Ehrlé Nathalie1,2*, Cason Nia2, Vaunaize Jean3, Garcia Tony4 and Bakchine Serge1
1Neurology Department, Reims Hospital, France
2PSITEC Laboratory, Université Lille 3, EA4072, France
3Courlancy Clinic, Reims, France
4EST Lyonnais Hospital, Saint Priest, France
*Corresponding Author:
Ehrlé Nathalie
Neurology Department, Reims Hospital, France
Tel: 33326783964/3089
Fax: 33326832668
E-mail: nehrle@chu-reims.fr
Received date: July 13, 2017; Accepted date: July 19, 2017; Published date: July 24, 2017
Citation: Nathalie E, Nia C, Jean V, Tony G, Serge B (2017) Multiple Sclerosis Presenting as Posterior Cortical Atrophy. Dual Diagn Open Acc 2:34. Doi: 10.21767/2472-5048.100034
Copyright: © 2017 Nathalie E, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Introduction
Posterior cortical atrophy (PCA) is a rare neurodegenerative syndrome, characterized by insidious and gradual visual impairment in the absence of primary ocular disease [1]. Pathologic studies have revealed that PCA is most often the clinical expression of an atypical form of Alzheimer pathology [2], named the visual variant. More rarely, PCA may be associated to other neurodegenerative etiologies, such as corticobasal degeneration, dementia with Lewy bodies, prion disease (Creutzfeldt-Jakob disease), and subcortical gliosis [1,3-5]. The clinical phenotype may vary according to the etiology, and may include elements of the Balint’s syndrome (optic ataxia, oculomotor apraxia, simultagnosia). Patients complain having inconsistent difficulties to distinguish lines, to read, to estimate distances, and to identify objects. Visual hallucinations are often reported. Clinical onset of PCA is usually observed during the 5th or 6th decades. Diagnosis is usually evoked on a very peculiar neurovisual pattern during cognitive testing and comforted by posterior (occipito-temporo-parietal atrophy on MRI, with clear cortical hypometabolism in the same regions on perfusion PET ou SPECT scans. [6-8]. We describe the case of a patient presenting with PCA syndrome, which was related to an atypical presentation of multiple sclerosis.
Case Report
A 64-year-old right-handed female was referred for a visual complaint. Her impairment was insidious and had progressively become worse for about four years, with a significant impairment of her daily life activities for the past 6 months. The patient had no previous history of neurological or ophthalmological pathology, except for a bilateral cataract surgery two years earlier. There was a familial history of dementia; her sister had presented with a cortical degenerative disease (diagnosed as probable Alzheimer’s disease) at the same age. Physical examination was normal.
For three years, the patient had reported complex visual difficulties which remained unexplained despite several ophthalmological examinations. She complained of being unable to properly see objects located beyond 7 feet, with some variability in clarity. Due to these reasons, she gave up the hunting. According to her husband, she was able to see the prey “only when it was right in front of her eyes”. The cataract surgery did not change her condition. She became lost several times while driving her car in a familiar environment, seeing clearly but being unable to identify her usual landmarks. A simultagnosia (a decrease in the amount of perceived visual information) was present. The patient complained of her inability to see a jar that she previously put away in the usual cupboard. At home, she got used to put her things in the same place in order to easily find them again. She complained also of a gradual hypersensitivity to luminance, especially to intense red lights which “hurted the back of her eyes”. Six months before her referral, she became very disturbed by a discomfort triggered by visual motion. In her activity as a farmer, she experienced blurred vision when she feeded the fowls, which moved in every direction for this occasion. The same happened when she moved herself rapidly (e.g. when she jumped up). Except for this disability, the patient remained autonomous. She otherwise complained of mild memory difficulties. Her language remained fluent and unimpaired.
Neuropsychological assessment revealed no storage or language impairment (this point was previously discussed [6]. Table 1 summarizes the cognitive abilities of the patient compared to the usual PCA semiology.
| Cognitive abilities |
Patient results |
Usual features of PCA |
| Intellectual efficiency |
IQ=65*; verbal IQ=70; performance IQ=66 |
Low efficiency at an advanced stage; usually, verbal IQ>performance IQ |
| Verbal and visual episodic memory |
Encoding and retrieval impairments without storage difficulties |
Unusual at early stage |
| Reading of isolated words and pseudo-words |
- but not prevailing for large-printed, spaced letters and lengthy words |
Cognitive marker: peripheral alexia (difficulties to see the letters or reading letter by letter without agraphia or oral language impairment); more pronounced for large-printed, spaced letters and lengthy words |
| Verbal fluency |
- |
Usually preserved at early stage |
| Images naming |
- agnosia |
Cognitive marker: agnosia, prosopagnosia |
| Praxia |
+ |
Cognitive marker with visuospatial errors and dressing apraxia |
| Cancellation test |
+ but slowing |
Cognitive marker (probably consecutive to agnosia and simultagnosia) |
| Embedded figures test |
- simultagnosia |
Cognitive marker |
| Objects drawn from memory |
- |
Cognitive marker |
| Detection of primitives (line orientation) |
+ |
Cognitive marker |
| Discrimination of 2D geometrical forms |
+ |
Possibly impaired |
| Discrimination of 3D geometrical forms |
- |
Cognitive marker |
| Navon letters (a big letter made up of small letters) |
-for identification of big letters
+for small letters |
Cognitive marker |
| Optic ataxia |
+ (absent whatever the quadrant of visual field and the pointing hand) |
Cognitive marker |
| Graphic fluency |
- |
Impairment resulting from visual perceptual deficit |
| Executive test implying abstraction and flexibility |
- |
Possibly impaired at late stage |
| Frises |
+ |
Impairment resulting from visual perceptual deficit; flexibility errors possible |
| Visual hallucinations |
+ (absent) |
Cognitive marker |
| Anxiety or depression |
+ (absent) |
Mood marker |
Table 1: Results of neuropsychological examination compared to PCA regular semiology.
An MRI scan was performed three years ago was interpreted as showing on the T1 sequences a bilateral posterior cortical atrophy. A few supra tentorial hypersignals were observed on T2 FLAIR sequences without any contrast enhancement, which were considered as not relevant. A second MRI scan was performed one year later which was interpreted as showing an increased posterior atrophy (Figure 1). The diagnosis of PCA was suggested by a neurologist. A SPECT scan was performed a few months later, but the result was apparently not confronted with the PCA diagnosis (Figure 2).
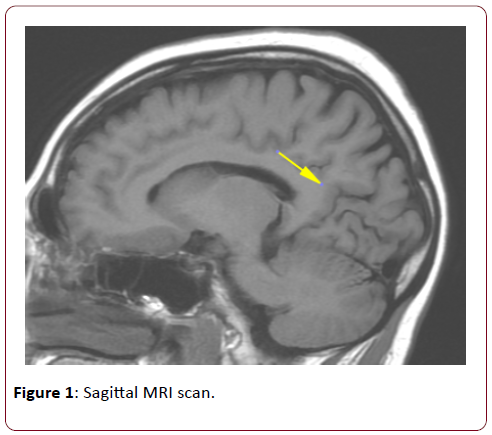
Figure 1: Sagittal MRI scan.
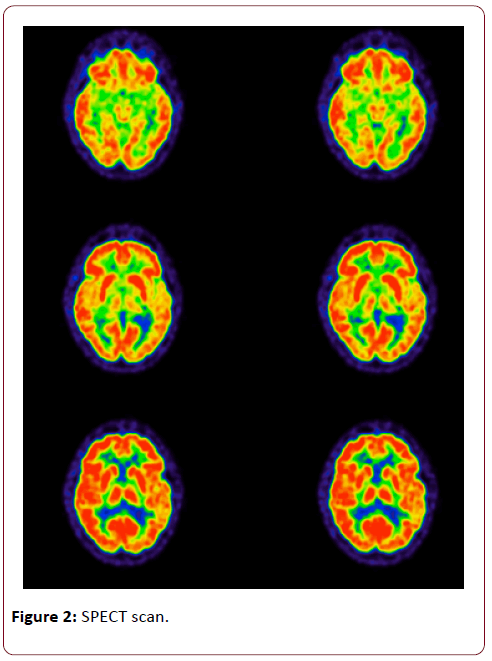
Figure 2: SPECT scan.
Discussion
In this case, several criteria were highly suggestive of a PCA: the insidious and progressive installation of visual symptoms, their selectivity, and age at onset. MRI also showed a significant posterior and bilateral atrophy [7-9]. Neuropsychological assessment revealed some signs compatible with PCA, such as visual aperceptive agnosia (discrimination of 3D objects), associative agnosia (drawing from memory), simultagnosia, environmental disorientation, and alexia. However, some cognitive and mood markers were absent, such as dressing apraxia, visual hallucinations, impairment of primitives’ detection (which is a good marker for primary cortex dysfunction), and significant depression and/or anxiety. Reading was impaired (alexia) but without the inverse size effect (increased difficulties for large-printed letters), including with spaced letters and lengthy words [10]. Balint syndrome, characteristic of PCA, was also incomplete with a simultagnosia (without optic ataxia or oculomotor apraxia). The painful hypersensitivity to red light was also atypical and more suggestive of optical nerve injury. Moreover, the result of the SPECT scan was clearly unfit with the diagnosis of PCA, as the aspect of visual associative regions was normal (when it shows usually a clear hypometabolism in PCA).
The spinal MRI was normal as was the electromyogram of inferior limbs. The neuro-ophthalmological examination revealed an acuity of 8/10 for monocular and binocular vision, a papillary pallor, evocative of a bilateral atrophy of optic nerve. This was confirmed by laser optical coherence tomography and bilaterally disturbed evoked potentials (increased latency and decreased amplitude of the P100 component). These signs, associated with diffuse subcortical FLAIR hyperintensities, were highly suggestive of multiple sclerosis. The patient next received corticotherapy, which improved the visual symptoms.
Conclusion
Visual impairment is common in multiple sclerosis, implying anterior and posterior pathways, with optic neuritis as the most common afferent pathway symptom (50% of these patients [11]; see [12] for a review). The timing of axonal and neuronal loss seems to decrease with illness duration, which emphasizes the necessity of early care [13]. The wide variety of visual complaints in multiple sclerosis can lead to clinical confusion [14,15]. Recent literature highlights the unusual semiology of this autoimmune demyelinating disorder (pain syndromes, movement disorders, rare cranial nerve involvement, cognitive or psychiatric symptoms [16,17]. In this case, both a late onset and an atypical clinical pattern were misleading. The patient presented with progressive evolution of selective visual impairment, when motor symptoms are reported as prominent in late-onset multiple sclerosis [18]. For clinical diagnosis, a discriminating analysis of visual semiology and MRI are essential.
References
- Crutch SJ, Lehmann M, Schott JM, Rabinovici GD, Rossor MN, et al. (2012) Posterior cortical atrophy. Lancet Neurol 11: 170-178.
- Suárez-González A, Crutch SJ, Franco-Macías E, Gil-Néciga E (2016) Neuropsychiatric Symptoms in Posterior Cortical Atrophy and Alzheimer Disease. J Geriatr Psychiatry Neurol 29: 65-71.
- Alladi S, Xuereb J, Bak T, Nestor P, Knibb J, et al. (2007) Focal cortical presentations of Alzheimer’s disease. Brain 130: 2636–2645.
- Galton CJ, Patterson K, Xuereb JH, Hodges JR (2000) Atypical and typical presentations of Alzheimer's disease: a clinical, neuropsychological, neuroimaging and pathological study of 13 cases. Brain 123: 484-498.
- Giorelli M, Losignore NA, Bagnoli J, Difazio P, Zimatore GB (2014) The progression of posterior cortical atrophy to corticobasal syndrome: lumping or splitting neurodegenerative diseases. 24: 1-4.
- Ehrlé N, Bakchine S, Garcia T, Vaunaize J (2016) Approche diagnostique de l'atrophie corticale. In Vingt cas cliniques en neuropsychologie. Dunod éditeur.
- Lehmann M, Ghosh PM, Madison C (2013) Divergin patterns of amyloid deposition and hypometabolism in clinical variants of probable Alzehimer's disease. Brain 136: 844-858.
- Scheltens NM, Galindo-Garre FPijnenburg YA, Van der Vlies AE, Smits LL, et al. (2015) The identification of cognitive subtypes in Alzheimer's disease dementia using latent class analysis. J Neurol Neurosurg Psychiatry
- Slattery CF, Crutch SJ, Schott JM (2015) Phenotypical variation in Alzheimer disease: insights from posterior cortical atrophy. Pract Neurol 15: 2-4.
- Yong KX, Shakespeare TJ, Cash D, Henley SM, Warren JD, et al. (2014) Context-specific effects of visual dysfunction on reading in posterior cortical atrophy. Cortex 57: 92-106.
- Yoshida Takemura M, Hori M, Yokoyama K, Hamasaki N, Suzuki M, et al. Alterations of the optic pathway between unilateral and bilateral optic nerve damage in multiple sclerosis as revealed by the combined use of advanced diffusion kurtosis imaging and visual evoked potentials. Magnetic Resonance Imaging 39: 24-30.
- Balcer LJ, Miller DH, Reingold SC, Cohen JA (2015) Vision and vision-related outcome measures in multiple sclerosis. Brain 138: 11-27.
- Balk LJ, Cruz-Herranz A, Albrecht P, Arnow S, Gelfand JM, et al. (2016) Timing of retinal neuronal and axonal loss in MS: a longitudinal OCT study. J Neurol 263: 1323–1331.
- Costello F (2016) Vision Disturbances in Multiple Sclerosis. Semin Neurol 36: 185-95.
- Torres-Torres R, Sanchez-Dalmau BF (2015) Treatment of acute optic neuritis and vision complaints in multiple sclerosis. Curr Treat Options Neurol 17: 328.
- Evlice A, Demir T, Kalea?as? C, Özcan F, Demirk?ran M (2016) Rare onset symptoms in multiple sclerosis. Acta Clin Belg 21: 1-4.
- Yetimalar Y, Seçil Y, Inceoglu AK, Eren S, Ba?o?lu M (2008) Unusual primary manifestations of multiple sclerosis. N Z Med J 4: 47-59.
- Kis B, Rumberg B, Berlit P (2008) Clinical characteristics of patients with late-onset multiple sclerosis. J Neurol 25: 697-702.