Keywords
Peripheral venous gases (pv); Partial pressure of Oxygen PpvO2; Oxygen saturation SpvO2
Arterio-venous oxygen difference, predictably, results from the characteristics of oxygen dynamics and kinetics during its transfer from arterial to venous sides of tissues through capillaries. As dissolved oxygen is taken up by tissue cells, partial pressure of oxygen drops, which allows oxygen molecules to depart from haemoglobin binding sites, according to the principle of cooperativity and characteristics of oxygen dissociation curve [1]. A new equilibrium is achieved with different oxygen saturation and less oxygen content and tension. Central venous (cv) oxygen saturation becomes, predictably, narrowly around 75%, depending on different regional metabolic rate and tissue oxygen uptake. PcvO2 is 5.2, 6.4, 9.1, and 48 kPa when breathing air, oxygen, O2 at 2 atmospheric pressure, and O2 at 3 atmospheric pressure respectively [2].
On the other side, peripheral venous (pv) gases had been proven to correlate with arterial values short of PpvO2 or SpvO2 [3]. Presently, either PaO2 or SpO2 are the preferred monitors in clinical conditions including anaesthesia and PpvO2 & SpvO2 lack any similar value. SpO2 detects O2 lack, which is vital, however fails to monitor O2 excess, which is toxic. We report an interesting finding of highly correlating PpvO2 and SpvO2 under anaesthesia and during early recovery (Table 1).
A 21 years girl, with Peutz-Jegher’s Syndrome (PJS) [4], had undergone Laparotomy, multiple polyps excision, and limited resection. GA was conducted by administering, fentanyl 100 μgms, morphine 10 mg, propofol 150 mg, atracurium 30 mg, and then mechanical ventilation, with ET tube on air, oxygen of FiO2 (0.51) and sevoflurane for 2 MAC. A chance venous sample to check haemoglobin level had SpvO2 96.5%, and PpvO2 30.87 kPa on FiO2 0.51 as shown in associated table. In recovery room, PpvO2 was 11.92 kPa on face mask O2, with assumed FiO2 (0.35). Reexamining her heart and both ECG and transthoracic cardiac Echocardiography proved normal. In the second day, PpvO2 was 5.55 kPa on room air with SpvO2 78.7%. Arterial samples were not taken intraoperatively nor the following days, however assumed PaO2 values of 40 and 12 kPa respectively, were used in calculating regional O2 uptake as shown in Table 2.
A thorough search was conducted of the MEDLINE database on NHS Evidence for the following topic: peripheral venous oxygen saturation PpvO2 and PpvO2 under anaesthesia. Human and English Language articles were the limitations used.
Vasodilatation is a recognized cause for arterialization of peripheral veins. This was exploited by heated-hand technique [5] and warming the hand up while applying transcutaneous carbon dioxide monitor.
Anaesthesia induced vasodilatation and partly metabolic depression could explain our case high SpvO2 99.5% with very high positive correlation to SpO2, (Figure 1). Vasodilatation [6] could be potentiated in peripheries where continuous capillary network with throughfare channels prevail, leading to arterio venous shunt. O2 uptake to O2 content ratios during anaesthesia and 24 hours later, were 0.59% and 24.3% respectively, in marked contradistinction to the usual 15% metabolic depression under anaesthesia.
| Time VBGs |
Under anaesthesia |
Recovery room |
24h |
| Site |
Dorsum R hand |
L Forearm |
Dorsum L hand |
| FiO2 |
0.51 |
0.35 |
0.21 |
| SpO2% |
100 |
99 |
99 |
| Temp |
36.2 |
36.2 |
37 |
| O2 SAT% |
99.5 |
96.5 |
78.7 |
| O2CT ml/dl |
12.2 |
13 |
9.30 |
| pH |
7.355 |
7.354 |
7.429 |
| pCo2 kPa |
5.7 |
5.55 |
5.16 |
| pCo2 kPa |
30.87 |
11.92 |
5.55 |
| BE mmol/l |
-2.1 |
-2.7 |
0.7 |
| tHB gm/l |
83 |
95 |
85 |
| FO2 HB% |
98 |
95.1 |
74.4 |
| FCO HB% |
1.3 |
0.7 |
1.4 |
| F Met HB% |
0.3 |
0.3 |
0.6 |
| F H HB% |
0.4 |
3.9 |
23.9 |
Table 1: Time VBGs.
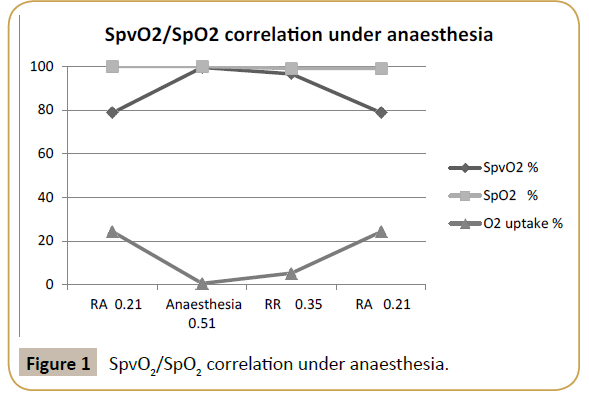
Figure 1:SpvO2/SpO2 correlation under anaesthesia
SpO2, the standard continuous non-invasive oxygen saturation monitor, reflects the 98 percent of arterial oxygen content that is normally carried by haemoglobin, while the PO2, invasively, measures dissolved O2 in plasma. There is lack of literature evidence of favourable correlation between SpvO2 and SpO2 or established clinical place for using PpvO2 or SpvO2 as ventilation monitors under anaesthesia [7].
Arterio-venous malformation is not a recognized association of PJS. Besides, cardiovascular status didn’t show any abnormality on re-examination of our case and PpvO2 normalized 24 hours later to become 5.55 kPa.
Venous PO2, and therefore minimum tissue PO2, increases at three atmospheric pressures only. This is because O2 tissue requirement is then met by dissolved O2 and saturation of venous blood remains close to 100% [1]. Unfortunately no arterial sample was taken, however in our young and healthy patient with FiO2 0.51, it could be assumed to be around 40 kPa. Then, with PpvO2 of 30.87 kPa, venous oxygen uptake would come to 0.212 ml/dl. This was taken from soluble O2, hence oxygen saturation was 99.5%, hence tissue would be drenched in oxygen. Then, according to PpvO2, oxygen uptake was satisfied by dissolved form, which could be calculated to 0.212 ml/dl blood.
Hence, It would be difficult to assume that raising FiO2 could cause such rise in venous oxygenation. However, if this were the case, then the question of oxygen toxicity as related to such abruptly high PpvO2, and hence tissue PO2, should be addressed. Also, exposing venous endothelium to excess oxygen could play a factor in developing deep venous thrombosis, should deep veins have the same high SpvO2. Finally, during O2 therapy, monitoring SpvO2 or PpvO2 could prove a reasonable option in order to avoid unnecessary excess oxygen with its potential toxicity.
It seems theoretically plausible that higher oxygenation of peripheral veins could be secondary to anaesthesia induced regional vasodilatation or metabolic depression or both. However this is not included in the recognized effects of general anaesthesia as stated in Nunn’s Applied Respiratory Physiology [1], seventh edition.
Vasodilatation of continuous capillary network, as in the case of hands’ and feet’s muscles, could lead to immense “steal” phenomenon with shutting down the whole capillary network in favor of central arteriolar-venular capillary vascular shunt leading to continuation of arteriolar blood flow, kinetically uninterrupted, to the venular side and causing peripheral PvO2 to attain higher values. If this were the case, vasodilators and regional anaesthesia could possibly lead to such phenomenon as well [6, 8].
On the other side, it is difficult to assume that anaesthesia could, paradoxically, cause metaarteriolar vasospasm, allowing arterial flow directly through the capillary central arteriolar-venular vascular shunt leading to higher oxygenation of peripheral venous blood.
Unfortunately, we didn’t have arterial values to check on arteriovenous difference and tissue oxygen uptake in relation to variable FiO2.
Regional metabolic depression, lack of peripheral tissue oxygen consumption and maintaining soluble oxygen level could possibly be another explanation. However absolute metabolic shut down is not usually associated with anaesthetics, and anyway neither lactate level, glucose, Anion gap were affected, nor body temperature was unduly dropped. However, It would be interesting to measure simultaneously peripheral veins, femoral, jugular, or mixed venous gases in order to look into differential metabolic depression.
Etiologically, functional magnetic resonance imaging (fMRI) could offer a valuable hint by detecting changes in blood flow through using the blood oxygen-level-dependent (BOLD) contrast [9]. Near infrared spectroscopy (NIRS) [10] alone or combined with fMRI [11], could display spectral absorption of the hand tissue and make some conclusions about its average tissue oxygenation saturation (StO2), hence metabolic activity level.
| Gases / FiO2 |
pv anaesthesia 0.51 |
a anaesthesia 0.51 |
pv RR 0.35 |
a RR 0.35 |
pv 24h 0.21 |
a 24h 0.21 |
| PO2 kPa |
30.87 |
32.1* |
11.92 |
22* |
5.55 |
13* |
| O2 sat % |
99.5 |
99.5 |
96.5 |
99.5 |
78.7 |
99.5 |
| tHB gm/dl |
8.3 |
8.3 |
9.5 |
9.5 |
8.5 |
8.5 |
| H HB gm/dl |
0.033 |
0 |
0.37 |
0 |
2.03 |
0 |
| O2 uptake from HB ml/dl |
0.045 |
- |
0.5 |
- |
2.82 |
- |
| Dissolved O2ml/dl |
0.716 |
0.774 |
0.276 |
0.510 |
0.128 |
0.301 |
| Dissolved O2uptake ml/dl |
0.028 |
|
0.234 |
|
0.173 |
|
| O2 CT ml/dl |
12.2 |
12.273 |
13 |
13.734 |
9.3 |
12.3 |
| O2 uptakeml/dl & % |
0.073 0.594% |
|
0.734 5.34% |
|
3 24.3% |
|
*PaO2 kPa= FiO2 x 63; Dissolved O2 ml/dl = PO2 x 0.0232 (very small to be affected by approximation) O2aCT ml/dl = dissolved O2+tHBx1.35, RR: Recovery room.
Table 2: PaO2 values of 40 and 12 kPa respectively, were used in calculating regional O2 uptake.
Should this phenomenon of higher PpvO2, prove consistent, venous sampling could, then, suffice instead of the potentially complicated arterial one and continuous venous oxymetry could be an option. Also if it were technically possible to check non-pulse oxymetry directly or through frequent venostasis, then noninvasive comparison between pulse and non-pulse oxymetry would be feasible, with its potential repercussions on level of oxygenation, adequacy of anaesthesia, and possibly intraoperative awareness.
Finally, we wish to raise the attention to our unexpected and unexplained observation of high PpvO2 under anaesthesia, that warrants serious appraisal that is necessary to define its actual weight and territorial distribution, as well as its life span. This would necessitate monitoring quite large number of patients and different accessible veins under different anaesthetics, including TIVA and regional anaesthetics, as well as various vasoactive agents.
References
- Andrew BL (2010) Nunn's Applied Respiratory Physiology. Churchill Livingstone, UK.
- Andrew BL (2010) Nunn's Applied Respiratory Physiology, Seventh Edition. Churchill Livingstone, UK.
- Treger R, Pirouz S, Kamangar N, Corry D (2010) Agreement between central venous and arterial blood gas measurements in the intensive care unit. Clin J Am SocNephrol 5: 390-394.
- Goldman L, Ausiello D (2007)Cecil Textbook of Medicine. Pa: Saunders Elsevier, Philadelphia.
- MA Nauck, H Lie, EG Siegel,PD Niedmann,Creutzfeldt W (1992) Critical evaluation of the ‘heated-hand-technique’ for obtaining ‘arterialized’ venous blood: incomplete arterialization and alterations in glucagon response. Clinical Physiology 12: 537-552.
- Wendell ES, William EC, William KH (1968) Circulatory studies during spinal anaesthesia: Central and Peripheral Venous Oxygen Saturation Before and After Administration of Vasopressors. Anesthesia and Analgesia, Current Researches 47: 725-732.
- Masip J, De Mendoza D, Planas K, Paez J, Sanchez B, et al. (2012) Peripheral venous blood gases and pulse-oximetry in acute cardiogenic pulmonary oedema.European Heart Journal: Acute Cardiovascular Care 1: 275-280.
- Cerilli GJ, Engell HC (1966)The Effect of Spinal Anesthesia on Femoral Vein Oxygen Tension. Surgery 60:668-670.
- Maton A, Jean H, Charles WM, Susan J, Maryanna QW, et al. (1993) Human Biology and Health. Englewood Cliffs, New Jersey.
- Echiadis AS, Crabtree VP, Bence J, Hadjinikolaou L, Alexiou C, et al. (2007) Non-invasive measurement of peripheral venous oxygen saturation using a new venous oximetry method: evaluation during bypass in heart surgery. Physiol Meas 28:897-911.
- van Erning MC, Thijssen LJ, Oeseburg HO, HoefnagelsB, et al. (2002) Simultaneous near-infrared spectroscopy and functional magnetic resonance imaging in healthy young and elderly subjects. Hum Brain Mapp16:14-23.

