Ismail KA1,2*
1Faculty of Medicine, Department of Parasitology, Ain-Shams University, Cairo, Egypt
2Faculty of Applied Medical Science, Department of Medical Laboratory, Taif University, Taif, Saudi Arabia
*Corresponding Author:
Ismail KA
Faculty of Medicine, Department of Parasitology
Ain-Shams University, Cairo, Egypt and Faculty of Applied
Medical Science, Department of Medical Laboratory
Taif University, Taif, Saudi Arabia
Tel: +966 12 727 2020
E-mail: khadigaahmed68@yahoo.com
Received Date: April 10, 2018 Accepted Date: April 27, 2018 Published Date: May 02, 2018
Citation: Ismail KA (2018) Prevalence of Intestinal Parasitic Infection among School Children in Taif. Insights Biomed. Vol.3 No.2:10 doi: 10.21767/2572-5610.100045
Keywords
Intestinal parasitic infection; Giardia duodenalis; Mental health; School children
Introduction
Intestinal parasitic infections are global in distribution and particularly endemic in developing countries [1,2]. The high prevalence in developing countries are due to lack of sanitation, lack of access to safe water and improper hygiene; therefore, they occur wherever there is poverty. People of all ages are affected by this cycle of prevalent parasitic infections; however, children are the worst [3,4].
Giardia lamblia, causing giardiasis, is the most prevalent protozoan parasite which affects about 200 million people being currently infected [5,6]. About 3.5 billion people are affected, and that 450 million are ill as a result of these infections [7]. These infections are considered as a serious public health problem, as they cause growth retardation in children and other physical and mental health problems [8].
There is association between malnutrition and intestinal parasitism and the correlation between nutritional status and both prevalence and intensity of infections [9]. Malnutrition may affect children development, affecting even cognitive function and school performance of children [10]. Also, acute complications such as intestinal obstruction, severe anemia [11].
In Saudi Arabia studies revealed high prevalence rates of infection with intestinal parasitic diseases among specific populations including food handlers (14%), Riyadh school children (14.2%), expatriates (55.7%) [12]. In spite of a great development in healthcare, the problem of parasitic infections continues to be widely distributed in tropical and subtropical areas, especially in poor populations [13]. Asymptomatic carriers of intestinal parasites are considered as public health hazard, especially if they work in catering facilities, where they may become a source of infection for others [14].
Amoebiasis is the third leading cause of death from parasitic diseases worldwide, with its greatest impact on the people of developing countries. According to World Health Organization (WHO) showed that approximately 50 million people worldwide suffer from invasive amoebic infection each year, resulting in 40- 100 thousand deaths annually [15].
Cryptosporidiosis is becoming the most prevalent in both developed and developing countries among immunocompromised patients with AIDS and among children aged less than five years. Several outbreaks of diarrheal disease caused by Cryptosporidium parvium have been reported during the last decade [16]. fecal contamination transmits this parasite as a result of poor sewage and poor quality of water. Food and water-borne outbreaks of these protozoan parasites have occurred, and the infectious oocyst form of the parasites is relatively resistant to chlorine [17].
Amebiasis can cause both intestinal and extraintestinal disease spread [19]. These intestinal parasites exhaust nutrients from children they infect, thus retarding their physical development. They destroy tissues and organs, cause abdominal pain, diarrhea, intestinal obstruction, anemia, ulcers and other health problems which can lead to slow cognitive development and impaired learning [20].
So, the aim of our study is to detect prevalence of parasitic intestinal infection among primary school children.
Materials and Methods
Study type, site and duration
Descriptive cross section study was conducted in Taifg overnorate, western Saudi Arabia during the period from September 2017 to Janury 2018. The city lies on an elevation of 1,879 m on the slopes of Al-Sarawat Mountains. It accommodates a population of 1,200,000 people comprising Saudi Arabians and significant foreign populations, primarily from Asia, Africa, and other Arab countries. The city has a hot desert climate, with hot summers and mild winters. Children under the study had age range from 4–14 years,100 males and 50 females.
Ethics Consideration
This research was approved by the Research Ethics Committee of College of Applied Medical Sciences, Taif University.
Study Methodology
Sample collection and processing
Fresh stool samples were collected in appropriate containers from 150 children and submitted to the College of Applied Medical Science laboratory. Inside the laboratory, stool samples were individually inspected for consistency and the presence of mucous or blood, Intestinal parasites, trophozoites and cysts were looked for through microscopic examination of wet mount and formalin-ether concentrated fecal preparations. Detection of intestinal protozoa was performed systematically on each sample using iodine, modied Ziehl–Neelsen and Trichrome stained preparations.
Statistical analysis
Collected data were numbed, coded, and introduced to a computer using the Statistical Package for Social Science for Windows version 19 The x2 test was used to analyze the frequency of parasitic infection with outdoor food consumption in the study group to clarify statistically significant differences (Table 1 and Figure 1). A value of P<0.05 was considered statistically significant, and value of P<0.001 was considered statistically highly significant (Figures 2 and 3).
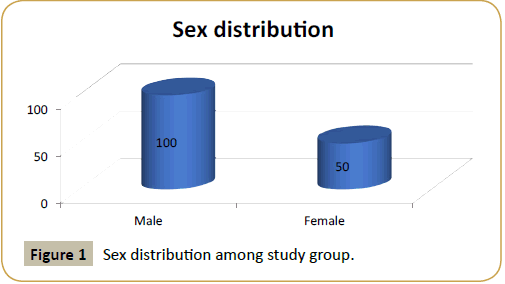
Figure 1: Sex distribution among study group.
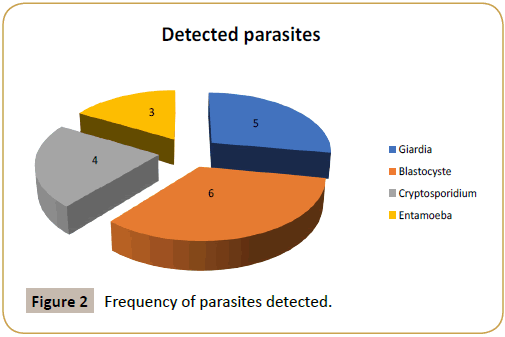
Figure 2: Frequency of parasites detected.
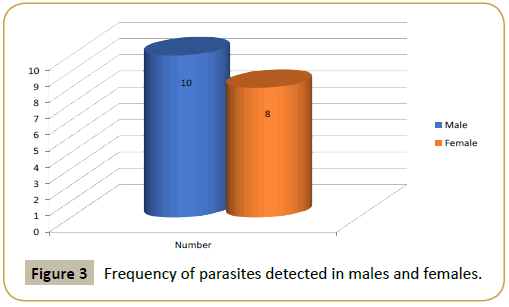
Figure 3: Frequency of parasites detected in males and females.
| Study samples |
No.
(150) |
Presence of intestinal parasites |
X2 |
P-value |
| Positive No. ( %) |
Negative No. ( %) |
| Outdoor food consumer |
45 |
13(28.9%) |
32(71.1%) |
15.529 |
P=3.08
Non-significant |
| Indoor food consumer |
105 |
5 (4.6%) |
100(95.4%) |
Table 1: Frequency of parasites detected in outdoor food consumer and indoor one.
Results
Descriptive cross section study among Taif primary school randomize samples were chosen age range is from 4-14 years.
Discussion
The most common parasitic causes of gastroenteritis are Giardia lamblia, Cryptosporidium parvum and Blastocystes hominis which will be discussed in this research similar. The purpose of parasite detection is not limited to curing disease in an infected individual, but it is crucial in the prevention and spread of diseases. For these reasons, improving detection methods with high both sensitivity and specificity [21].
Cryptosporidiosis occurred more frequently among children less than 7 years of age, and particularly in the first two years of life [22]. This go with our result which detect Cryptosporidium in young age group with prevalence of 3%.
Infection may occur via contaminated material such as earth, water, uncooked or cross-contaminated food that has been in contact with the feces of an infected individual or animal [23].
Giardia lamblia is broad worldly distributed, being detected in both developing and developed countries. It is the most commonly reported human intestinal parasite, with prevalence rates reaching 2 to 7%, in the developed countries. The prevalence rates may reach 20 to 60% in some areas in the developing countries [24]. This go more or less with our result which is 3% of examined specimens. Some people may present the asymptomatic form, others an acute or chronic diarrhea that can last for several months with mal-absorption syndrome and weight loss. Giardia lamblia is usually pointed as one of the causes of children ‘s retarded growth and development [25].
Blastocystis hominis infection is widely distributed all over the world with a high prevalence in countries in the tropics and subtropics regions. Its prevalence may exceed 50% in developing countries and reach 20% in industrialized countries. Human infection is associated with poor personal hygiene, lack of sanitation, continues exposure to animals, and consumption of contaminated food or water. Transmission of Blastocystis is suggested to be by the fecal–oral route, for example, via contaminated water or food, with sources being both humans and animals [26]. This controversy with our result which is 4% of cases have Blastocystis hominis may be due to young age group under our study.
Although around 10 percent of the world's population is infected with Entamoeba histolytica, about 90 percent of infected persons are asymptomatic [18]. This controversy with our result which is 2% of cases have Entamoeba histolytica may be due to young age group under our study.
Conclusion
Gastrointestinal parasitic infection was one of the most prevalent public health problem among Taif primary school children. Therefore, the local health office and other governmental and non-governmental organizations need to give attention to this serious problem of theses parasitic infection of school children. As it leads to growth retardation and bad school achievements so implementation of national program of early detection of intestinal parasites infection especially in asymptomatic children is mandatory.
References
- Steketee R (2003) Pregnancy, nutrition and parasitic diseases. J Nutr 133: 1661–1667.
- Garzon M (2003) Capital university of integrated medicine. Parasites-A holistic approach. In: Associates NIH, editor.
- Curtale F, Pezzotti P, Sharbini A, Al Maadat H, Ingrosso P, et al. (1998) Knowledge, perceptions and behaviour of mothers toward intestinal helminths in upper Egypt: Implications for control. Health Policy Plan 13: 423–432.
- Bethony J, Brooker S, Albonico M, Geiger SM, Loukas A, et al. (2006) Soil-transmitted helminth infections: Ascariasis, trichuriasis, and hookworm. Lancet 367: 1521–1532.
- Pillai D, Kain K (2003) Common intestinal parasites. Curr Trea Options Infect Dis 5: 207–217.
- Minenoa T, Avery M (2003) Giardiasis: Recent progress in chemotherapy and drug development. Curr Pharm Des 9: 841–855.
- Keiser J, Utzinger J (2010) The drugs we have and the drugs we need against major helminth infections. Adv Parasitol 73: 197–230.
- Evans AC, Stephenson L (1995) Not by drugs alone: The fight against parasitic helminths. World Health Forum 16: 258–261.
- Quihui-cota, L, Valencia, M, Crompton, D (2004) Prevalence and intensity of intestinal parasitic infections in relation to nutritional status in Mexican school children. Trans Roy Soc Trop Med Hyg 98: 653-659.
- Olness K (2003) Effects on brain development leading to cognitive impairment: A worldwide epidemic. J Dev Behave Pediat 24: 120-130.
- Safiri S, Kelishadi R, Qorbani M, Lotfi R, Djalalinia SH, et al. (2016) Association of dietary behaviors with physical activity in a nationally representative sample of children and adolescents: The CASPIAN- IV Study. Int J Pediatr 4: 1505-1517.
- Saeidi Z, Vakili R, Ghazizadeh Hashemi A, Saeidi M (2015) The effect of diet on learning of junior high school students in Mashhad, North-east of Iran. Int J Pediatr 3: 517-526.
- Vakili R, Moghadam EZ, Khademi GH, Vakili S, Saeidi M (2015) Child mortality at different world regions: A comparison review. Int J Pediatr 3: 809-816.
- Khan ZA, Al-Jama AA, Madan I (1989) Parasitic infections among food handlers in Dammam and Al-Khobar, Saudi Arabia. Ann Saudi Med 7: 47-50.
- Petri WA, Haque R, Lyerly D, Vines R (2000) Estimating the impact of amebiasis on health. Parasitol Today 16: 320–321.
- Herwaldt B (2000) Cyclospora cayetanensis: Review, focusing on the outbreaks of cyclosporiasis in the 1990s. Clin Infect Dis 31: 1040–1057.
- Okhuysen P, White A (1999) Parasitic infections of the intestine. Curr Opin Infect Dis 12: 467–472.
- Reed SL (2001) Amebiasis and infection with free-living amebas. In: Harrison's Principles of internal medicine. 15th (edn), McGraw-Hill, New York, USA.
- Stanley S (2001) Pathophysiology of amoebiasis. Trends Parasitol 17: 280–285.
- Nokes C, Bundy D (1992) Does helminth infection affect mental processing and educational achievement. Parasitol Today 10: 14-18.
- Ortega Y (2006) Food borne parasites. Springer Science Business Media, USA.
- Areeshi M, Beeching N, Hart C (2007) Cryptosporidiosis in Saudi Arabia and neighboring countries. Ann Saudi Med 27: 325-332.
- Ortega T, Vergara A, Joaquín G, Antonio C, Patricia G, et al. (2006) Cryptosporidium hominis diarrhea outbreak and transmission linked to diaper infant use. Medicina Clínica 127: 653–656.
- Khan A, Gul A, Hammad M, Bibi Y, Bibi A, et al. (2015) Prevalence of Giardia intestinalis and hymenolepis nana in Afghan refugee population of Mianwali district, Pakistan. Afr Health Sci 15: 394–400.
- Sehgal R, Reddy G, Verweij J, Rao A (2010) Prevalence of intestinal parasitic infections among school children and pregnant women in a low socio-economic area, Chandigarh, North India. RIF 1: 100-103.
- Duda A, Bogacka D, Arendarczyk N, Kołodziejczyk L, Lanocha A (2015) The prevalence of blastocystis hominis and other protozoan parasites in soldiers returning from peacekeeping missions. Am J Trop Med Hyg 92: 805–806.

