Keywords
Health care; Health delivery; Private sector; Zimbabwe
Introduction
The private sector can be broadly defined as the part of a country's economic system that is owned, controlled and run by private entities, notably privately-owned enterprises incorporated under law (corporations) that are geared to making profits, or privatelyowned non-profit organizations and households [1]. The role and impact of the for-profit private sector in healthcare delivery, especially in low income countries, remains a highly-debated and contentious issue both from an ideological and practical perspective, with particular regard to healthcare equity and access issues. Empirical evidence has been presented over the years, for and against private sector participation in healthcare [2,3]; with critics arguing that private sector-run health facilities’ high prices limit the poor’s access to and use of health care facilities, thereby undermining healthcare consumption affordability, access and equity. Proponents of the private sector argue that it improves access and equity, and more efficient delivery practices by bringing in much needed resources whilst creating the space for government public health systems to increase focus on underserved populations. This argument however overlooks its impact on “healthcare market” segmentation as it selects for those who can afford against citizens who cannot. In addition some of these analyses ignore the funding, institutional and infrastructural roles played by the public sector in skills development which are ultimately leveraged by the private sector in their healthcare delivery systems [4,5]. Consequently, in health policy scholarship, an important consideration is whether and to what extent the relationship between public and private sectors is one of complementarity, substitution, competition or crowding out. Although some specific interventions designed to improve access and equity by participation of the private sector and other non-traditional actors have been shown to be successful and complementary to government efforts [3], there is a dearth of empirical evidence, especially from resource constrained national health systems on the appropriate role of the private sector in healthcare delivery. The lack of empirical evidence also extends to the link between motivations, procedures and impacts of private sector interventions with the overarching and broad national priorities and goals set out in healthcare strategies and policies [6].
In this paper we begin by assessing the assertion that entry of private sector actors into healthcare delivery improves health outcomes. We analyse evidence on the extent (if any) to which outcomes are led by, or in line with the national healthcare delivery objectives. We base our approach on the assertion that policy objectives can shape practice and interventions in economic sectors broadly [7] and apply the concept to the case of Zimbabwe’s healthcare delivery systems. We argue that understanding how policy shapes practice and interventions, especially in resource-constrained economic settings, provides an opportunity to reflect on how and whether synergistic mobilization as well as deployment of scarce resources can be optimized. Our analysis circumscribes healthcare provision to institutions that deal directly with patients for diagnostics and therapy; clinics, medical centres and hospitals, and does not extend to the broader healthcare delivery value chain which includes private sector players such as suppliers of medical health technologies (pills, vaccines or medical devices) and other ancillary inputs. We situate our analysis within the policy implementation context.
Using Zimbabwe’s 2009-2013 National Health Strategy and the WHO’s 6-factor health system building blocks, we focus on policy levers and frameworks that enable us to unpack and understand motivations, processes and impacts of private sector interventions in healthcare delivery. We discuss our methodology and research design, exploring the implications of the case study research approach and temporality for broader understandings of the role of the private sector in healthcare delivery in resourceconstrained low and middle income countries in section 2. We then present and analyse the interventions by the private sector in Zimbabwe’s healthcare delivery system in section 3. The final section (4) discusses the findings and explores ways of ensuring optimised, more predictable and sustainable outcomes from the private sector’s participation in healthcare delivery in resource-constrained environments.
What are the Health and Access Challenges Facing Zimbabwe?
Zimbabwe is a landlocked country in Southern Africa, bordered by Botswana, Zambia, Mozambique and South Africa. It has a population of 15 million and from a health perspective was one of the hardest hit nations by HIV/AIDS in the 1980s to 1990s where the prevalence rate was as high as 25% (ZIMSTAT, 2015), this has since reduced to around 13%, however new infections are still occurring. The Ministry of Health and Child Welfare has however instituted prevention of mother to child transmission (PMTCT) programme that has seen vertical infection drop. Figure 1 shows the impact of HIV/AIDS in terms of the top 25 causes of death in the country.
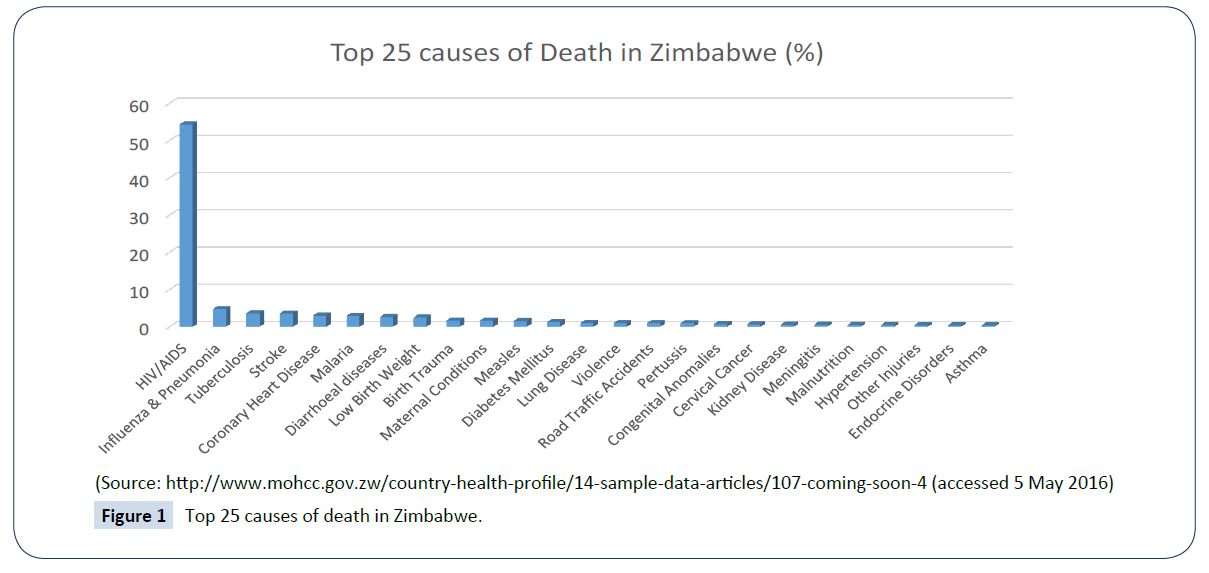
Figure 1: Top 25 causes of death in Zimbabwe.
By far the greatest challenge for the health sector is HIV/ AIDS (54.41%), followed by influenza and pneumonia (4.8%), tuberculosis (3.71%), stroke and coronary heart diseases (3.66%) as well as malaria (2.98%) as the leading causes of death. Funding and support for the HIV/AIDS therapy area has historically come from Global Health partners and locally from an AIDS levy and health budget. Other authors have described the burden that HIV/AIDS place on the health system especially since the late 1980s.
The onset of the economic challenges that began in the late 1990s and culminated in the hyperinflationary era of the 2000s strained the public health system. Fiscal provision for the public health system in real terms was reduced drastically and this forced citizens to resort to out of pocket health expenditure, and for those who were still gainfully employed medical insurance was the best option for accessing healthcare. With the gradual increase in unemployment the citizens depended more on out of pocket expenses or subscription of the elderly and other dependents onto medical insurance (cash subscriptions in addition to salary deductions) by on or offshore relatives or children.
Linkages amongst healthcare providers and service delivery platforms
Table 1 and Figure 2 shows the systemic linkages amongst actors and health seeking behaviour for people in rural, peri-urban and urban areas. The urban and peri-urban population’s primary point of contact for healthcare is the polyclinics which are managed by local government authorities (City Councils). The urban and periurban healthcare seekers can also access private healthcare in their locality; doctor’s surgeries or clinics with out of pocket or medical insurance payment methods. Medical insurance holder because of disagreements between clinicians and insurance companies usually pay a core payment which they claim from their insurance; with varying levels of re-imbursement.
| Health System Building Block |
Strategic Response and Guidance (National Health Strategy 2009–2013) |
| Selected Goal |
Target/Objective |
| Service delivery |
To increase coverage, access and utilization of affordable, comprehensive and quality preventive, curative and palliative health services |
Ensure full functionality of primary health care (PHC) system and Increased availability of functional infrastructure in underserved areas e.g. farming and rural communities |
| Health workforce |
Ensure that the PHC system has appropriate numbers and categories of human resources for health |
Implement a human resources strategy and reduce vacancy levels by 50%1 |
| Information |
Provide reliable, relevant, timely, reasonably complete and up-to-date information for managers at facility, district, provincial and national levels & increase utilisation of health research findings for decision-making |
Increase, strengthen and harmonise information generation and use. |
| Medical products, vaccines and technologies |
Increase availability of drugs, medical supplies and other consumables to 90%. Increase availability and functionality of medical equipment. Increase rational use of safe traditional medicines |
Develop and transfer appropriate technologies to underserved populations. Ensure 100% of all medicines and equipment are safe, efficacious and of good quality |
| Financing |
Increase the levels of predictable and sustainable funding base |
Mobilise more resources, improve use of existing resources & strengthen financial management systems2 |
| Leadership/Governance |
Improve health governance through strengthening formulation, implementation and review capacities |
Strengthen capacities in individuals and agencies, coordinate, ensure transparency, monitor, review and provide clear strategic direction for health |
1There had been a mass exodus of experienced health personnel into the region (South Africa, Lesotho and Swaziland) and abroad (UK, USA, Australia and New Zealand) especially from 2002 onwards, hence the high vacancy rates in the public health sector.
2This was in the context of the deteriorating macro-economic environment from year 2000 onwards and health budget was eroded by hyperinflationary pressures.
Source: Table developed by authors mainly from NHS [23] and WHO [12]. The table above summarises the separate but overlapping elements of the Zimbabwean health system as revealed by the WHO framework and the country’s 2009-2013 National Health Strategy. Zimbabwe’s National Health Strategy [24] was designed in a hyperinflationary environment when budgetary allocations to health lost value rapidly.
Table 1: Strategic responses for strengthening health system building blocks in Zimbabwe.
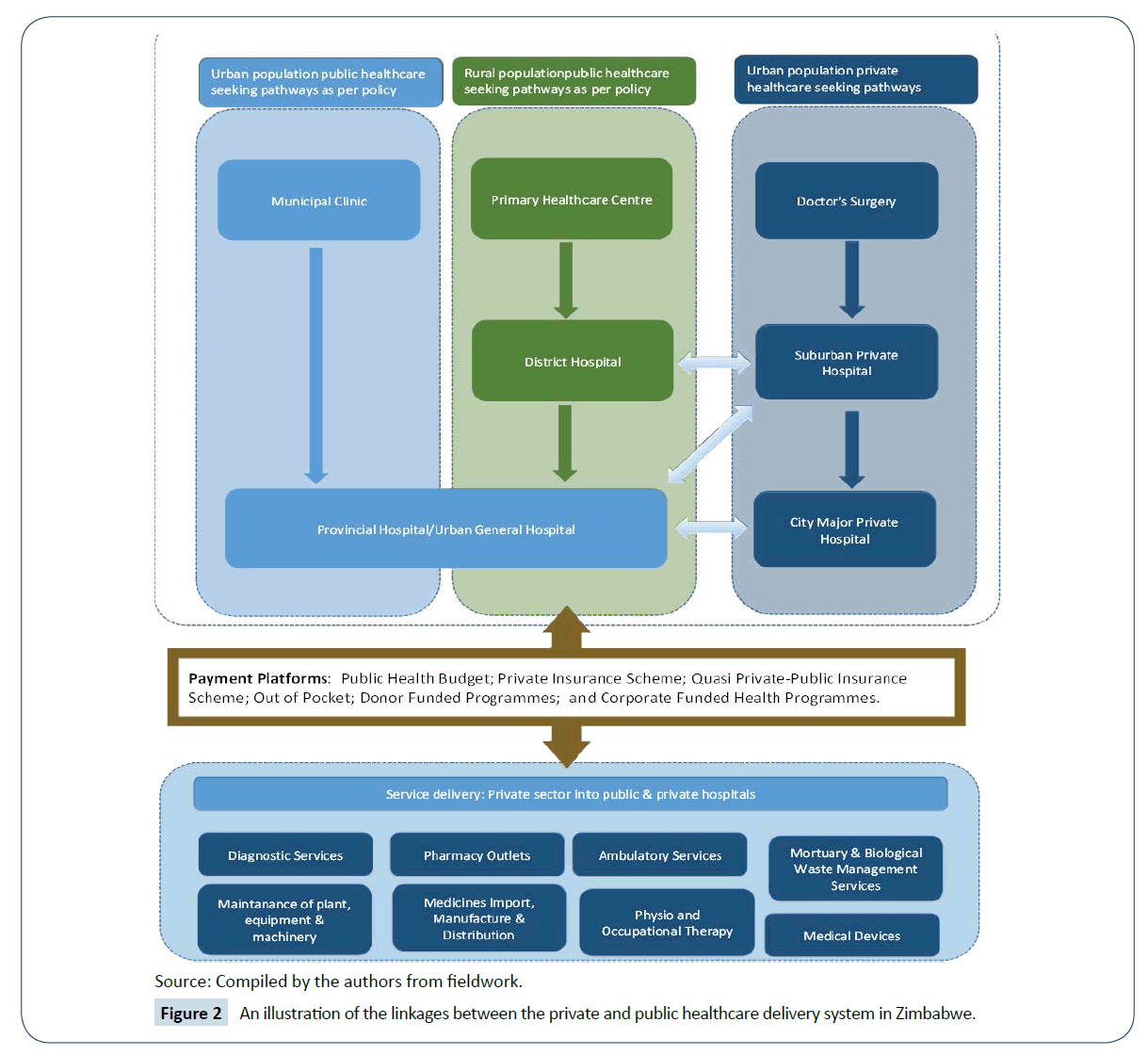
Figure 2: An illustration of the linkages between the private and public healthcare delivery system in Zimbabwe.
Thus with respect to adding value, the private sector has many entry points over and above financial resources. As Figure 2 shows, the private healthcare sector is not a homogeneous grouping, and in Zimbabwe, a wide range of private sector players exist, which include doctor’s surgeries, private hospitals, church-run mission hospitals, pharmaceutical companies, health insurers, mobile phone operators and mining companies, with varying combinations of for-profit and not-for-profit motives.
Policy Implementation and Evaluation
Turning to the theoretical framing of our argument, Walt et al. [6] argue that theory deployment in health policy research could benefit public policy practice by deepening our understanding of causality, and by bringing coherence to fragmented policy analysis. We situate this paper in the policy analysis terrain especially within the realms of policy implementation and evaluation, by focusing specifically on how health strategies and policy shape and are shaped by practice. Motivated by practical concerns, and a criticism against health policy research, this analysis points out some implementable recommendations while, as Hunter [8] cautions ‘‘avoiding a reductionist policy quick ‘fix’. The analysis contends with other conceptual challenges on how to ‘do’ policy analysis, such as capturing and measuring levels of resources, values, beliefs and power of diverse actors which are very difficult. ‘Power’ in particular is both a fundamental but highly contested concept in policy implementation and policy analysis [6].
Influential theories of the public policy process include multiple-streams [9], punctuated-equilibrium [10] and top-down and bottom-up implementation [11]. Theories are more specific than frameworks, and postulate precise relationships among variables that can be tested or evaluated empirically. For this analysis we use frameworks; we focus specifically on policy implementation, and use Zimbabwe’s National Health Strategy and the WHO [12] health system building blocks as useful frameworks for identifying and organising the inquiry into elements and the relationships amongst these elements that need to be considered. We are cognisant of the fact that, as aptly noted by Schlager [13], frameworks do not, of themselves, explain or predict behaviour and outcomes.
Multiple implementation theories have been dominated by a discourse revolving around whether decision-making is top-down or bottom-up, or a synthesis of the two [11]. For example, Dye [14] argues that even in a democracy like the United States, public policy is made from the top down, not from the bottom up. In his view, public policy reflects the values, interests and preferences of the governing elite. Dye [14] separates policy development from implementation, admitting that bureaucrats may affect policy in implementation, but suggesting that all decisions are monitored to ensure they are not altered significantly. Lipsky [15], on the other hand, describes implementation of policy as highly influenced by ‘street level bureaucrats’; front-line staff who can change policies significantly, and others have developed this approach [16]. Much of the literature focuses on the gap or deficit between policy objectives and actual implementation [17].
Saetren [18] on the other hand reviewed then all implementation literature published and concluded that while most of the studies focused on health and education, they were predominantly of high income, Western countries; underscoring the need for theory development for low and middle income settings that takes into account economic, geographic, cultural and other realities. There are however a few notable exceptions [19] and our paper contribute towards filling that empirical gap. We do this by focusing on how multiple sector responses to healthcare challenges in a resource-constrained environment are driven by and impact policy objectives.
Methodology
Using Zimbabwe’s 2009-2013 National Health Strategy as a lens for identifying priority areas for intervention and therefore the arenas for analysis of expected and unexpected impact, this paper examines whether and how the participation of the private sector in health delivery adds value to the health system in general, and in particular how this value relates to the country’s health delivery objectives and targets as set out by the National Health Strategy and health-related policies. Situated within a project studying health spending innovations1 in South Africa and Zimbabwe, the latter was chosen as a specific case for this paper because, between the two countries in the bigger study, the acute resource challenges Zimbabwe is facing and the responses in such a scenario offered greater potential explanatory value and insights on policy effectiveness in such environments. A case study approach was chosen to allow in-depth investigations of [this] single instance of a phenomenon in its real-life context [20]. We also grappled with the question: what is it a case of [21]? Our take was that this was in many interconnected ways an example of health policy implementation success and/or failure; of collaboration between private sector and government in health delivery broadly; of health policy influence on agenda (re)setting by different players; and of the political, professional and economic factors that influence resource deployment and health policy evaluation. Identifying our case, what it is a case of and why this case was useful to study helped us to select the tools and theories that could frame our analysis and determine the methods to be used in the analysis. This analysis carried out a documentary review of government policies, records, reports and health sector bulletins produced by and available at the MoHCC, stakeholder annual reports and newsletters as well as media reports to identify and evaluate the roles and contributions of different private sector actors in health delivery in Zimbabwe.
The following section presents and discusses these roles in the backdrop of the empirical lens presented in Table 1 above.
Results and Analysis
Since independence in 1980, and increasingly in the last 10 years, Zimbabwe has had a number of international organizations and donors, international and local corporate actors, civil society organisations and other non-state actors playing significant roles in health delivery. Lately this has been in response to the fact that Zimbabwe’s once vibrant health system still suffers from the effects of a prolonged economic meltdown which has left the extensive network of hospitals, clinics and other health service centres severely incapacitated in terms of personnel, equipment and drug supplies [22].
In the face of medical staff vacancy rates of up to 70% in some public health facilities; increasing public health significance of chronic non-communicable diseases (NCDs) such as diabetes, hypertension and cancers; high maternal and child mortality rates; declining though still-high HIV/AIDS infection and TB morbidity rates; physical infrastructure for health in a state of disrepair [23,24]-it is hardly surprisingly that most of the country’s health indicators have deteriorated significantly in the last decade, and that like most African countries, Zimbabwe missed the health-related MDG targets2 [24]. In addition to the persistent challenges in all the health system building blocks, and a lens of particular interest for this paper, health governance is generally a challenging area for Zimbabwe, and other developing countries, especially given the brain drain of health staff to the private sectors and mostly to developed nations. The country experienced a high exodus of health personnel, especially nurses to the UK from 1997 peaking around 2002 when the UK actively recruited health personnel from Zimbabwe. This reflects the losses from the initial gains through free health and free education that heralded Zimbabwe’s social transformation miracle in the early 1980s [25]. Consequently through the then Ministry of Health and Child Welfare (MOHCW) now Ministry of Health and Child Care (MOHCC), the country put in place measures to ‘give strategic direction in health sector [re]development’, notably the National Health Strategy 1997-2007, which was succeed at the end of 2009 by the National Health Strategy 2009-2013. Additionally, a Patients’ Charter, originally developed in 1996, was revised and a new version was distributed in early 2011 to serve as a framework for how clients should be treated throughout the health system, and it defines the responsibilities/rights of clients/ patients within the health system [26]. As a result of the persistent and growing economic and brain drain challenges during the hyperinflation era, the National Health Strategy 2009-2013 recognised the need for ‘inclusive implementation and working together’, and recognised the roles that communities, ‘missions’ and local authorities, private sector and funding partners played and would continue to play in service provision and financing. They acknowledged that because some of the arrangements were ad hoc and informal and ‘since some of these resources would not flow through government channels, there would be obvious difficulties in tracking them and monitoring their use [21]. The foreign currency fiasco exemplifies some of these issues and resulted in global funds for HIV programme moneys being handled by UNDP and not the Ministry of Health and Child Care (MOHCC Interview, 2014).
The private healthcare sector footprint and funding in Zimbabwe
The private sector has historically been active in Zimbabwe and initially catered for the upmarket clients mainly on health insurance through Medical Aid Societies. However with the advent of independence and an expansion in training capacity of medical doctors, there was an increase in private surgeries that catered for the low-income urban populace, living in the so-called ‘high-density’ suburbs. With increasing entrepreneurial activity private hospitals were constructed in major cities and towns. Munyuki and Jasi showed that growth in private hospitals increased tremendously from 14 in 1991, to 209 in 1996, whereas private specialist centres increased modestly from 6 to 13 in the same period. Church related hospitals/clinics on the other hand increased from 97 to 128 in the same period. To put these numbers in perspective, the public healthcare statistics for the same period (1991-1996) were follows: Central Hospitals; rose from 4 to 5, General Hospitals were static at 7; State Clinics reduced from 377 to 349, Provincial Clinics increased from 452 to 497 and Municipal Clinics increased from 102 to 105 and fell back to 102.
Evidencing the growing impact of the sector, the Private Hospitals Association of Zimbabwe (PHAZ) was formed in 1996, and the founding members were The Avenues Clinic (Harare), St Annes Hospital (Harare), Borradale Hospital (Marondera), Seventh Avenue Surgical Unit (Mutare), Claybank Clinic (Gweru) and Colin Saunders (Triangle)3. PHAZ has grown from the initial four members to thirty five with 1500 hospital beds. The portfolios covered by the members include hospitals; for example Mater Dei (Bulawayo) and South Medical (Chitungwiza); clinics, medical insurance firms’ own clinics, maternity hospitals, 24 hrs accident and emergency centres, and specialist centres such as Harare Haemodialysis Centre.
The growth of private healthcare centres was underpinned by an extensive private sector health insurance system, through what is locally known as Medical Aid Societies. Underscoring the message that the private sector has a long history in healthcare in Zimbabwe, the first association of medical health insurers, the National Association of Medical Aid Societies (NAMAS) was formed in 1969. NAMAS became Association of Healthcare Funders of Zimbabwe (AHFoZ) in 2004 when it embraced other funders besides medical aid societies. Premier Medical Aid Society (PSMAS) is one of the oldest funders in the country having been established in 1930 after appointment of a special committee by the Public Service Association4. PSMAs grew from a membership of under a thousand in 1931 to over 600000 members today, and it caters mostly for civil servants.
Medical Aid works on the basis of employer and employee monthly contributions and the delivery platform is segmented according to net-worth or contribution; there are general, private and executive statuses with varying re-imbursement values and healthcare service access. There are currently twenty one medical insurance organisations5 which belong to the (AHFoZ), and ownership of the organisations range from municipal, private (including financial services players), pension funds and quasi-public institutions. However the economic challenges of the last decade have affected AHFoZ which reported loss of 4 members due to viability challenges [27]. Table 2 below summaries some of the work being done by the private sector in Zimbabwe’s health sector, the private sector here comprising all actors who exist outside the public sector, whether their aim is philanthropic or commercial.
| Health system building block |
Stakeholders and their interventions |
Impact |
Existing gaps |
| Service delivery |
Individuals and consortia setting up private hospitals, private clinics and private wards in public hospitals |
Improved service provision in most urban and provincial hospitals. |
Populations in rural and farming communities still underserved |
| Health workforce |
Medical school bursaries by some mobile phone companies and health insurers and health staff retention allowances by bilateral and multilateral donors |
Stabilisation of staff numbers, morale and skills levels in some health facilities |
Staff retention mainly in urban facilities. There is also unequal burden sharing between health facilities in that government trains and loses staff to private health sub-sector. Underfunded MOHCW unable to absorb all trained nurses. Emigration of junior doctors due to poor emoluments |
| Information |
Support from mobile phone companies for health information systems, solar energy and internet connectivity at rural hospitals across the country |
Up to 80% of rural hospitals and clinics able to provide and access information instantly |
Some rural and farming communities still lack infrastructure for internet and would benefit from resuscitation of abandoned technologies such as radio communication systems |
| Medical products, vaccines and technologies |
Support by multilateral donors for decentralisation of screening and treatment services for NCDs |
Specialist NCD centres mainly in major cities Harare and Bulawayo. |
Disconnect between diagnosis and treatment e.g. chemotherapy still centralised and costly |
| Financing |
Public and private medical insurance schemes to cover user fees |
Country has 33 medical insurance providers, with diverse and innovative packages that include individual and family packages, which allow access to different categories of health facilities |
Only 10% of the Zimbabwe’s 15million population has medical aid cover; the urban and rural poor cannot access specialist health care unless they can pay for it out-of-pocket |
| Leadership/Governance |
Multilateral donor, civil society and corporate sector support of the review of the Public Health Act |
Public Health Act 15:09 now in place, emphasising need for broad-based stakeholder awareness and collaboration |
Awareness-raising efforts on Act and other strategies are under-resourced, not widely spread and ad hoc, hence many social and institutional actors remain unaware of their role in implementation |
Table created by authors with data from Chinyadza [28], Mugwagwa [29], ZIMSTAT [24], NHS [23] and TARSC [30]. Highlighted in the 4th column are some areas which stand in stark contrast with the National Health Strategy goal of universal coverage and equitable access to quality health care.
Table 2: Examples of private sector involvement in Zimbabwe’s health system (2013–2015).
Emerging private sector partnership principles
The evidence above confirms the active involvement of private sector actors in health delivery in Zimbabwe. This reality is both good for the health system and various actors in it, as much is it creates some expected and unexpected vulnerabilities in the health delivery system. The Table 3 below captures an analysis of some of the emerging opportunities and vulnerabilities from the partnerships above, looking specifically at three areas namely, motivations, procedures and impact.
| Principles |
Motivations |
Procedures |
Impact |
| Opportunities |
Coordinate overall motivations around broader health delivery and socio-economic imperatives |
Develop agile and user-friendly policy guidance to coordinate, document, standardize and deploy responses |
Trail and accumulate real-time impact from multiple and intermittent responses |
| Vulnerabilities |
Actors not motivated when their motivations and contributions are swallowed in ‘big pictures’; and in a constrained environment they have more power to hold on to their motivations |
Reflection on procedures is time and resource-consuming, more so in a an environment already constrained for both |
Access takes precedence over quality and cost of service. Health system users more concerned with at least being able to access health service providers. Government and consumer watchdogs less able to protect consumers because of preoccupation with other priorities |
Table 3: Emerging opportunities and vulnerabilities for health partnerships in Zimbabwe.
Discussion
Elusive challenges and multiple players
The data presented and analysed here not only shows that the private sector is playing active and diverse roles in various aspects of health delivery in Zimbabwe, but that in addition and resulting from that, there are opportunities and vulnerabilities that are emerging which this paper unpacks to understand how they relate to the country’s health delivery objectives.
The findings confirm that indeed private sector participation in Zimbabwe covers the six building blocks of the health system, though the ‘information mechanisms’ block is the one most dominant. There are both commercial and philanthropic motivations for the entry of the different players in the health delivery arena, resulting in multiple procedures for delivery of activities, and different impacts from the activities. This is hardly surprising, and not in itself the problem, but what seems to lack is documentation and standardization of the procedures to link motivations and impact.
One way to ensure this link would be through the guidance of the country’s health strategy and policies, but there are a number of inherent and transcendent challenges which include limited human resource capacity in the Ministry of Health and Child Care (MOHCC) to ensure compliance of stakeholder activities with policy objectives; limited financial capacity in the MOHCC to support continuous appraisal of interventions for alignment with policy objectives; the financial power of private sector players which allows them to by-pass procedures; historical and on-going poor usage of results of evaluation processes which result in stakeholders not paying much attention to the need for evaluation and alignment of procedures; the reality that indeed the resource and intervention space is severely constrained, to the extent therefore that any intervention that comes into the fray not only has potential to make a genuinely important and much needed impact, but also comes in the backdrop where due diligence processes may be seen as undesirable efforts to frustrate timely interventions. The observations therefore are that while the policies and strategies in place encapsulate the desirable vision for health delivery in the country, they lack the agility to guide a process in which resource availability is ad hoc and intermittent, and where implementation of activities is largely on an ‘as and when resources become available’ basis, making it a huge challenge for delays to be desirable or acceptable. In a resource-constrained environment, the chances of resources being diverted to other causes are high and real, pushing reflection and alignment to policy to the periphery. In fact, it becomes clear in this case that practice is being directed by the realities on the ground [15], and that while there is not necessarily a mismatch between policy objectives (or direction) and the practice responses, the mismatch exists on the pace with which responses have to be ushered. The absence of single large private sector players with big enough resource endowments to fill the gap also means there will (of necessity) be multiple players responding to the challenge, at different time periods, at different points in the health system, and in different geographical locations, making standardization of procedures difficult, if not impossible when the backdrop of constrained health ministry staff numbers and financial resources are factored in.
Our analysis provides evidence to show that beyond immediate positive outcomes on one hand, and the usual worries about cost of health provision as a result of participation by private sector actors on the other [6], the debate about the appropriate role of private sector participation in health delivery in severely constrained resource environments presents unique sets of challenges and opportunities for policy responses, not at the visionary level, but with respect to emergence of agile guidance on how to attain the vision within the reality of multiple responses. While standardization remains both good and desirable for the multiple funders, for policy makers and for patients, balancing the requirement for that with timely and life-saving responses becomes the main requirement. We observe that policy guidance falls short where it hinges on policies not agile enough to direct a dynamic practice, necessitating the need for ‘policy implementation as unusual’ approaches which balance pace of response with quality of delivery. The appropriate role of the private sector will thus depend on the capacity of governments to provide agile stewardship, regulation and organisation of the health sector in a health care financing environment which is unpredictable. Innovative ways of harnessing the motivations, responses and impacts at different levels of the various actors will thus go a long way in ensuring acknowledgement, relevance and user-shaping of the service delivery space. Devolving decision-making authority and capacity to the lowest levels possible across the health delivery system while ensuring system-wide cohesion will be key.
Conclusion
In the face of mounting challenges in health delivery, the Zimbabwean government sees the private sector as important partners in the quest for increased access to health by the country’s population. This paper has provided and analysed evidence confirming that the Zimbabwean healthcare ‘puzzle’ is made up of ‘pieces of different sizes, forms and shapes’, and the puzzle will be complete to the extent that all the pieces are available and in their proper place. Evidence presented in this paper highlights that indeed collaboration between government and private sector in health delivery is both desirable and necessary given the shrinking resource base for health delivery which has further weakened an already stretched health system facing multiple political, economic and social difficulties. The government has put in place the National Health Strategy and various programmes to direct and institutionalise stakeholder participation in health delivery, maintain the momentum of public-private cooperation and create an enabling environment for those who want to come aboard. Monitoring of alignment of the motivations, procedures and impacts of private sector participation in health delivery is however hampered by the intercalated constraints of funding, human resources and time. We conclude therefore that while broadened participation by the private sector evidently results in some favourable intermediate outcomes in terms of access and equity, there is need for systematic documentation and standardisation of the various procedures and approaches employed by the different actors, in order for their motivations to be aligned with the government’s health delivery goals and for more predictable, scalable, measurable and sustainable impact from these interventions to emerge. This will not only help avoid possible deleterious links (e.g. wastage of much needed resources through overlaps and duplications) between private sector participation and health system performance in the country, but will ensure timely decision-making, curation and deployment of required institutionalisms and identification of synergies that are good for government, health facilities, patients and the new actors coming on board.
Acknowledgements
Dr Julius Mugwagwa acknowledges funding by the ESRC Future Research Leaders Fellowship grant number ES/K001442/1 which supported this work and the intellectual support from colleagues in the Development Policy and Practice Group at The Open University and numerous health sector stakeholders in Zimbabwe. Dr Geoff Banda is grateful for support from the Innogen Institute and Science, Technology and Innovation Studies (STIS), University of Edinburgh.
1ESRC Future Research Leaders Fellowship grant number ES/K001442/1, project title: ‘Innovative spending: what should money be spent on to make global health innovations more effective in developing countries?’
2https://www.newsday.co.zw/2013/05/13/zim-misses-mdg-targets/
3https://www.phaz.co.zw/
4https://www.ahfoz.org/testimonial-view/psmas/
5https://www.ahfoz.org/members/
References
- Lienert I (2009) Where does the public sector end and the private sector begin? IMF Working Paper WP/09/122.
- Yoong J, Burger N, Spreng C, Sood N (2010) Private sector participation and health system performance in Sub-Saharan Africa. PLoS ONE 5: e13243.
- Patouillard E, Goodman C, Hanson K (2007) Can working with the private sector improve access of the poor to quality health services? A systematic review of the literature. Int J Equity Health 7: 6-17.
- Peter B (1998) Rethinking health care systems: private health care provision in India. World Development 26: 1463-1479.
- International Finance Corporation (2007) The business of health in Africa: partnering with the private sector to improve people’s lives.
- Walt G, Shiffman J, Schneider H, Murray SF, Brugha R, et al. (2008) ‘Doing’ health policy analysis: methodological and conceptual reflections and challenges. Health Policy Plan 23: 308-317.
- Bassanini A, Scarpetta S, Hemmings P (2001) “Economic Growth: The Role of Policies and Institutions: Panel Data. Evidence from OECD Countries”, OECD Economics Department Working, OECD Publishing, p: 283.
- Hunter DJ (2003) Evidence-based policy and practice: riding for a fall? J R Soc Med 96: 194-196.
- Kingdon JW (1984) Agendas, alternatives and public policies. Boston, MA and Toronto: Little, Brown and Company.
- Baumgartner FR, Jones BD (1993) Agendas and instability in American politics. Chicago and London: The University of Chicago Press, USA.
- Sabatier PA (2007) Theories of the policy process. Boulder, CO: Westview Press.
- WHO (2007) Everybody’s business: strengthening health systems to improve health outcomes: WHO’s framework for action. World Health Organisation, Geneva, Switzerland.
- Schlager E (2007) A comparison of frameworks, theories, and models of policy processes.
- Dye T (2001) Top down policy making. New York & London: Chatham House.
- Lipsky M (1980) Street-level bureaucracy: dilemmas of the individual in public services. New York: Russell Sage Foundation.
- Hjern B, Porter DO (1981) Implementation structures: a new unit of administrative analysis. Organ Stud 2: 211-227.
- Hill MJ, Hupe PL (2002) Implementing public policy: governance in theory and practice. London: Sage.
- Saetren H (2005) Facts and myths about research on public policy implementation: out-of-fashion, allegedly dead, but still very much alive and relevant. Policy Stud J 33: 559-582.
- Kamuzora P, Gilson L (2007) Factors influencing implementation of the community health fund in Tanzania. Health Policy Plan 22: 95-102.
- Yin R (1994) Case study research: design and methods (2nd edn.). Thousand Oaks, CA: Sage Publications
- George AL, Bennett A (2004) Case studies and theory development in the social sciences. Cambridge, MA: MIT Press.
- Mugwagwa J (2013) Innovative spending in health: Evidence from South Africa and Zimbabwe. Innovation and International Development.
- National Health Strategy for Zimbabwe (2009-2013) Equity and quality in health: a people are right. Ministry of Health and Child Welfare, Zimbabwe.
- Zimbabwe National Statistics Agency (ZIMSTAT) (2015) Zimbabwe multiple indicator cluster survey 2014, Final report. Harare, Zimbabwe.
- Davies R, Ratso J (2000) Zimbabwe: Economic adjustment, income distribution and trade liberalization. Centre for Economic Policy Analysis, New School University, NY, USA.
- Osika J, Altman D, Ekbladh L, Katz I, Nguyen H, et al. (2010) Zimbabwe health system assessment 2010. Bethesda, MD: Health Systems 20/20 Project, Abt Associates Inc.
- Sanyanga S (2015) Surviving with adversity in the healthcare sector. Private Hospital Association of Zimbabwe (PHAZ) Conference, Victoria Falls, Zimbabwe.
- Chinyadza JK (2014) How the private sector adds value in health. Presentation made at the Association of Healthcare Funders of Zimbabwe Annual Conference, Victoria Falls.
- Mugwagwa J (2014) Innovative spending in health: a case study of Zimbabwe, South Africa and United Kingdom, Presentation made at the Association of Healthcare Funders of Zimbabwe Annual Conference, Victoria Falls.
- Training and Research Support Centre (TARSC) (2015) Implementers training on the Public Health Act Chapter 15:09, Training workshop report.

