients (age range between 20 and 70 years) of both sexes (septic and non-septic patients, e.g., trauma patients, post-surgical patients).
Exclusion criteria
1. Pregnancy
2. ICU readmission
3. Dyslipidemia
4. Patients with liver disease
5. Concomitant use of immunosuppressive therapy
6. Using statin or steroid (≥ 15 mg/day) within the previous seven days
7. Patients who had been treated with corticosteroid therapy for septic shock before admission to ICU
8. Patients sedated by propofol
Management of the patients in the SICU, starting from the day of admission
Patients admitted to SICU either postsurgical patients or trauma patient received from the emergency department. Some patients were already intubated and ventilated, and on arrival to SICU, they were connected to the mechanical ventilator. Other patients initially did not need intubation or ventilation, and during the course of the patient stay in the SICU some of these patients deteriorated and needed intubation and mechanical ventilation or administration of vasoactive drugs. For all patients monitors were connected including (Noninvasive Blood Pressure (NIBP), Electrocardiogram (ECG), pulse Oximetry, temperature monitoring) and baseline readings were recorded. Central venous line and arterial line were inserted under complete aseptic technique also urinary catheter was inserted for urine output monitoring.
Inotropes and vasopressors as dopamine, epinephrine and norepinephrine were used if needed and the rate of infusion was adjusted according to the blood pressure. Full investigations were done including (Complete Blood Count (CBC), coagulation profile, serum electrolytes, liver function tests, kidney function tests, Arterial-Blood Gas (ABG), urine analysis). Radiological examination as chest X-ray was done and pelvic-abdominal u/s was done if needed. For the patient with sepsis, cultures were done (urine, sputum, blood culture) and also cultures were done from the suspected source of infection (e.g., from the surgical drain in case of alleged abdominal or pelvic as the source of infection following surgery), and initially empirical antibiotics were started.The patients were randomly assigned into two groups, septic patients (group S, n=50) according to established consensus definitions [16] or non-septic patients (NS, n=45) as post-surgical and trauma patients.
The following data were recorded by senior SICU resident who was unaware of the study protocol
Age, sex, the cause of SICU admission, administration of vasoactive drugs, length of SICU stay, 28-day mortality, days on mechanical ventilation, Acute Physiology, and Chronic Health Evaluation II (APACHE II) scores [17], Quick Sequential Organ Failure Assessment (qSOFA) scores. The score ranges from 0 to 3 points. The presence of 2 or more qSOFA points near the onset of infection is associated with a higher risk of death or prolonged intensive care unit stay [18]. Serum cholesterol and triglyceride on days 0 (ICU admission), 1st, 3rd, 7th, 10th and 14th day.
Statistical methods
Sample size: After a pilot study with five patients in each group, the detectable difference in cholesterol level on the third day between the two groups was 46 mg/dL, and the difference in the standard deviation was 55. Accordingly, the calculated minimum sample size was 39 patients in each group with 95% power and α level was 0.05 using a t-test, Biostatistics, version 3.01 was used to calculate the sample size. The number was increased to 50 patients in each group in case of the drop in any case.
Data analysis: Data were statistically described in terms of mean ± standard deviation (± SD), median and range, or frequencies (number of cases) and percentages when appropriate. Comparison of numerical variables between the study groups was done using Student-t-test for independent samples. For comparing categorical data, Chi-square (χ2) test was performed. The exact test was used instead when the expected frequency is less than 5. Correlation between various variables was done using Pearson moment correlation equation for linear relation of normally distributed variables and Spearman rank correlation equation for non-normal variables/non-linear monotonic relation p values less than 0.05 was considered statistically significant. The correlation was done between APACHE II score and 28 days mortality and cholesterol and triglyceride level in day 0 and also correlation was done between qSOFA score and 28 days mortality and cholesterol and triglyceride level in day 0 for both septic and non-septic group. All statistical calculations were done using computer program IBM SPSS (Statistical Package for the Social Science; IBM Corp, Armonk, NY, USA) release 22 for Microsoft Windows.
Results
In this study, 100 patients were assessed for eligibility, allocated into 2 groups, septic group, and non-septic group, 5 patients were excluded from the non-septic group as they died before the third day of the SICU stay.
Demographic data
There was no statistically significant difference regarding the age and sex of the patients between the septic and non-septic groups (Table 1).
| Variable |
Group S (n=50) |
Group NS (n=45) |
p value |
| Sex (M/F) |
30/20 (60%/40%) |
31/14 (69%/31%) |
0.838 |
| Age (Years) |
48.96 ± 5.48 |
49. 6 ± 7.34 |
0.728 |
Group S = Septic Group; Group NS = Non Septic Group
p values ≤ 0.05 are considered statistically significant
Table 1 Demographic Data; Data are presented as mean ± SD, numbers (%).
The source of sepsis in the patient of the septic group is presented in Table 2.
| Source of sepsis |
Number of patients |
| Respiratory tract |
20 (40%) |
| Urinary tract |
13 (26%) |
| Gastroenterological |
7 (14%) |
| Wound infection |
5 (10%) |
| Soft tissue infection |
2 (4%) |
| Unknown |
3 (6%) |
| Total |
50 |
Table 2. Source of sepsis in the patients of the septic group; Data are presented as number (%).
The diagnosis of the patients is presented in Table 3.
| Diagnosis of patient |
Number of patients in the Septic group (S) |
Number of the patient in the Non-septic group (NS) |
| Postoperative |
38 (76%) |
37 (82.2%) |
| CNS surgery |
11 (22%) |
4 (9%) |
| Abdominal surgery |
7 (14%) |
3 (6.7%) |
| Uro-surgery |
4 (8%) |
6 (13.3%) |
| Vascular surgery |
4 (8%) |
3 (6.7%) |
| Malignancy surgery |
7 (14%) |
5 (11%) |
| Orthopedic surgery |
1 (2%) |
8 (17.8%) |
| Gynecological surgery |
1 (2%) |
3 (6.7%) |
| ENT surgery |
2 (4%) |
1 (2%) |
| Plastic surgery |
1 (2%) |
4 (9%) |
| Trauma |
12 (24%) |
8 (17.8%) |
| Total |
50 |
45 |
Table 3: The diagnosis of the patients; Data are presented as number (%).
APACHE II score was statistically significantly higher in the septic group (S): [32(24-48)] than the non-septic group (NS) [8.5(2-35)], (p value <0.001).
qSOFA score was statistically significantly higher in septic group (S) [2(2-3)] than the non-septic group (NS) [1(0-3)],(p value < 0.001) (Table 4).
| Variable |
Group S (n=50) |
Group NS (n=45) |
p value |
| APACHE II |
32 (24-48)* |
8.5 (2-35) |
<0.001 |
| qSOFA |
2 (2-3)* |
1 (0-3) |
<0.001 |
Group S = Septic Group; Group NS = Non Septic Group
*p values <0.05 are considered statistically significant
Table 4: Acute physiology and chronic health evaluation II (APACHE II) score and quick sequential organ failure assessment (qSOFA) score: Data are presented as median (range).
The number of patients needed vasoactive drugs was statistically significantly higher in the septic group (S) 33 patients (66%) than the non-septic group (NS) 4 patients (8.8%), (p value <0.001) (Table 5).
| Variable |
Group S (n=50) |
Group NS (n=45) |
p value |
| Administration of vasoactive drugs |
33 (66%)* |
4 (8.8%) |
<0.001 |
| 28 day Mortality |
44 (88%)* |
8 (17.7%) |
<0.001 |
| Length of Surgical Intensive Care Unit (SICU) stay |
13.9 ± 9.0 * |
4.4 ± 1.9 |
<0.001 |
| Days on Mechanical ventilation (MV) |
13.9 ± 9.0 * |
0.76 ± 1.8 |
<0.001 |
Group S = Septic Group
Group NS = Non-Septic Group
*p values≤0.05 are considered statistically significant
Table 5: Administration of vasoactive drugs, 28-days Mortality, length of Surgical Intensive Care Unit (SICU) stay, and days on Mechanical Ventilation, Data are presented as mean ± SD, numbers (%).
28 Days mortality was statistically significantly higher in the septic group (S) 88% (44 patients) than the non-septic group (NS) 17.77% (8 patients); (p-value <0.001); (Table 5).
The length of SICU stay was statistically significantly longer in the septic group (S) 13.9 ± 9.3 than the non-septic group (NS) 4.4 ± 1.9, (p value <0.001); (Table 5).
Days on mechanical ventilation were statistically significantly longer in the septic group (S) 13.9 ± 9.3 than the non-septic group (NS); 0.76 ± 1.8, (p value <0.001); (Table 5).
Cholesterol level (mg/dL): Day 0: It was 119.4 ± 29.33 in the septic group (S) versus 131.2 ± 35.37 in the non-septic group (NS and it was statistically significantly lowering the septic group versus the non-septic group (p-value=0.037).
Day 1: Cholesterol level in day 1 was statistically significantly lower in the septic group (S) 103.6 ± 29.19 versus the non-septic group (NS) 123.56 ± 36.5 (p-value <0.001).
Day 3: Cholesterol level in day 3 was statistically significantly lower in the septic group(S) 80.7 ± 26.87 than in the non-septic group (NS) 124.84 ± 32.4 (p-value <0.001) (Table 6).
| Cholesterol level (mg/dL) |
Group S (n=50) |
Group NS (n=45) |
p value |
| Day 0 |
119.4 ± 29.33 |
131.2 ± 35.37 |
0.076 |
| Day 1 |
103.6 ± 29.19 |
123.56 ± 36.5 |
0.001 |
| Day 3 |
80.7 ± 26.87* |
124.84 ± 32.4 |
<0.001 |
Group S= Septic Group; Group NS = Non Septic Group
*p values<0.05 are considered statistically significant
Table 6: Cholesterol level (mg/dL): Data are presented as mean ± SD
Triglyceride level (mg/dL): Day 0: Triglyceride level in day 0 showed no statistically significant difference between the two groups (p value=0.08) it was 134.94 ± 73. 06 in the septic group (S) and it was 116.8 ± 52.05 in the non-septic group (NS).
Day 1: Triglyceride level in day 1 was statistically significantly higher in the septic group (S) 151.5 ± 54.8 than the non-septic group (NS) 112.14 ± 33.02 (p value<0.001).
Day 3: Triglyceride level in day 3 was statistically significant higher in the septic group (S) 185.1 ± 43.2 than the non-septic group (NS) 113.5± 39.56 (p value <0.001) (Table 7).
| Triglyceride level (mg/dL) |
Group S (n=50) |
Group NS (n=45) |
p value |
| Day 0 |
134.94 ± 73.06 |
116.8 ± 52.05 |
0.163 |
| Day 1 |
151.5 ± 54.79* |
112.14 ± 33.02 |
<0.001 |
| Day 3 |
185.1 ± 43.2* |
113.5 ± 39.56 |
<0.001 |
Group S= Septic Group; Group NS = Non Septic Group
*p values<0.05 are considered statistically significant
Table 7: Triglyceride level (mg/dL): Data are presented as mean ± SD.
For the non-septic group the length of Surgical Intensive Care Unit (SICU) stay was 4.4 ± 1.9 days and the patients were discharged to the word, so we continue following up the cholesterol and triglyceride levels; cholesterol level (mg/dL) was increasing it was 125.28 ± 34.05, 127.71 ± 26.65 and 129.77 ± 24.45 on day 7,10 and 14 respectively.
Triglyceride level (mg/dL) was 115.04 ± 42.35, 114.47 ± 43.00 and 114.27 ± 43.4 on days 7, 10 and 14 respectively, (Figure 2).
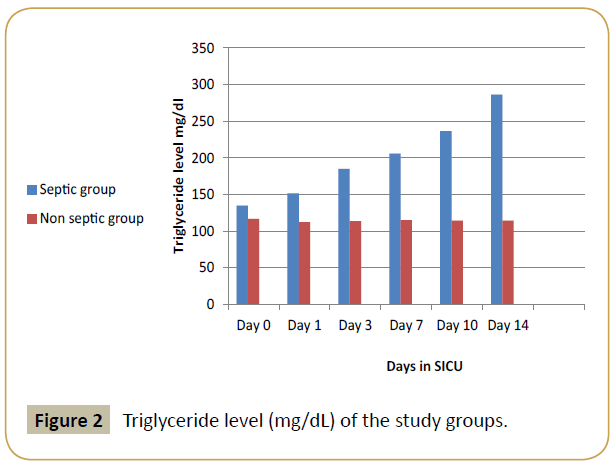
Figure 2: Triglyceride level (mg/dL) of the study groups
For the septic group 11 patients died before the tenth day, so cholesterol and triglyceride levels were measured for the remaining 39 patients; cholesterol level (mg/dL) was markedly reduced it was 62.07 ± 16.10, 59.97 ± 16.24 and 56.33 ± 14.4 on day 7, 10 and 14 respectively, The triglyceride level was increasing it was 205.97 ± 30.25, 236.52 ± 32.48 and 286.64 ± 30.46 on days 7,10 and 14 respectively (Figure 1).
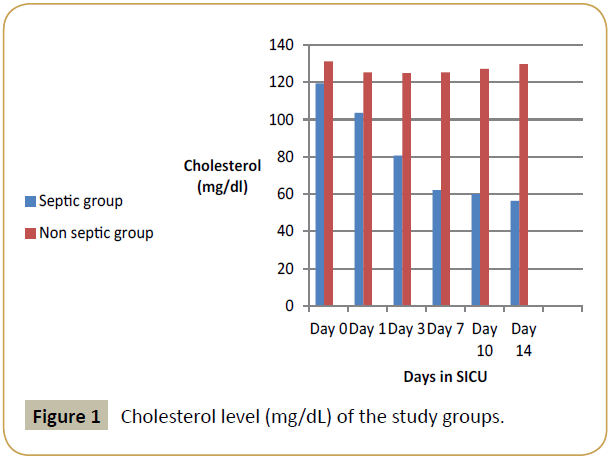
Figure 1: Cholesterol level (mg/dL) of the study groups.
Regarding the correlation in the septic (S) and non-septic group (NS)
For the septic group (S): There was no significant correlation between APACHE II score and 28 days mortality (p-value=0.933, correlation coefficient=-0.012).
There was a weak negative correlation between APACHE II score and cholesterol level on the day 0 of admission (p-value=0.030, correlation coefficient=-0.308) (Figure 3).
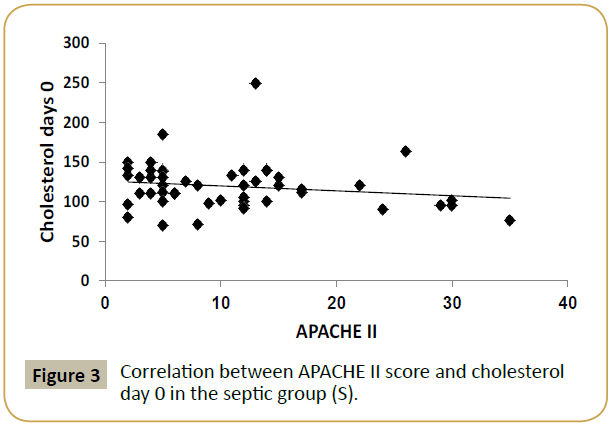
Figure 3: Correlation between APACHE II score and cholesterol day 0 in the septic group (S).
There was no significant correlation between APACHE II score and triglyceride level on the day 0 of admission (p-value=0.0541, correlation coefficient=-0. 089), (Table 8).
| |
Group S (n=50) |
Group NS (n=45) |
| APACHE II |
qSOFA |
APACHE II |
qSOFA |
| 28 days Mortality |
-0.012 |
0.094 |
0.813 |
0.804 |
| -0.933 |
-0.517 |
(< 0.001) |
(< 0.001) |
| Cholesterol 0 |
-0.308 |
-0.107 |
0.085 |
0.034 |
| -0.03 |
-0.458 |
-0.558 |
-0.815 |
| TGs 0 |
-0.089 |
0.096 |
-0.039 |
-0.056 |
| -0.541 |
-0.508 |
-0.786 |
-0.699 |
Table 8: Correlations in the septic (S) and non-septic groups (NS); Values represent the correlation coefficient (p value).
There was no significant correlation between qSOFA score and 28 days mortality (p-value=0.517, correlation coefficient=-0.094), (Table 8).
There was no significant correlation between qSOFA score and cholesterol level on the day 0 of admission (p-value=0.458, correlation coefficient=-0.107), (Table 8).
There was no significant correlation between qSOFA score and triglyceride level on the day 0 of admission (p-value=0. 508, correlation coefficient=-0.096), (Table 8).
For the non-septic group (NS): There was a strong positive correlation between APACHE II score and 28 days mortality (p value <0.001, correlation coefficient=0.813) (Figure 4).
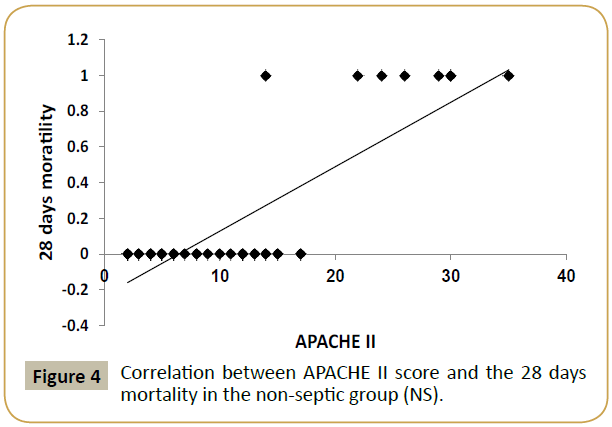
Figure 4: Correlation between APACHE II score and the 28 days mortality in the non-septic group (NS).
There was no significant correlation between APACHE II score and cholesterol level on the day 0 of admission (p-value=0.558, correlation coefficient=0.085), (Table 8).
There was no significant correlation between APACHE II score and triglyceride level on the day 0 of admission (p-value=0.786, correlation coefficient=-0.039), (Table 8).
There was a strong positive correlation between qSOFA score and 28 days mortality (p value <0.001, correlation coefficient=0.804) (Figure 5).
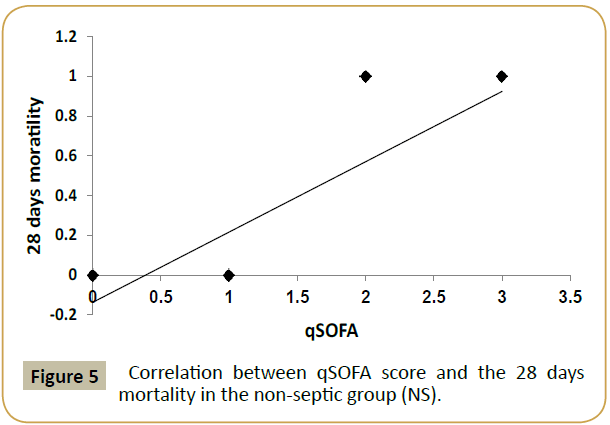
Figure 5: Correlation between qSOFA score and the 28 days mortality in the non-septic group (NS).
There was no significant correlation between qSOFA score and cholesterol level on the day 0 of admission (p-value=0.815, correlation coefficient=0.034).
There was no significant correlation between qSOFA score and triglyceride level on the day 0 of admission (p-value=0.699, correlation coefficient=-0.056); (Table 8).
Discussion
The results of the present study showed that serum cholesterol levels decreased markedly, and triglyceride levels increased in patients with sepsis compared to non-septic patients, and there was a significant difference between septic and non-septic patients. The septic patients had a higher rate of mortality than the non-septic patients, in septic patients there was increasing in length of SICU stay, administration of vasoactive drugs, days on mechanical ventilation, higher qSOFA, and APACHE II scores compared to non-septic patients. Patients with severe sepsis have low levels of cholesterol and high levels of triglycerides [3]. Hypertriglyceridemia is due to reduced plasma Triglyceride (TG) clearance rate [16]. An increase in triglyceride levels during sepsis might have beneficial effects on the host because triglyceriderich lipoproteins bind and neutralize the effects of endotoxin [19]. The hypocholesterolemia of acute illness is associated with a moderate increase in triacylglyceride levels [20]. Mechanisms are an imbalance between synthesis and utilization of plasma lipids, usage of lipids to restore damaged cell membranes [21].
Cetinkaya et al. [5], observed that patients with sepsis had high TG levels and that the TG level 150 mg/dL at 0 hours (onset of sepsis) were a significant predictive marker of sepsis mortality rate. Barati et al. [9] investigated changes in plasma lipid levels in patients with sepsis found markedly lower levels of cholesterol, LDL, and HDL on admission and ten days later, which was online with the presented study but no difference could be found in triglyceride level which also went in line with the results of the given research, in their study on non- septic patients, total cholesterol level increased on 10 days than the day of admission, triglyceride level showed no significant change it was 182.8 ± 45.9 mg/dL and after 10 days it was 181.4 ± 40 mg/dL, in the presented study triglyceride level was 116.8 ± 52.6 mg/dL on day 0, 115.04 ± 42.35, 114.47 ± 43.00 and 114.27 ± 43.40 on day 7, 10 and 14 respectively. A study by Lekkou et al. [22] included 50 patients with severe sepsis. Sepsis survivors had significantly higher HDL-C concentrations than non survivors. They concluded that low cholesterol and lipoprotein concentrations are detected in septic patients especially in individuals with poor prognosis, which went in line with the results of the presented study. Jeyasuriya et al. [23] concluded that ICU patients showed an increasing trend of total cholesterol levels had a higher rate of survival. Lee et al. [24] concluded that persistent hypocholesterolemia (<61 mg/dL) independently predicted in-hospital mortality, after emergency GI surgery in patients with diffuse peritonitis. Abdollahi et al. [25] showed that patients with severe sepsis and septic shock had lower levels of serum lipid compared with patients without sepsis. Tanaka et al. [26] concluded that HDL levels were low in septic patients, whereas their concentration was not changed in trauma patients. The mortality was not associated with lipid levels in the sepsis group, and a significant negative correlation was found between HDL concentration and the length of ICU stay in the group of survivor septic patients at ICU discharge. Whitney [27] reported that total cholesterol might be a superior prognostic marker of mortality in patients with sepsis compared to Procalcitonin (PCT) and C-reactive Protein (CRP). Das, et al [28] ., also observed that the cholesterol level at the onset of sepsis (0 hour) could be an indicator of survival. The cholesterol level was changed and there was a positive association between low serum cholesterol levels, and increased mortality which agreed with the results of the presented study. Chiarla et al. [29] reported that hypocholesterolemia is often paralleled by low TG levels in surgical, sepsis, and critical illness patients. Fahila et al. [30] showed that the triglyceride value in the sepsis group was 120 ± 5.1 mg/dL on day 1, non-sepsis 117.53 ± 36.37 mg/dL. On the fifth day, in the sepsis group triglyceride values were 124.2 ± 50.29 mg/dL and the non-sepsis group triglyceride values 134.03 ± 68.12 mg/dL. They found no significant correlation between the severity of sepsis and triglyceride value in the patient with sepsis. Vyroubala et al. [31] reported very low levels of total cholesterol in polytrauma, after extensive surgery, in severe infections, in severe hypovolemic shock. Dunham et al. [32] concluded that hypocholesterolemia was observed after severe injury. Discharged patients had improved cholesterol levels, whereas dying patients had progressive hypocholesterolemia which went online with the results of the presented study. Wilson [33] reported that hypocholesterolemia observed following trauma. Lüthold et al. [34] showed that HDL-C and total cholesterol levels were lower in critically ill infected patients than they were in noninfected patients and this agrees with the results of the presented study and that no significant difference was seen in the serum TG level in critically ill infected patients when compared with noninfected critically ill patients which disagreed with the results of the presented study.
Conclusion
Cholesterol levels decreased markedly and triglyceride levels increased in patients with sepsis compared to non-septic patients and there was a significant difference between septic and nonseptic patients for cholesterol and triglyceride levels. The septic patients had a higher rate of mortality than the non-septic patients, in septic patients there was increasing in length of ICU stay, administration of vasoactive drugs, days on mechanical ventilation, higher qSOFA, and APACHE II scores compared to non-septic patients.
Recommendation
Since the mechanism which alters cholesterol and triglyceride level in the critically ill patients is not clearly identified so further studies in larger populations with lipid monitoring for longer duration are recommended.
Competing Interests
None declared.
References
- Gonçalves-Pereira J, Pereira JM, Ribeiro O, Baptista JP, Froes F, et al. (2014) Impact of infection on admission and of the process of care on mortality of patients admitted to the Intensive Care Unit: the INFAUCI study. Clin Microbiol Infect 20: 1308-1315.
- Angus DC, van der Poll T (2013) Severe sepsis and septic shock. N Engl J Med 369: 840-851.
- Wendel M, Paul R, Heller AR (2007) Lipoproteins in inflammation and sepsis. II. Clinical aspects. Intensive Care Med 33: 25-35.
- Wu A, Hinds CJ, Thiemermann C (2004) High-density lipoproteins in sepsis and septic shock: metabolism, actions, and therapeutic applications. Shock 21: 210-221.
- Cetinkaya A, Erden A, Avci D, Karagoz H, Karahan S, et al. (2014) Is hypertriglyceridemia a prognostic factor in sepsis? Ther Clin Risk Manag 10: 147–150.
- van Leeuwen HJ, Heezius EC, Dallinga GM, van Strijp JA, Verhoef J, et al. (2003) Lipoprotein metabolism in patients with severe sepsis. Crit Care Med 31: 1359-1366.
- Murch O, Collin M, Hinds CJ, Thiemermann C (2007) Lipoproteins in inflammation and sepsis. I. Basic science. Intensive Care Med 33: 13-24.
- Lee SH, Park MS, Park BH, Jung WJ, Lee IS, et al. (2015) Prognostic Implications of Serum Lipid Metabolism over Time during Sepsis. BioMed Research International 1-8.
- Barati M, Nazari MR, Taher MT, Farhadi N (2011) Comparison of Lipid Profile in Septic and Non-Septic Patients. Iran J Clin Infect Dis 6: 144-147.
- Gordon BR, Parker TS, Levine DM, Saal SD, Wang JC, et al. (2001) Relationship of hypolipidemia to cytokine concentrations and outcomes in critically ill surgical patients. Crit Care Med 29: 1563-1568.
- Vermont CL, den Brinker M, Kâkeci N, de Kleijn ED, de Rijke YB, et al. (2005) Serum lipids and disease severity in children with severe meningococcal sepsis. Crit Care Med 33: 1610-1615.
- Herzum I, Renz H (2008) Inflammatory markers in SIRS, sepsis and septic shock. Curr Med Chem 15: 581-587.
- Kruger PS (2009) Forget glucose: what about lipids in critical illness? Crit Care Resusc 11: 305-309.
- Barlage S, Gnewuch C, Liebisch G, Wolf Z, Audebert FX, et al. (2009) Changes in HDL-associated apolipoproteins relate to mortality in human sepsis and correlate to monocyte and platelet activation. Intensive Care Med 35: 1877-1885.
- López-Martínez J, Sánchez-Castilla M, García-de-Lorenzo A (2000) Hypocholesterolemia in critically ill patients. Intensive Care Med 26: 259-260.
- Levy MM, Fink MP, Marshall JC, Abraham E, Angus D, et al. (2003) 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit Care Med 31: 1250-1256.
- Knaus WA, Draper EA, Wagner DP, Zimmerman JE (1985) APACHE II: a severity of disease classification system. Crit Care Med 13: 818-829.
- Seymour CW, Liu VX, Iwashyna TJ, Brunkhorst FM, Rea TD, et al. (2016) Assessment of Clinical Criteria for Sepsis: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 315: 762-774.
- Remaley AT, Norata GD, Catapano AL (2014) Novel concepts in HDL pharmacology. Cardiovasc Res 103: 423-428.
- Kreeftenberg HG, Roos AN, Bindels AJGH, Scharnhorst V (2015) Cholesterol in the ICU: a cheap and reliable marker for illness severity? Neth J Crit Care 20: 17-20.
- Esteve E, Ricart W, Fernández-Real JM (2005) Dyslipidemia and inflammation: an evolutionary conserved mechanism. Clin Nutr 24: 16-31.
- Lekkou A, Mouzaki A, Siagris D, Ravani I, Gogos CA (2014) Serum lipid profile, cytokine production, and clinical outcome in patients with severe sepsis. J Crit Care 29: 723-727.
- Jeyasuriya A, Badrinath AK, Nagalingam S (2018) Cholesterol levels: the prognostic significance in ICU patients. Int J Adv Med 5: 652-657.
- Lee SH, Lee JY, Hong TH, Kim BO, Lee YJ, at al (2018) Severe persistent hypocholesterolemia after emergency gastrointestinal surgery predicts in-hospital mortality in critically ill patients with diffuse peritonitis. PLoS One 13: e0200187.
- Abdollahi O, Gohari A, Nobakhtrad M, Golshahi H (2016) Comparison of lipid profile changes in patients with severe sepsis and septic shock versus non-septic patients admitted to the medical ICU of Semnan Kosar Hospital and its association with hospital mortality from 2013 to 2014. Daneshvar Medicine 23: 25-32.
- Tanaka S, Labreuche J, Drumez E, Harrois A, Hamada S, et al. (2017) Low HDL levels in sepsis versus trauma patients in intensive care unit. Ann Intensive Care 7: 60.
- Whitney T (2015) Serum cholesterol: A Superior Prognostic Marker of Sepsis Mortality in the ICU Compared to Procalcitonin or Creactive Protein. School of Physician Assistant Studies pp: 528.
- Das S, Bhargava S, Manocha A, Kankra M, Ray S, et al. (2011) The Prognostic Value of Hypocholesterolemia in Sepsis. Asian J Pharma Bio Res 1: 41-46.
- Chiarla C, Giovannini I, Giuliante F, Zadak Z, Vellone M, et al. (2010) Severe hypocholesterolemia in surgical patients, sepsis, and critical illness. J Crit Care 25: 361.e7-361.e12.
- Fahila R, Kembaren T, Rahimi A (2018) The effect of bacterial sepsis severity on triglyceride value. IOP Conference Series: Earth and Environmental Science 125: 012074.
- Vyroubal P, Chiarla C, Giovannini I, Hyspler R, Ticha A, et al. (2008) Hypocholesterolemia in clinically serious conditions--review. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub 152: 181-189.
- Dunham CM, Fealk MH, Sever WE (2003) Following severe injury, hypocholesterolemia improves with convalescence but persists with organ failure or onset of infection. Crit Care 7: R145-R153.
- Wilson RF, Barletta JF, Tyburski JG (2003) Hypocholesterolemia in sepsis and critically ill or injured patients. Crit Care 7: 413-414.
- Lüthold S, Berneis K, Bady P, Müller B (2007) Effects of infectious disease on plasma lipids and their diagnostic significance in critical illness. Eur J Clin Invest 37: 573-579.

