Keywords
Infection control; Knowledge, Nurses; PPE
Introduction
Health care professionals and patients are at high risk to be exposed to potentially infected blood and body fluids that can lead to serious or even lethal infections [1]. Nurses in particular are repeatedly exposed to various infections during the course of carrying out their nursing activities [2]. This can be minimized by applying standard precautions as hand hygiene, use of personal protective equipment (e.g., gloves, gowns, masks), safe injection practices, safe handling of potentially contaminated equipment or surfaces in the patient environment, and respiratory hygiene/ cough etiquette which are designed to reduce the risk of acquiring occupational infection from both known and unexpected sources in the healthcare setting [3]. At 1996 the Center for Disease Control and Prevention (CDC), put forward guidelines, a revised version of a preventive concept against nosocomial infections. It advocates basic standard precautions for all healthcare delivery and additional specific measures to protect healthcare workers and patients from exposure to potentially harmful microorganisms [4-6].
Despite the adoption of these guidelines by healthcare worker in several countries, compliance with aseptic precautions is know n to be “poor and lacking” [7-10]. Numerous studies shown that factors that contribute to non-compliance with standard precautions include lack of understanding and knowledge among health care workers on how to properly use protective barriers, lack of time, lack of resources, and lack of proper training. Other reported that better knowledge of universal precautions among health care workers was one of the predictors of better compliance [11-20].
Nurses at King Fahad Hospital-Al-Baha (KFH – Baha) are responsible for directing and coordinating nursing care in all departments in line with the nursing clinical application standards. This cover observing and reporting patient condition, providing nursing care, recording pulse and temperature, administering drugs and other medicines and providing support to patients and relatives.
In King Saudi Arabia (KSA), as in several other countries, each hospital has a multidisciplinary Infection Control Committee, which provides advice on the issues of control of infection, defines standards, and recommends policies. Several studies have evaluated disinfection and sterilization procedures in hospitals, knowledge and practices of hospital staff, and compliance with universal precautions, but similar data are few if not available in KSA. Information on this topic is necessary to assess whether nurses are prepared to assume their responsibilities in preventing hospital infections. Studies on standard precautions are increasing over the world [3,6,7,10], studies from Saudi Arabia that assessed nurse knowledge and compliance towards SPs are scarce. Hence this study was conducted, with the objective to determine with usage of Personal Protective Equipment (PPE) among nurses working at Al-Baha King Fahad Hospital, KSA.
Methodology
This was a cross sectional descriptive study aimed at determining the knowledge, practice and factors that influence compliance with usage of Personal Protective Equipment (PPE) among nurses working at Al-Baha King Fahad Hospital, KSA.
Study population
The study population were nurses working in medical, surgical, maternity and pediatric wards, who had worked for a minimum period of six months. The study targeted nurses since they are amongst the healthcare providers who are in majority and are involved in a number of nursing activities which render them at risk of acquiring and transmitting HAIs. These activities include, wound management, initiation of intravenous infusions, administration of injections, management of labour, waste disposal and instrument processing. The medical wards admit patients with various disease conditions some of which are infectious. Patients in surgical wards are at increased risk of acquiring hospital acquired infections because of the nature of surgical interventions they go through most of which are invasive. Midwifes in maternity wards are at increased risk of acquiring hospital acquired infections because the nursing and midwifery activities involve blood and body secretions as well as being invasive in nature. Some of these activities include, vaginal examination, handling of second and third stage of labour, suturing of episiotomies, and removal of retained placenta. Paediatric ward admits patients with both medical and surgical conditions.
Sampling procedure
Purposive sampling was used for selecting the wards and in each selected ward a list of names for the nurses was obtained from the team leader. Simple random sampling was then applied to obtain eligible participants. All the eligible participants were selected and those who consented to participate were recruited into the study.
Data collection
Data was collected using self- administered semi structured questionnaire that composed of information about demographic and occupational characteristics of the respondents like: (gender, age, education and years of experience), as well as their knowledge and practices regarding compliance with usage of Personal Protective Equipment (PPE). The questionnaire was developed grounded on the associated literatures and statistical experts in our college assess its validity and reliability. The subjects were asked to rate their believe, awareness and practices about PPE using rating as "Excellent", "Good" or "Ok". Knowledge questions using rating as " Disagree, "Ok", "Agree" and "Strongly agree". These questionnaires were checked for completeness and consistency upon collection.
Data analysis
Statistical Package on Social Science (SPSS) version 16 was used to analyze the data. Descriptive statistics were used to analyse characteristics of participants. Chi-square and correlation was used to establish significance and relationship between variables.
Presentation of Results
The results have been presented in form of frequency tables and bar graphs and a narrative explanation accompanying each form of presentation.
Findings
A total of 185 nurses consented and the response rate, adjusted for non-delivery of questionnaires, was 92.5%.
Table 1 represents demographic characteristics of the studied sample, among the respondents, 145 (78.4%) were female and 40 (21.6%) were male; most of the studied nurses were young in the age group of less than 40 years, had bachelor’s degree and work as staff nurses for more than 3 years in percentages of (81.1%, 74.6% & 61.6%) respectively.
| Character |
Components |
Frequency |
Percent |
| Gender |
Male |
40 |
21.6 |
| Female |
145 |
78.4 |
| Age |
20 - 30 year |
66 |
35.7 |
| 31-40 years |
84 |
45.4 |
| Over 40 years |
35 |
18.9 |
| Education |
Diploma or less |
47 |
25.4 |
| Bachelor and post |
138 |
74.6 |
| Work experience |
Less than 3 years |
71 |
38.4 |
| More than 3 years |
114 |
61.6 |
Table 1 Demographic characteristics.
Personal protective equipment (PPE)
The primary use of personal protective equipment (PPE) is to protect healthcare workers (HCWs) and reduce opportunities for transmission of microorganisms in healthcare facilities. It does not reduce the level of hazard itself nor guarantee total protection. They should be used as the supplement to the administration and engineering control in the care of the infective patients.
The overall awareness amongst the entire questionnaire respondents was 172 (93%) as shown in Table 2 below.
| |
Frequency |
Percent |
| Excellent |
141 |
76.2 |
| Good |
31 |
16.8 |
| Ok |
13 |
7.0 |
| Total |
185 |
100.0 |
Table 2 Overall awareness to PPE.
Regarding the correlation of PPE with the demographic characteristics of respondent nurses as shown in Table 3 there is strong evidence of positive relationship [p – value of (0.024, 0.043, 0.001, 0.030)] between awareness of the respondents with PPE as an effective barrier for infection control and their gender, age, education and work experience respectively.
| PPE |
| Character |
Excellent
141 (76.2%) |
Good
31(16.8%) |
Ok
13 (7%) |
P value |
| Gender |
Male |
24 (17.0 %) |
11 (35.5%) |
5 (38.5%) |
0.024 |
| Female |
117 (83.0%) |
20 (64.5%) |
8 (61.5%) |
| Age |
20 - 30 year |
55(39.0%) |
6 (19.4%) |
5 (38.5%) |
0.043 |
| 31-40 years |
57 (40.4%) |
22 (71.0%) |
5 (38.5%) |
| Over 40 years |
29 (20.6%) |
3 (9.7%) |
3 (23.1%) |
| Education |
Diploma or less |
28 (19.9%) |
15 (48.4%) |
4 (30.8.0%) |
0.001 |
| Bachelor and post |
113 (80.1%) |
16 (51.6%) |
9 (69.2%) |
| Work experience |
Less than 3 year |
51 (36.2%) |
14 (45.2%) |
6 (46.2%) |
0.030 |
| More than 3 years |
90 (63.8%) |
17 (54.8%) |
7 (53.8%) |
Table 3 Statistical Relation between the respondent Awareness of using PPE and their Demographic Characteristics.
Hand mediated transmission
Hands are the most common vehicle of transmission of organisms. And 91.6 per cent of the nurse staff agreed that hand mediated transmission is one of the major sources of cross infection. As shown in Figure 1 the majority (85.4%) of the studied sample were agreed that hands mediated transmission (spread) of infection is a main contributory factor to the infection risks for hospital in-patients.
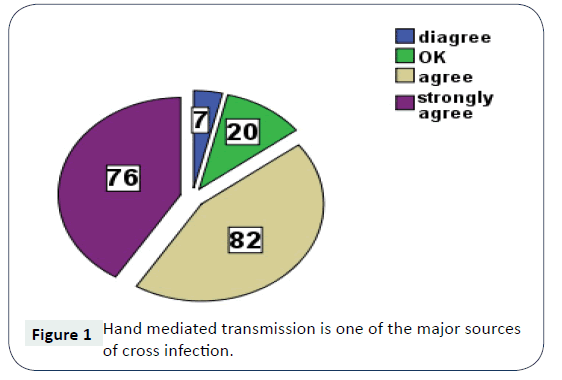
Figure 1: Hand mediated transmission is one of the major sources of cross infection.
Table 4 shows that there was an evidence of significant difference between hand mediated transmission of infection and demographic characters of respondent nurse groups regarding age, sex, education and work experience years being more in females, ages less than 40 years, bachelor and post-graduation and more than 3 years experiences, (P value <0.005).
| Character |
Disagree
27 (14.6%) |
Agree
158 (85.4%) |
P value |
| Gender |
Male |
15 (55.6 %) |
25 (15.8%) |
0.000 |
| Female |
12 (44.4%) |
133 (84.2%) |
| Age |
20 - 30 year |
3(11.1%) |
63 (39.9%) |
0.001 |
| 31-40 years |
15 (55.6%) |
69 (43.7%) |
| Over 40 years |
9 (33.3%) |
26 (16.3%) |
| Education |
Diploma or less |
11 (40.7%) |
36 (22.8%) |
0.000 |
| Bachelor and post |
16 (59.3%) |
122 (77.4%) |
| Work experience |
Less than 3 year |
9 (33.3%) |
62 (39.2%) |
0.000 |
| More than 3 years |
18(66.7%) |
96 (60.8%) |
Table 4 Statistical Relation between the respondent Knowledge of Hand Mediated Transmission and their Demographic Characteristics.
Wearing gloves
Routine use of disposable gloves has been recommended for all patient contacts. Gloves ideally should be removed after seeing a patient and the hands washed thoroughly before re-gloving to see a new patient. Out of the total staff, 86 per cent claimed to wear fresh gloves before patient examination and procedures but only 57 per cent of the staff actually did it during observations (Figure 2). Out of 185 nurses staff 126 (68.1%) claimed that they always wore gloves before patient examination (Table 5).
| Character |
Sometimes
28 (15.1%) |
Frequently
31 (16.8%) |
Always
126 (68.1%) |
P value |
| Gender |
Male |
13 (46.4%) |
9 (29%) |
18 (14.3%) |
0.001 |
| Female |
15 (53.6%) |
22 (71%) |
108 (85.7%) |
| Age |
20 - 30 year |
6(21.4%) |
11 (35.5%) |
49(38.5%) |
0.190 |
| 31-40 years |
17 (60.7%) |
11 (35.5%) |
56 (38.5%) |
| Over 40 years |
5 (17.9%) |
9 (29.0%) |
21 (23.1%) |
| Education |
Diploma or less |
4 (14.3%) |
1 (3.2%) |
42 (33.3%) |
0.013 |
| Bachelor and post |
24 (85.7%) |
30 (96.8%) |
84 (66.7%) |
| Work experience |
Less than 3 year |
8 (28.6%) |
9 (29.0%) |
54 (42.9%) |
0.030 |
| More than 3 years |
20 (71.4%) |
22 (71.0%) |
72 (57.1%) |
Table 5 Association of demographic characteristics and wearing gloves.
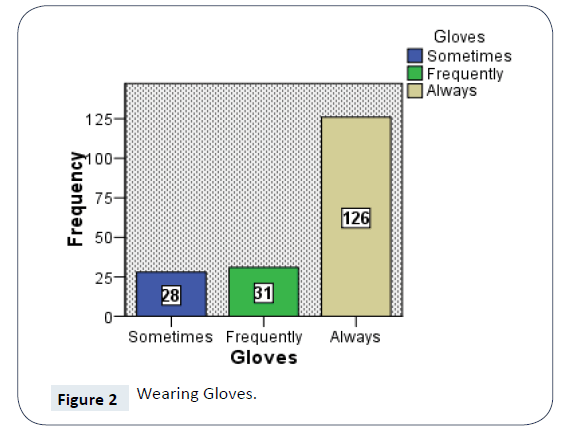
Figure 2: Wearing Gloves.
Discussion
To our knowledge, this is the first research study contracted in Al- Baha king Fahad hospital among any group of health care workers, investigating the issue of compliance with Standard Precautions to avoid occupational exposure to pathogens. Present study was carried out to assess the knowledge, practice and attitude of nursing staff related to infection control measures [21-24].
Infection control is a key factor of practice for all healthcare professionals, not only for their health but also to reduce nosocomial infections and thus improve the patient safety [25]. Standard precautions are a set of basic infection prevention practices intended to prevent transmission of infectious diseases from one person to another. Because it is not always known if a person has an infectious disease or not, standard precautions should be applied to every person every time to ensure that transmission of diseases do not occur [3].
By means of their knowledge and practice to protect themselves and patients from exposure to potentially infection, nurses show an important part in infection management [26,27]. Our study discovered that, among 185 nurses consented and participated in this study, 21.6% were males and 78.4% were females. Nursing is a female dominated profession hence most of the participants were females. Female nurses had a higher perception of being at risk by virtue of working in a hospital than their male counterparts and this difference was statistically significant p=0.002. In our study most of the studied nurses were young in the age group of less than 40 years, had bachelor’s degree and work as staff nurses for more than 3 years in percentages of (81.1%, 74.6% & 61.6% ) respectively, in comparison with some other studies in the area in which three quadrants of the studied nurses had diploma degree and nearly half of them attended training programs in infection control. Moreover, their years of experience was more than 15 years at workplace [28]. These results come in agreement with similar studies that revealed dominance of females, majority of nurses in their study had bachelor's degree and most of nurses attended infection control programs [29-31].
Regarding PPE, the mandatory use of PPE defined by health authorities in Saudi, our study showed the overall awareness amongst study respondents was 93%, this was not in accordance with may studies in Egypt [32,33]. Routine use of disposable gloves has been recommended for all patient contacts. Gloves require hand hygiene before wearing and be removed after seeing a patient and the hands washed thoroughly before re-gloving to see a new patient. In our study nurses showed satisfactory knowledge 86% on this regard, this finding was in concordance with a study reported that compliance with hand hygiene performance is high [34] but was not in concordance with three studies who reported that compliance with hand hygiene performance is low [35-38].
Conclusion
Our study concluded that nurses had excellent knowledge with and appropriate use of PPE as vital in safeguarding the HCWs and spread of infection. However, practice was unsatisfactory about infection control standard precautions.
Recommendation
Continuous monitoring of nurses' practice parallel with providing adequate resources, decrease of work load by increasing the number of nursing staff and emphasizing training courses is crucial issues that improve the compliance with infection control standard precautions.
References
- Twitchell KT (2003) Bloodborne pathogens. What you need to know–Part II. AAOHN J 51: 89-97.
- Kosgeroglu N, Ayranci U, Vardareli E, Dincer S (2004) Occupational exposure to hepatitis infection among Turkish nurses: frequency of needle exposure, sharps injuries and vaccination. Epidemiol Infect 132: 27-33.
- Siegel JD, Rhinehart E, Jackson M, Chiarelho L, The Healthcare Infection Control Practices Advisory Committee (2007) Guideline for isolation precautions: preventing transmission of infectious agents in healthcare settings. Am J Infect Control 35: S64?S164.
- Widmer AF, Sax H, Pittet D (1999) Infection control and hospital epidemiology outside the United States. Infect Control Hosp Epidemiol 20: 17-21.
- Centers for Disease Control (1988) Update: Universal precautions for prevention of transmission of human immunodeficiency virus, hepatitis B virus, and other bloodborne pathogens in health-care settings. MMWR Morb Mortal Wkly Rep 37: 377-388.
- Garner JS (1996) Guideline for isolation precautions in hospitals. The Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol 17: 53-80.
- Jawaid M, Iqbal M, Shahbaz S (2009) Compliance with standard precautions: a long way ahead. Iran J Public Health 38: 85-88.
- Powers D, Armellino D, Dolansky M, Fitzpatrick J (2016) Factors influencing nurse compliance with standard precautions. Am J Infect Control 44: 4?7.
- Gammon J, Morgen H (2007) A review of the evidence for suboptimal compliance of health care practitioners to infection control precautions. J Clin Nurs 17: 157-167.
- Talan DA, Baraff LJ (1990) Effect of education on the use of universal precautions in a university hospital emergency department. Ann Emerg Med 19: 1322-1326.
- Baraff LJ, Talan DA (1989) Compliance with universal precautions in a university hospital emergency department. Ann Emerg Med 18: 654-657.
- Gershon RRM, Vlahov D, Felknor SA, Vesley D, Johnson PC, et al. (1995) Compliance with universal precautions among health care workers at three regional hospitals. Am J Infect Control 23: 225-236.
- Taneja J (2009) Evaluation of knowledge and practice amongst nursing staff toward infection control measures in tertiary care hospital in India. Can J Infect Control 24: 104-107.
- Vij A, Williamson SN, Gupta S (2001) Knowledge and practice of staff towards infection control measures in a tertiary care hospital. J Acad Hosp Adm 13: 31-35.
- Chan MF, Ho A, Day MC (2008) Investigating the knowledge, attitudes and practice patterns of operating room staff towards standard and 96 Labrague LJ, Rosales RA, Tizon MM transmission-based precautions: results of a cluster analysis. J Clin Nurs 17: 1051-1062.
- Vaz K, McGrowder D, Alexander-Lindo R, Gordon L, Brown P, et al. (2010) Knowledge, awareness and compliance with universal precautions among health care workers at the University Hospital of the West Indies, Jamaica. Int J Occup Environ Med 1: 171-181.
- Tait AR, Voepel-Lewis T, Tuttle DB, Malviya S (2000) Compliance with standard guidelines for the occupational transmission of bloodborne and airborne pathogens: A survey of post anesthesia nursing practice. J Contin Educ Nurs 31: 38-44.
- Sax H, Perneger T, Hugonnet S, Herrault P, Chraiti MN, et al. (2005) Knowledge of standard and isolation precautions in a large teaching hospital. Infect Control Hosp Epidemiol 26: 298-304.
- Chan R, Molassiotis A, Chan E, Chan V, Ho B, et al. (2002) Nurse knowledge of and compliance with universal precaution in an acute care hospital. Int J Nurs Stud 39: 157-163.
- Ofili AN, Asuzu MC, Okojie OH (2003) Knowledge and practice of universal precaution amongst nurses in Central Hospital, Benin City, Edo State, Nigera. Niger Postgrad Med J 10: 26-31.
- Oliveira AC, Marziale MH, Paiva MH, Lopes AC (2009) Knowledge and attitude regarding standard precautions in a Brazilian public emergency service: a cross sectional study. Rev Esc Enferm USP 43: 313-319.
- Tavolacci MP, Ladner J, Bailly L, Merle V, Pitrou I, et al. (2008) Prevention of nosocomial infection and standard precautions: knowledge and source of information among healthcare students. Infect Control Hosp Epidemiol 29: 642-647.
- Luo Y, He GP, Zhou JW, Luo Y (2010) Factors impacting compliance with standard precaution in nursing, China. Int J Infect Dis 14: e1106-e1114.
- Kim KM, Kim MA, Chung YS, Kim NC (2001) Knowledge and performance of the universal precautions by nursing and medical students in Korea. Am J Infect Control 29: 295-300.
- Christenson M, Hitt J, Abott G, Septimus E, Iverson N (2006) Improving patient safety; resource availability and application for reducing the incidence of health care associated infection. Infect Control Hosp Epidemiol 27: 245-251.
- World Health Organization (2011) Report on the burden of endemic health care - associated Infection Worldwide : clean care is healthy care, Geneva: WHO.
- Amadu MO, Saka MJ (2012) Knowledge, awareness and compliance with standard precautions. J Community Med Health Educ 2: 131.
- El- Greeb HE, Ahmed AI, Atia HM, Abdel- Mouty SM (2018) Assessment of nurses' compliance with infection control standard precautions at outpatient clinics of Urology and Nephrology Center - Mansur University. IOSR J Nurs Health Sci 7: 54-59.
- Labrague LJ, Rosales RA, Tizon MM (2012) Knowledge of and compliance with standards precautions among student nurses. Int J Adv Nurs Stud 1: 84-97.
- Hamid MZA, Aziz NA, Anita AR, Norlijah O (2010) Knowledge of blood-borne infectious diseases and the practice of universal precautions amongst health-care workers in a tertiary hospital in Malaysia. Southeast Asian J Trop Med Public Health 41: 1192-1199.
- Fayed NM, Elbahnasawy HT, Omar TK (2016) Effect of instructional program on nurses compliance with universal precautions of infection control. Int. J Novel Res Healthc Nurs 3: 81-92.
- Ahmed ER, Khamis M (2013) Effect of a developed educational booklet about standards infection control precautions on nurses´ knowledge and performance at Woman’s Health Center - Assiut university, Egypt. Med J Cairo Univ 80: 435-445.
- Hakim SA, Abouelezz NF, El Okda EM (2016) Use of personal protective devices among health care workers in a teaching hospital in Cairo, Egypt. Egypt J Occup Med 40: 287-300.
- Asare A, Enweronu-Laryea CC, Newman MJ (2009) Hand hygiene practices in a neonatal intensive care unit in Ghana. J Infect Dev Ctries 3: 352-356.
- Kim PW, Roghmann MC, Perencevich EN, Harris AD (2005) Rates of hand disinfection associated with glove use, patient isolation and changes between exposure to various body sites. Am J Infect Control 31: 97-103.
- Akyol AD (2007) Hand hygiene among nurses in Turkey: opinions and practices. J Clin Nurs 4: 431-437.
- Kalata NL, KamangeL, Muula AS (2013) Adherence to hand hygiene protocol by clinicians and medical students at Queen Elizabeth Central Hospital, Blantyre-Malawi. Malawi Med J 25: 50-52.
- Wagner PDJ, Parker CE, Mavis B, Smith MK (2011) An interdisciplinary infection control education intervention: necessary but not sufficient. J Grad Med Educ 3: 203-210.

