Background: Eosinophilic myocarditis is a rare and under-recognized subtype of myocarditis. The signs and symptoms are non-specific, most often mimicking other diseases, leading to a late, and sometimes, incorrect diagnosis. This disease can be self-limiting, however, if not detected early, can progress to a fatal outcome.
Case Presentation: A 33-year-old female, known asthmatic was admitted due to recurrent chest pain, dyspnea and abdominal pain. ECGs showed transient ST segment elevation. The cardiac enzymes, WBC and eosinophil counts were significantly elevated. Coronary angiogram was normal. 2D echocardiogram showed concentric hypertrophy with segmental hypokinesia, normal LV EF, severe mitral regurgitation, with signs of diastolic dysfunction. Cardiac MRI showed mild diffuse myocardi10.21767/2471-8505.100060al edema and a patchy subendocardial enhancement. After initiation of steroid therapy, there was dramatic improvement in the symptoms and peripheral eosinophilia. Repeat 2D echocardiogram after several months was normal. Early discontinuation of steroids resulted in recurrence of cardiac events.
Conclusion: Eosinophilic myocarditis, though uncommon, should be considered as a differential diagnosis in patients with acute coronary syndrome-like symptoms, history of asthma and allergies, a normal coronary angiogram, with or without peripheral eosinophilia. An echocardiogram and a cardiac MRI can support the diagnosis, however, endomyocardial biopsy remains to be the gold standard. Prompt recognition and immediate steroid therapy are important keys in managing this rare disease.
Introduction
Eosinophilic myocarditis (EM) is a rare type of myocarditis characterized by diffuse or focal myocardial inflammation with eosinophilic infiltration, most often associated with peripheral eosinophilia. X syndrome is defined as an absolute eosinophil count greater than 1.5 × 109/L lasting for more than six months in the absence of any known cause of hypereosinophilia with evidence of organ involvement. Cardiac disease is the major cause of morbidity and mortality in patients with this syndrome, occurring in about 50% of patients with idiopathic hypereosinophilic syndrome [1, 2]. EM can present with a wide range of symptoms and can easily be missed or diagnosed late. In severe cases, it can lead to a fatal outcome if not recognized and managed early.
Case Presentation
A 33 year old Filipino female, known asthmatic, with a history of gastritis and allergies to NSAIDs and Paracetamol, came to the emergency room due to a two-week history of recurrent chest pain, radiating to the right jaw and shoulder, accompanied by dyspnea and diaphoresis. Workups at the ER showed ST segment elevation in the inferior and anterolateral wall in the ECG, elevated cardiac enzymes (Troponin T 1053 ng/L; CK-MB 27), with CBC showing leukocytosis (WBC 10.21, eosinophilia 26%, absolute eosinophil count of 2,654/mm3 and thrombocytosis 506,000). The patient was initially managed as a case of ST-elevation MI and subsequently underwent emergency coronary angiogram, which showed non-obstructive CAD. ST segment elevation was noted to have resolved after the procedure. Coronary vasospasm versus spontaneous lysis of the thrombus was considered at that time and the patient was started on nitrates and calcium-channel blocking agent.
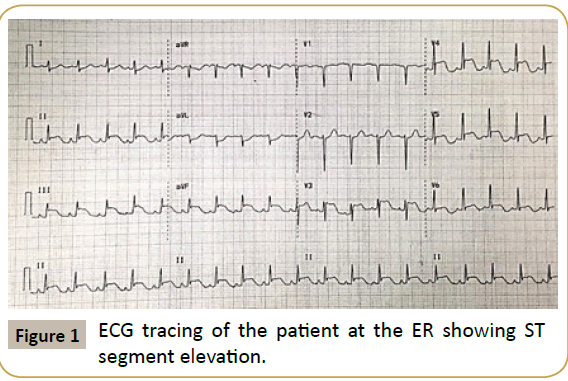
Figure 1: ECG tracing of the patient at the ER showing ST segment elevation.
During the course of her admission, the patient continued to have on and off chest pain, with transient ST segment elevation. 2D echo showed concentric LVH, with hypokinetic postero-inferior LV free wall from base to apex, anterior IVS and anterior LV free wall from mid to apex, normal ejection fraction of 62%, with moderate to severe mitral regurgitation, and Doppler evidence of stage III restrictive filling pattern and mild pulmonary hypertension. Cardiac MRI showed diffuse mild myocardial edema on T2-weighted imaging and segmental subendocardial enhancement involving the apex, apical septal, inferior and lateral walls, midventricular anteroseptal wall, and basal anteroseptal wall with a patchy delayed enhancement involving the posteromedial papillary muscle. The cardiac MRI findings are consistent with ischemic cardiomyopathy. However, in the absence of coronary artery disease as evidenced by the normal angiogram and with a history of eosinophilia, eosinophilic myocarditis was considered. The patient was then started on lowdose Prednisone with subsequent dramatic improvement in her symptoms and significant decrease in her peripheral eosinophilia.
The patient has been non-compliant with her medications and was subsequently re-admitted twice in our institution, after selfdiscontinuation of steroids, due to abdominal pain, dyspnea and chest pain, with re-elevation of her cardiac enzymes and eosinophil count (absolute eosinophile count range of 4,800 to 6,965/mm3). On her third hospital admission, she presented with mild heart failure symptoms and was also noted to have erythematous, pruritic rashes on both upper and lower extremities which were not noted in the previous two admissions. The patient was again given steroids, with subsequent rapid improvement of her condition and return of cardiac enzymes and eosinophil count to normal levels (Figure 1).
Discussion
Infiltration of eosinophils in the myocardium can lead to myocardial inflammation or eosinophilic myocarditis (EM). To date, there are very limited data available on this disease and majority of the cases are diagnosed either late or post-mortem. The signs and symptoms can be non-specific, which can lead to either a delay in the recognition of EM or to an incorrect diagnosis. Patients can present with fever, cough, chills, skin rashes, malaise, weight loss, abdominal pain, vomiting, chest pain and other acute coronary syndrome-like symptoms, heart failure symptoms, arrhythmias and sudden death. Coronary vasospasm, demonstrated using intracoronary acetylcholine infusion, is one cause for chest pain in patients with clinical signs of myocarditis in the absence of significant coronary atherosclerosis. Chest pain may also mimic that in pericarditis, suggesting epicardial inflammation with adjacent pericardial involvement [3].
Degranulation of eosinophils with release of major basic protein is implicated in the pathologic process of the disease. Major basic protein is also a potent stimulator of platelets that result in cardiac thrombi [4]. In some studies, the release of eosinophilic cationic protein has also been implicated in contributing to myocardial damage. Myocyte death caused by necrosis and apoptosis plays a role in the development of heart failure; furthermore, myocardial fibrosis can occur despite treatment and puts the patient at high risk for fatal arrhythmias [1]. The exact mechanism for the affinity of eosinophils for cardiac myocytes is still unknown.
Up to the present time, there has been no generally accepted guideline for the diagnosis and management of EM. However, in 2009, the Japanese Circulation Society Task Force Committee on Acute and Chronic Myocarditis formulated useful diagnostic criteria for EM [5]. It was stated that EM should be strongly suspected if a patient has met the five minimal requirements for diagnosis, which include: (1) Peripheral eosinophil count of >500/mm3, (2) Cardiac symptoms such as: chest pain, dyspnea, and palpitations; (3) Elevated cardiac enzymes; (4) ECG changes including ST elevation (observed in 50% of the patients) and abnormal Q waves; (5) Transient left ventricular wall thickening and wall motion abnormality on echocardiography; and that acute myocardial infarction has been ruled out by coronary angiography. Additional useful information includes: the presence of allergic conditions (such as asthma, rhinitis and urticarial), and previous flu-like symptoms (such as fever, sore throat and cough). Diagnosis must be confirmed by endomyocardial biopsy [5], which remains to be the gold standard for diagnosis. However, the sensitivity of endomyocardial biopsy based on autopsy specimens was estimated to be around only 54%, given the often patchy nature of the disease and this is likely even lower in the beating heart due to the technical difficulties of the biopsy procedure [6]. The presence of peripheral eosinophilia may help the cardiologist in suspecting EM; however, there has been a rare reported case of histologically confirmed eosinophilic myocarditis without peripheral eosinophilia. Therefore, the presence of peripheral eosinophilia alone is not a reliable indicator for the diagnosis and treatment response of EM and its absence does not rule out the diagnosis either. Some studies mentioned eosinophilic cationic protein (ECP), a toxic protein from the degranulation of eosinophils, as a more effective supplementary diagnostic tool instead of peripheral eosinophil count. Ito et al. published a pediatric case report demonstrating the usefulness of eosinophilic cationic protein (ECP), as a marker for the diagnosis of EM and its efficacy in monitoring treatment response [7].
Non-invasive and readily available cardiac imaging modalities that can help support the diagnosis of EM include echocardiography and cardiac MRI. There are no known specific echocardiographic findings in EM. However, commonly cited findings include left ventricular dysfunction as evidenced by segmental wall motion abnormalities, and reversible left ventricular hypertrophy [2]. There was a case report published by Liao et al. in 2012 wherein he reported a case of acute necrotizing EM in a young Filipino woman. According to that report, the hallmarks of echocardiography in EM include endocardial infiltration, apical thrombus formation and endocardial fibrosis as the disease progresses. The geometrics of heart involvement are uniquely confined to the LV basal segment of the posterior wall, and further impair the motion of the posterior mitral leaflet to cause eccentric mitral regurgitation. Furthermore, diastolic dysfunction is always seen, and restrictive cardiomyopathy is evident in the chronic stage [8].
Cardiac MRI, on the other hand, is the only non-invasive method used to visualize the extent of endomyocardial involvement in the diagnosis and treatment of eosinophilic myocarditis [9]. T2- weighted imaging can detect myocardial edema while delayed enhancement imaging is capable of detecting myocardial fibrosis and inflammation associated with EM as well as subendocardial delayed enhancement. The extent of hyper-enhancing myocardium in delayed enhancement images was inversely correlated with the LV EF [10]. The cardiac MRI findings however all decrease with time. Its sensitivity and specificity in suspected myocarditis were poor if taken more than 14 days after symptom onset (63% and 40%, respectively) [3]. Therefore, it is ideal to have the cardiac MRI done early in the disease course.
Due to the limited available data, there has been no randomized controlled trial or guidelines developed for the definitive management of EM. Given its wide range of severity, the initial management should include supportive treatment, stabilization of the hemodynamic status and standard heart failure regimen if warranted. Reversible factors that are contributing to the eosinophilia (such as parasites, allergic disease, drug-induced allergy) should also be addressed. Steroid therapy has remained to be the mainstay therapy in various case reports based on the inflammatory nature of the disease. In a recent retrospective case series by Kawano and colleagues in 2011, who were the first authors to propose the initiation and maintenance doses of prednisolone based on disease severity as follows: Initial 1 g methylprednisolone pulse dose was reserved for patients with pre-cardiac tamponade, cardiogenic shock, and pulmonary edema; 1 mg/kg/day of prednisolone for more stable patients; and 5-10 mg/day dose of prednisolone was subsequently given to prevent relapse with good outcomes [11]. This dosing regimen remains to be validated in a much larger study.
Conclusion
Eosinophilic myocarditis, though uncommon, should be considered as a differential diagnosis in patients with acute coronary syndrome-like symptoms, history of asthma and allergies, a normal coronary angiogram, with or without peripheral eosinophilia. An echocardiogram and a cardiac MRI can support the diagnosis and may be used to monitor treatment with reversible myocardial changes. However, endomyocardial biopsy remains to be the gold standard for diagnosis. Eosinophilic myocarditis has the potential to become rapidly fatal and prompt recognition and immediate steroid therapy is the cornerstone of managing this rare disease.
References
- Al Ali AM, Straatman LP, Allard MF, Ignaszewski AP (2006) Eosinophilic myocarditis: case series and review of literature. Can J Cardiol 22: 1233-1237.
- Rizkallah J, Desautels A, Malik A, Zieroth S, Jassal D, et al. (2013) Eosinophilic myocarditis: Two case reports and review of the literature. BMC Research Notes 6: 538.
- Douglas LM, Douglas PZ, Peter L, Robert OB (2015) Braunwald’s heart disease, A Textbook of Cardiovascular Medicine, 10th edition. Elsevier Saunders, Philadelphia.
- Senthil KT, Hema LK, Amy JA, William JH, Mark JH (2009) Acute eosinophilic myocarditis mimicking myocardial infarction. Tex Heart Inst J 36: 355-357.
- JCS (2009) Japanese circulation society task force committee on acute and chronic myocarditis: Guidelines for diagnosis and treatment of myocarditis.
- Burke AP, Saenger J, Mullick F, Virmani R (1991) Hypersensitivity myocarditis. Arch Pathol Lab Med 115: 764-769.

- Reiko I, Takuma S, Kiyoshi Y, Mari I, Yukoh A (2003) Usefulness of eosinophilic cationic protein as a marker of eosinophilic myocarditis in a child. Allergol Int 52: 219-224.
- Liao YC, Su CS, Teng CL, Wang KY, Lin FY, et al. (2012) Acute necrotizing eosinophilic myocarditis in a young woman. J Chin Med Assoc 75: 536-538.
- Debl K, Djavidani B, Buchner S, Poschenrieder F, Heinicke N, et al. (2008) Time course of eosinophilic myocarditis visualized by CMR. J Cardiovasc Magn Reson 10: 21.
- Tani H, Amano Y, Tachi M, Machida T, Mizuno K, et al. (2012) T2-weigted and delayed enhancement MRI of eosinophilic myocarditis: relationship with clinical phases and global cardiac function Jpn J Radiol 30: 824-831.
- Kawano S, Kato J, Kawano N, Yoshimura Y, Masuyama H, et al. (2011) Clinical features and outcomes of eosinophilic myocarditis patients treated with prednisolone at a single institution over a 27 year period. Intern Med 50: 975-981.

