Abdurrahman Sönmezler1* and ?akir Özgür Ke?kek2
1Department of Neurology, Adana City Research and Training Hospital, Adana, Turkey
2Department of Internal Medicine, Adana City Research and Training Hospital, Adana, Turkey
*Corresponding Author:
Abdurrahman Sönmezler
Assistant Professor
Department of Neurology
Adana City Research and Training Hospital, Adana, Turkey
Tel: +905323951977
E-mail: sonmezlera@gmail.com
Received Date: January 16, 2019; Accepted Date: February 05, 2019; Published Date: February 12, 2019
Citation: Sönmezler A, Ke?kek SO (2019) Low serum phosphorus levels and acute ischemic stroke. J Intensive Crit Care 5:3, doi: 10.21767/2471-8505.100122
Keywords
Acute ischemic stroke; Mortality; Serum phosphorus level
Introduction
Phosphorus plays an important role in delivery of oxygen to tissues by regulating the level of 2,3-DPG and ATP in erythrocytes. It is part of an important urinary buffer system permitting excretion of fixed acids. It is critical in the defence against infectious organisms. Phosphorus could have an important role in the brain where oxidation of glucose through the Krebs cycle is necessary for synthesis of ATP [1]. Studies related to phosphorus and ischemic stroke mortality in NICU has not adequate. The association between serum levels of phosphate and stroke has been investigated in studies, with controversial results [2-4]. There are many studies on phosphorus and cardiovascular diseases in the literature; hypophosphatemia can induce heart failure even in healthy subjects [5]. The myocardial concentrations of creatine phosphate and inorganic phosphate are significantly reduced during a phosphate depletion period, along with the mitochondrial and myofibrillar creatine phosphokinase activity, which has a crucial role in skeletal and cardiac muscle contractility [6]. Studies have shown that the creatine phosphate to ATP ratio is reduced in heart failure and is a strong predictor of prognosis [7-11]. Furthermore, cytoplasmic phosphate increases drastically with work rate in skeletal muscle and in the heart [12]. Therefore, phosphate levels are associated with ejection fraction [13]. Hypophosphatemia has been associated with ventricular arrhythmias additionally; low phosphate serum levels are common in the early stages of sepsis [14]. Due to the low ejection fraction and arrhythmias cerebral circulation may be adversely affected. In this study, 86 patients with acute ischemic stroke were examined with respect to phosphorus level in neurology intensive care unit in a tertiary hospital.
Materials and Methods
This study was performed at Adana City Training and Research Hospital between September 2017 and July 2018. A total of 86 patients with acute ischemic stroke were included in this retrospective study. Patients who stayed at least 24 hours in NICU were included the study. Patients with haemorrhagic stroke, chronic renal failure, hepatic failure, hearth failure were excluded from the study. In all cases, measurements were taken of the participants ‘serum phosphorus, magnesium, glucose, lipids, AST, ALT, creatinine levels and complete blood counts. Phosphorus levels were analysed using the phosphomolybdate method, with the Beckman Coulter Synchron LX20 (Danvers, MA), and the reference range was from 2.5-4.6 mg/dL. Magnesium levels were analysed with the Roche C-501 (Japan) using the colorimetric method. The reference levels range was between 1.9-2.6 mg/dL. Glucose, lipids, ASTs, ALTs, creatinine levels were analysed on the Beckman Coulter Synchron LX 20 (Massachusetts, USA). Complete blood counts were measured by on the Sysmex XE 2100i (Japan). For statistical evaluation MedCalc 15.8 software program (MedCalc Belgium) was used. Mean standard deviation values of the data were recorded. The Student's t-test was used to compare normal quantitative independent data and the Mann-Whitney U-test was used to compare independent quantitative data without normal distribution. Pearson correlation coefficient was used to analyse the degree of association between two variables. A log transformation was used for the variables that were not normally distributed. Chi-square test was used to compare qualitative data. Data were assessed at 95% confidence interval and p<0.05 values were considered as significant.
Result
The data of 86 patients with acute ischemic stroke who were admitted to the NICU for a period of approximately one year were examined retrospectively. There were 50 (65.7%) patients who survived while there were 36 (34.3%) patients who died. Of the survivor patients and died patients, 29 (58.0%) and 23 (63.9%) patients were female retrospectively (p=0.583). The mean age of survivors was 71.6 ± 13.9 and the mean age of deaths was 72.56 ± 13.6 years. The difference was not statistically significant (p= 0.762). There was no significant difference in mortality rates between sexes. Furthermore; there was no statistically significant difference between the groups according to the blood glucose (118.2 ± 18.7 vs. 122.0 ± 40.8) (p=0.564), creatinine (0.75 ± 0.22 vs. 0.66 ± 0.23) (p=0.054), haemoglobin (11.6 ± 1.9 vs. 12.3±2.1) (p=0.135), white blood cells (11.4 ± 4.5 vs. 12.3 ± 4.2) (p=0.360), red blood cells (4.35 ± 0.77 vs. 4.16 ± 0.48) (p=0.184), platelets (274.8 ± 115.6 vs. 240.5 ± 94.5) (p=0.147). The mean magnesium value of the patients who died (1.73 ± 0.14) was significantly lower than that of the living patients (2.1 ± 0.18) (p<0.001). Mean Glasgow coma score (GCS) was 5.3 ± 1.6 of died, 9.3 ± 1.1 of the survived patients (p<0.001). Phosphorus levels were correlated with GCS score (p<0.001, r=0.491) (Table 1 and Figure 1).
| |
Survived (N=50) |
Ex (N=36) |
P |
| Age (years) |
71.6 ± 13.9 |
72.5 ± 13.6 |
0.762 |
| Female N (%) |
29(58.0%) |
23(63.9%) |
0.583 |
| Creatinine mg/dL |
0.75 ± 0.22 |
0.66 ± 0.23 |
0.054 |
| Phosphorus mg/dL |
3.14 ± 0.2 |
2.77 ± 0.39 |
<0.001 |
| Glucose mg/dL |
118.2 ± 18.7 |
122.0 ± 40.8 |
0.564 |
| Glasgow coma score |
9.3 ± 1.1 |
5.3 ± 1.6 |
<0.001 |
Table 1 Demographical and biochemical data of the groups.
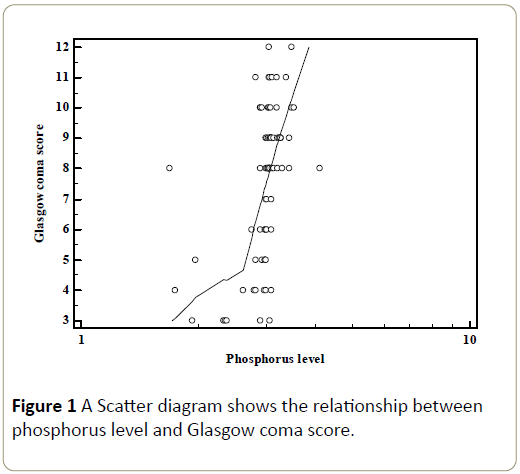
Figure 1: A Scatter diagram shows the relationship between phosphorus level and Glasgow coma score.
Discussion
In this study, we analysed 86 patients with acute ischemic stroke according to the phosphorus level. Moreover, we investigated GCS phosphorus association. We have found low levels of phosphorus in died patients. The relationship between ischemic stroke and phosphorus has not been extensively reviewed in previous publications. Massry has shown the clinical syndrome of phosphate depletion. According to Massry’s study on phosphate depletion, the syndrome can lead to disturbances in the central nervous system, hematopoietic system, parathyroid glands, cardiac function, renal function, and also in muscles and bones [15]. The low levels of phosphorus affect the organs; a decrease in 2,3-diphosphoglycerate in red blood cells leads to tissue hypoxia, mitochondrial energy production decreases due to low tissue content of ATP. Correspondingly, hypoxia in the tissue and energy deficiency in the cells may lead to organ failure [16]. Studies examining acute ischemic stroke and phosphorus levels have produced only a few results. Wannamethee et al. [2] concluded that their study find a relationship between raised serum phosphorus levels and increased total mortality of stroke cases. Li et al. [3] concluded that there is no association between serum level of phosphate and stroke. Aronson et al. [4] reported that higher phosphorus levels were also associated with increased risk of heart failure, but not the risk of myocardial infarction or stroke.
The results of studies evaluating the relationship between phosphorus and stroke prognosis are inadequate. The studies about the association between acute ischemic stroke mortality and hypophosphatemia are insufficient. In our study, we have found significant relationship between phosphorus levels and mortality in acute ischemic stroke. To our knowledge whether correlation between phosphorus levels with acute ischemic stroke mortality in NICU has not been described before.
This study has some limitations. First, it would have been beneficial if the sample size could be larger. Second, we did not measure the level of PTH (parathyroid hormone), fibroblast growth factor 23 (FGF23).
In conclusion, serum phosphorus level can be associated with mortality in patients with acute ischemic stroke. When working on strengthening intensive care scoring systems with laboratory parameters, the phosphorus levels need to be further examined. Presence of hypophosphatemia in the ICU patients may be a preliminary finding for other organ damage as brain.
Significance of the Study
Inadequate results have been shown about the phosphorus levels and stroke. This study supports that low serum phosphorus level may associated with mortality of cerebral infarction. Presence of hypophosphatemia in intensive care unit patients may be a preliminary finding for other organ damage such as brain.
Acknowledgement
The authors have no financial or personal relationships with other people or organizations that could pose a conflict of interest in connection with the present work.
References
- Knochel JP (1977) The pathophysiology and clinical characteristics of severe hypophosphatemia. Arch Intern Med 137: 203-220.
- Wannamethee SG, Sattar N, Papcosta O, Lennon L, Whincup PH (2013) Alkaline phosphatase, serum phosphate, and incident cardiovascular disease and total mortality in older men. Arterioscler Thromb Vasc Biol 33: 1070-1076.
- Li JW, Xu C, Xiao YB (2014) Serum phosphate concentration and incidence of stroke: a systemic review and meta-analysis. Neurol Sci 35: 1877-1882.
- Aronson D, Kapeliovich M, Hammerman H, Dragu R (2013) The Relation between Serum Phosphorus Levels and Clinical Outcomes after Acute Myocardial Infarction. PLoS One 8: e58348.
- Pesta DH, Tsirigotis DN, Befroy DE, Caballero D, Jurczak MJ, et al. (2016) Hypophosphatemia promotes lower rates of muscle ATP synthesis. FASEB J 30: 3378-3387.
- Brautbar N, Altura BM (1987) Hypophosphatemia and hypomagnesemia result in cardiovascular dysfunction: theoretical basis for alcohol-induced cellular injury. Alcohol Clin Exp Res. 11: 118-126.
- Neubauer S, Horn M, Cramer M, Harre K, Newell JB, et al. (1997) Myocardial phosphocreatine-to-ATP ratio is a predictor of mortality in patients with dilated cardiomyopathy. Circulation 96: 2190-2196.
- Neubauer S, Krahe T, Schindler R, Horn M, Hillenbrand H, et al. (1992) 31P magnetic resonance spectroscopy in dilated cardiomyopathy and coronary artery disease. Altered cardiac high-energy phosphate metabolism in heart failure. Circulation 86: 1810-1818.
- Neubauer S (2007) The failing heart--an engine out of fuel. N Engl J Med 356: 1140-1151.
- Beer M, Seyfarth T, Sandstede J, Landschütz W, Lipke C, et al. (2002) Absolute concentrations of high-energy phosphate metabolites in normal, hypertrophied, and failing human myocardium measured noninvasively with (31)P-SLOOP magnetic resonance spectroscopy. J Am Coll Cardiol 40: 1267-1274.
- Bizino MB, Hammer S, Lamb HJ (2014) Metabolic imaging of the human heart: clinical application of magnetic resonance spectroscopy. Heart 100: 881-890.
- Beard DA (2006) Modeling of oxygen transport and cellular energetics explains observations on in vivo cardiac energy metabolism. PLoS Comput Biol 2: e107.
- Ke?kek ?Ö, Sa?l?ker Y, K?r?m S, ?çen YK, Y?ld?r?m A (2015) Low Serum Phosphorus Level in Massry's Phosphate Depletion Syndrome May Be One of the Causes of Acute Heart Failure. J Nutr Sci Vitaminol (Tokyo) 61: 460-464.
- Schwartz A, Brotfain E, Koyfman L, Kutz R, Gruenbaum SE, et al. (2014) Association between Hypophosphatemia and Cardiac Arrhythmias in the Early Stage of Sepsis: Could Phosphorus Replacement Treatment Reduce the Incidence of Arrhythmias? Electrolyte Blood Press 12: 19-25.
- Massry SG (1987) The clinical syndrome of phosphate depletion. Adv Exp Med Biol 103: 301-312.
- Lichtman MA, Miller DR, Cohen J, Waterhouse C (1971) Reduced red cell glycolysis, 2, 3-diphosphoglycerate and adenosine triphosphate concentration, and increased hemoglobin-oxygen affinity caused by hypophosphatemia. Ann Intern Med 74: 562-568.

