Caleb R Walker1, Haroon N. Khan2, Eric W. Schneider1 and David A. Reichstein1*
1Tennessee Retina, PC. Nashville, TN, USA
2Concord Infectious Disease Associates, PC, Lebanon, TN, USA
*Corresponding Author:
David Reichstein
Tennessee Retina, 345 23rd Ave N
Ste 250, Nashville, TN 37203, USA
E-mail: dreichstein@tnretina.com
Received date: October 11, 2017; Accepted date: October 28, 2017; Published date: October 31, 2017
Citation: Walker C R, Khan H N, Schneider E W, Reichstein D A (2017) Ocular Tuberculoma in the Absence of Miliary. J Eye Cataract Surg Vol.3:40. doi: 10.21767/2471-8300.100040
Copyright: © 2017 Walker CR, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Keywords
Granuloma; Tuberculosis; Lesion
Introduction
While tuberculosis is a common disease worldwide, the incidence of tuberculomas in the eye is rare in developed nations. In 2015, there were approximately 10,000 cases of tuberculosis (TB) in the United States. Of the global population infected by Mycobacterium tuberculosis, 75% of those are latent infections [1]. Tuberculosis primarily affects the lungs although extra-pulmonary TB may affect the liver, bone, meninges, and eye. Although rare, primary TB has been documented in the eye. As such, ocular TB is manifested as panophthalmitis, keratitis, posterior uveitis, and endophthalmitis. When the lungs are involved, ocular involvement tends to primarily manifest as choroiditis [2].
Given it’s the varied nature of presentation, clinical diagnosis is challenging. While the most common symptom of ocular tuberculosis is uveitis, focal granulomatous disease is common as well. Posterior segment tuberculomas typically present with associated uveitis, even though tuberculosis is only diagnosed in 0.1% [3] of uveitis patients. Herein, we present the case of a tuberculoma presenting as a potential neoplasm in the absence of vitritis, anterior segment inflammation, or miliary TB.
Case Summary
A 45-year-old Filipino woman presented with blurred vision in her right eye two years after immigrating to the United States. Her best-corrected visual acuity was 20/50 in the right eye and 20/20 in the left. The patient’s medical history was otherwise unremarkable. The left fundus was unexceptional. The right eye demonstrated an amelanotic choroidal mass extending from the disc margin to the temporal aspect of the fovea. Optical Coherence Tomography (OCT) revealed a dome-shaped choroidal mass accompanied by subretinal fluid, with a juxtafoveal adhesion (Figure 1).
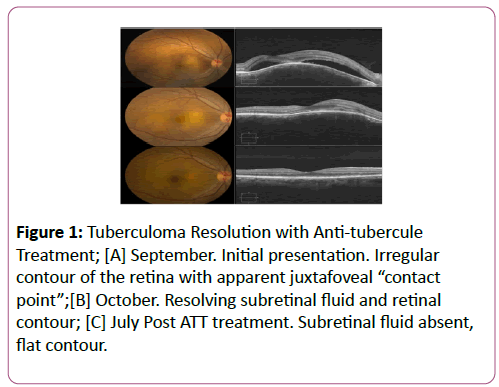
Figure 1: Tuberculoma Resolution with Anti-tubercule Treatment; [A] September. Initial presentation. Irregular contour of the retina with apparent juxtafoveal “contact point”;[B] October. Resolving subretinal fluid and retinal contour; [C] July Post ATT treatment. Subretinal fluid absent, flat contour.
A quantiferon gold test was recommended and was found to be positive, confirming the diagnosis of choroidal tuberculoma.
The patient initiated anti-tubercular therapy with a 2-month induction regimen of isoniazid (INH), rifampin (RIF), pyrizinamide (PZA), and ethambutol (EMB) followed by a 4-month consolidation regimen of isoniazid and rifampin. Pyridoxine, a vitamin B6 supplemented the anti-tubercular therapy. Four months later, BCVA in the right eye had improved to 20/40 with notable reduction in the size of the macular tuberucloma. OCT demonstrated decreased subretinal fluid. At final follow-up, BCVA in the right had improved to 20/20. No evidence of subretinal fluid was found on OCT. The patient completed ATT therapy and followed up as needed.
B-scan ultrasonography demonstrated an acoustically hollow mass measuring 5.8 × 4.4 × 1.4 mm (Figure 2). Fundus autofluorescence (FAF) found no abnormalities. Multifocal pinpoint leakages with prominent late pooling were seen on fluorescein angiography.
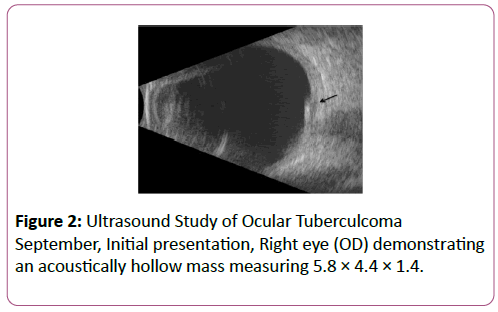
Figure 2: Ultrasound Study of Ocular Tuberculcoma September, Initial presentation, Right eye (OD) demonstrating an acoustically hollow mass measuring 5.8 × 4.4 × 1.4.
The patient was referred for a chest computerized tomography (CT) scan, mammogram, and evaluations due to concern for a choroidal metastasis. In September, a comprehensive uveitic evaluation was repeated and supplemented by infectious disease panels. Burgdorferi IgG and IgM, HIV antibodies type I and II, treponemal antibodies, and a syphilis screening profile were all negative. One month later, mammography demonstrated unilateral subtle focal microcalcifications, but no dominates mass. A chest, abdominal and pelvic CT with contrast revealed no evidence of acute abnormality, and there did not appear to be definitive signs of tuberculosis. At this point, the patient had a +20 mm PPD test.
Discussion
Active Tuberculosis is an uncommon disease in the United States, with an incidence of 3.0 per 100,000 persons in 2014 according to the CDC [4]. Rarely is ocular tuberculosis the presenting sign of a systemic tuberculosis infection isolated to the eye, and the lack of anterior segment inflammation or vitritis is still more rare.
Tuberculosis most commonly affects the choroid [5], presenting with uveitis or multi-focal choroiditis. Melanoma, metastatic disease, lymphoma and osteomas, need to be considered when tuberculomas are observed, especially in the absence of inflammation. This patient’s lesion had characteristics of both a metastasis and melanoma. Many of the granuloma characteristics matched that of an amelanotic melanoma: there was accompanying subretinal fluid (Figure 1), the lesion margin was adjacent to the optic nerve, the patient had symptoms of vision loss and the ultrasound was acoustically hollow (Figure 2). In contrast, choroidal metastases are typically yellow- or cream-colored, are acoustically solid and larger than 2.0 mm [6], and are often accompanied by subretinal fluid or intraretinal cysts. OCT patterns in ocular metastases show an irregular retinal pigment epithelium, with retinal thickening and gross undulation [7] while melanomas are accompanied by more shallow subretinal fluid and demonstrate a smooth curvature with shaggy photoreceptors [8].
While the cream-colored granuloma reported here was accompanied by fluid suggesting a metastasis, it had a smooth curvature on OCT and was acoustically hollow, which is more consistent with an amelanotic melanoma. Salman, et al. observed that many choroidal tuberculomas demonstrated a characteristic “contact point” on OCT, an adhesion between the retinal layers and retinal pigment epithelium, which may be attributable to the inflammatory adhesions overlying the neurosensory retina [9]. As other case reports [10], including the present one, have demonstrated, this observation by Salman, et al. may aid the clinician in the diagnosis of choroidal tuberculomas, and reflect the inflammatory process even among localized tuberculomas. Given that this patient’s lesion was subfoveal extending below the papillomacular bundle, a fine needle biopsy was felt to be unsafe. A negative chest x-ray and CT scan ruled out any systemic or primary infectious site, confirming the presence of TB isolated only within the eye.
WHO guidelines for tuberculosis infection were followed using INH, PZA, EMB, and RIF for 8 weeks, followed by INH and RIF for the following 18 weeks. Of note, ethambutol is well documented to produce dose-dependent optic neuritis, scotomas and edema, none of which were documented here. While our patient was prescribed EMB, some clinicians have chosen to replace EMB with a fluoroquinilone regimen to eliminate the risks accompanied by standard treatment. Pyridoxine, a vitamin B6 supplement, was prescribed as prophylaxis against peripheral neuropathy in using isoniazid. As seen on the OCT progression, the response was demonstrable in reducing the anatomical changes due to the tuberculoma.
Conclusion
Tubercular eye granulomas require a high degree of suspicion as they can mimic choroidal tumors. This case report demonstrates how careful anti-tubercular therapy can lead to excellent lesion regression once properly identified.
References
- Global tuberculosis control: key findings from the December 2009 WHO report. Wkly Epidemiol Rec 2010 Feb 26; 85(9):69-80.
- Mehta S (2006) The treatment of ocular tuberculosis: A survey of published literature. Indian J Ophthalmol 54: 278-280.
- Helm CJ, Holland GN (1993) Ocular Tuberculosis. Surv Ophthalmol 38(3):229-256.
- Copeland RA (1993) The classics: Tuberculosis, syphilis, and sarcoidosis. Jr. Ophthalmol Clin North Am 6:69-80.
- Salinas JL, Mindra G, Haddad M, Pratt R, Price SF et al. (2016) Leveling of Tuberculosis Incidence—United States, 2013-2015. MMWR Morb Mortal Wkly Rep 65: 273-278.
- Shields J, Shields C (2008) Intraocular Tumors: An Atlas and Textbook, 2nd edition. Philadelphia, PA. Lippincott Williams & Williams pp 189.
- Iuliano L, Scotti F, Gagliardi M, Bianchi I, Pierro L (2012) SD-OCT Patterns of the Different Stages of Choroidal Metastases. Ophthalmic Surg, Lasers and Imaging Retina 43: 30-34.
- Shields CL, Kaliki S, Rojanaporn D, Ferenczy SR, Shields JA (2012) Enhanced Depth Imaging Optical Coherence Tomography of Small Choroidal Melanoma Comparison With Choroidal Nevus. Arch Ophthalmol 130(7):850-856.
- Salman A, Parmar P, Rajamohan M, Vanila CG, Thomas PA et al. (2006) Optical Coherence Tomography in Choroid Tuberculosis. Am J of Ophthalmol 142 (1): 170-172.
- Arej N, Fadlallah A, Chelala E (2016) Choroidal Tuberculoma as a Presenting Sign of Tuberculosis. Int Med Case Rep J 9:365-368.

