Keywords
Calipers; cataract surgery; corneal diameter; IOLMaster
Introduction
The corneal diameter as determined by the horizontal white to white (WTW) is an important measurement that has diverse clinical applications within the field of ophthalmology. In the clinic, microphthalmia, relative anterior microphthalmia, microcornea, macrophthalmia, and macrocornea are examples where the measured corneal diameter is important. In the operating room, surgeons have relied upon the measured corneal diameter for sizing of some types of intraocular lenses. Yet, exact estimation of the normal horizontal corneal diameter range is vague, and the current definitions of microcornea and macrocornea referenced in many different textbooks vary from source to source. Some define microcornea in adults as anywhere from 10.0 [1-6] to 11.0 mm [7-8] or less. Similarly, the definition of macrocornea can vary anywhere from 12.5 [6] to 13.0 [1-5,8] mm or greater, although there is general consensus among clinicians that the current accepted standards of normal WTW is greater than 11.0 mm and less than 13.0 mm. The ranges referenced in textbooks are based on measurements taken with manual calipers, as automated devices are a relatively new development that have only appeared within the last two decades.
Few studies have sought out to re-evaluate this parameter and attempt to more precisely define the “normal” WTW diameter. A study published by Rufer, et al. in 2005 used Orbscan® to evaluate corneal diameters of 390 subjects found that normal limits, defined as the mean ± 2 standard deviations, were between 10.7 and 12.6 mm [9]. This study was limited by one measuring technique and did not include comparison with the IOLMaster, which is the device regarded as having the highest reliability in measuring corneal diameter as compared to other methods [10]. Another recently published study in rural China by Fu, et al., used the IOLMaster to evaluate corneal diameters in 1721 subjects. The authors found a general WTW mean of 11.75 mm and a standard deviation of 0.40 mm. The range resulting from the mean ± 2 standard deviations was 10.95 mm to 12.55 mm [11]. Neither study included measurements taken with manual calipers. In our study, we evaluated horizontal WTW corneal diameter measurements using manual calipers, the traditional method of measuring WTW, in a group of cataract surgery patients for the purpose of re-evaluating the currently accepted definitions of normal horizontal WTW corneal diameter, microcornea and macrocornea. We also evaluated WTW using the IOLMaster to determine how measurements obtained with this automated device compared to the results obtained with traditional manual calipers.
Materials and Methods
The study was conducted as a retrospective chart review of cataract surgery patients operated on by senior author (RHO) at the Cincinnati Eye Institute (CEI) from September 2010 to November 2012. All patients had cataract surgeries performed in one or both eyes. Patient consent to treat was obtained before each surgical procedure. Pre-operative measurements with the IOLMaster (Carl Zeiss®, Meditec were performed by an experienced certified ophthalmic technician, which included either unilateral or bilateral measurement of the horizontal WTW corneal diameter. Manual caliper measurements were performed by the operating surgeon who adjusted the calipers (Bausch & Lomb Storz® Ophthalmics E-2404 Castroviejo Caliper, St Louis, MO) under the microscope by placing each tip on the limbus just beyond the clear corneal margins.
All statistical analyses were performed with SPSS® versions 21.0 and/or 23.0 (Armonk, NY). Descriptive analyses were performed to determine mean, range, standard deviation, and quartiles. Normal range was reported as mean ± 2 standard deviations from the mean. Frequencies of each WTW measurement value were counted and plotted in a histogram with estimated normal curve. To assess for correlation between age and corneal diameter, linear and logarithmic curve estimations were assessed. Resulting Pearson’s coefficient of determination (R2) was used to assess for significance of correlation.
To test whether diameters differed significantly according to gender or left versus right eye, independent t-test comparisons of corneal diameters were performed. To determine if there was significant difference between mean diameters obtained with calipers versus IOLMaster, paired t-test comparison and Bland Altman analysis were performed. Prior to all t-test comparisons, Levene’s test for equality of variances was performed to ensure equal variance between the two data sets. P-values of less than 0.05 were considered significant.
Results
Measurements were obtained from the charts of a total of 516 subjects. Ages range from 19 to 97 years (mean=73.7 years, median=74 years, mode=78 years). In terms of gender, there were 312 females and 204 males. Eight hundred twenty seven total eyes were measured with calipers. Nine hundred seventy seven total eyes were measured with IOLMaster. While all patients had caliper measurements, not all had been recorded in the operative note, resulting in fewer total caliper measurements than IOLMaster measurements included in the statistical analyses.
The mean corneal diameter was 12.22 mm with the calipers and 12.12 mm with the IOLMaster. Range was from 10.7 to 13.9 mm for the calipers and from 10.9 to 13.6 mm with the IOLMaster. Standard deviation from the mean was 0.52 mm for the calipers and 0.42 mm for the IOLMaster. Variance was 0.268 mm for the calipers and 0.177 mm for the IOLMaster. The resulting normal range (± 2 standard deviations) was 11.2 to 13.2 mm for the calipers and from 11.3 to 13.0 mm for the IOLMaster. 10%, 25%, 50%, 75% and 90% intervals were 11.6, 12.0, 12.1, 12.6 and 13.0 mm, respectively, with the calipers, and 11.6, 11.8, 12.1, 12.4 and 12.7 mm with the IOLMaster. With calipers, 12% of subjects had WTW measuring ≥ 13.0 mm and 2% had WTW measuring ≤ 11.0. Histograms of measurement frequencies obtained from calipers and IOLMaster are plotted in Figures 1 and 2, respectively.

Figure 1: Histogram of corneal diameters as measured by calipers with resulting normal curve superimposed on graph.
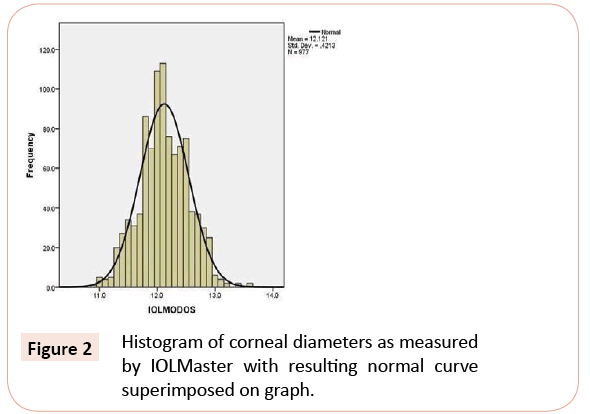
Figure 2: Histogram of corneal diameters as measured by IOLMaster with resulting normal curve superimposed on graph.
Corneal diameters measured with the calipers and the IOLMaster did not correlate significantly with age as assessed with both linear correlation (R2=0.047 for calipers; R2= 0.060 for IOLMaster) and logarithmic correlation (R2= 0.044 for calipers; R2= 0.048 for IOLMaster) (Figures 3 and 4).
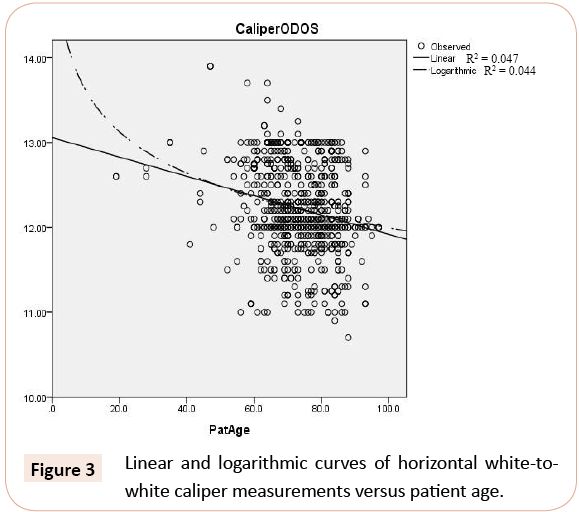
Figure 3: Linear and logarithmic curves of horizontal white-towhite caliper measurements versus patient age.
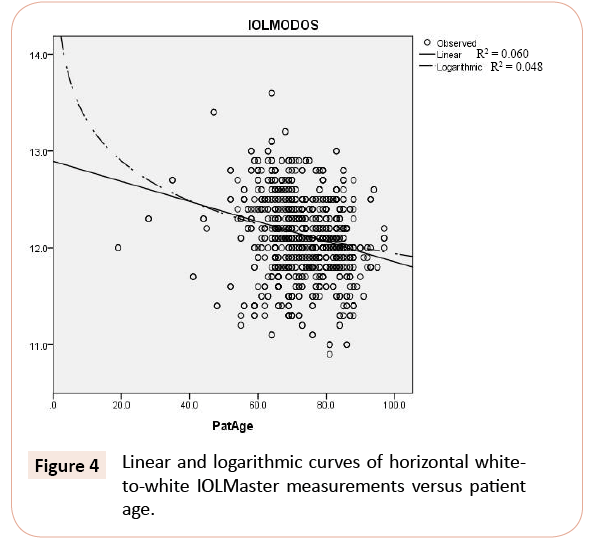
Figure 4: Linear and logarithmic curves of horizontal whiteto-white IOLMaster measurements versus patient age.
Males had slightly but significantly larger corneal diameters as compared to women with both calipers (mean difference=0.08 mm, p=0.04) and IOLMaster (mean difference=0.15 mm, p<0.001).
Equal variances were assumed according to Levene’s test (F=0.16, p=0.70 for calipers; F=0.007, p=0.93 for IOLMaster).
There was no difference in corneal diameters of left versus right eye with both calipers (p=0.09) and IOLMaster (p=0.86), assuming equal variances (F=2.33, p=0.13 for calipers; F=0.22, p=0.64 for IOLMaster).
Based on paired t-test comparison, measurements taken with calipers were an average of 0.1 mm larger than measurements taken by IOLMaster (p<0.001). Bland Altman analysis showed a mean difference of 0.09 mm and limits of agreement of -0.56 to +0.73 mm between WTW measured with calipers and IOLMaster (Figure 5).
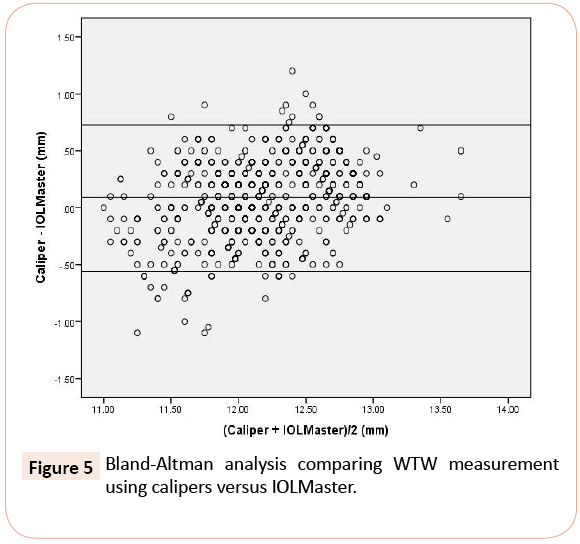
Figure 5: Bland-Altman analysis comparing WTW measurement using calipers versus IOLMaster.
Discussion
Current definitions of normal WTW are vague and inconsistent. The accepted general standard of normal horizontal WTW from >11.0 to <13.0 mm has not been established by evidence-based studies.
The measurement of the horizontal corneal diameter has clinical significance to the refractive cataract surgeon. Proper sizing of a traditional anterior chamber intraocular lens or a phakic anterior or posterior chamber intraocular lens depends upon this measurement, although the exact relationships between WTW, ATA and STS are still being evaluated. For the surgeon who performs astigmatic keratotomy for pre-existing astigmatism, the lasting effect of a corneal relaxing incision for a given optical zone depends upon the corneal diameter. For example, two corneal incisions placed at a 6 mm optical zone will have a far greater effect with a larger corneal diameter of 13 mm than a smaller corneal diameter of 11 mm. Moreover, visually judging the size of the capsulorhexis can be very deceptive in the eye with either a large or small corneal diameter. The surgeon may also need a greater amount of OVD to fill the anterior chamber when the corneal diameter is large. Even though a previous anatomic study failed to show a direct correlation between the corneal diameter and the size of the capsular bag [6], the surgeon must be cautious about implanting a toric lens in an eye that has a large anterior segment since rotation may occur within a large capsular bag.
The relationship between horizontal WTW and other measurements important for the refractive cataract surgeon have also been sought to be defined. Many surgeons add 0.50- 1.0 mm to the external corneal WTW measurement to determine the overall diameter for an anterior chamber phakic lens [12-14]. However, the relationship between external WTW and angle to angle (ATA) diameter has not been consistently determined. Several studies using various modalities of measurement have found that the ATA is larger than the WTW by 0.36 to 1.88 mm [13,15], while others have actually found significantly smaller ATA diameters than the WTW by 0.49 to 0.92 mm [16-18]. Best anterior chamber lens fit is paramount for the post-operative course, as improper sizing can result in corneal endothelial damage, iritis, glaucoma, and other complications. Additional studies have suggested that using an anterior chamber phakic lens diameter based on direct measurement of the ATA diameter with corneal and anterior segment OCT and very high frequency digital ultrasound may result in less sizing-related complications than when using estimates based on the WTW [18,19].
In 2005, the FDA approved an implantable posterior chamber phakic intraocular lens to correct myopia. The diameter of the posterior chamber phakic intraocular lens was determined by adding 0.5-1.0 mm to the external corneal WTW depending on the depth of the anterior chamber [20]. Since then, several studies have sought to further evaluate the relationship between WTW and sulcus-to-sulcus (STS) diameters. Two recent studies by Kawamorita, et al and Reinstein, et al found significantly larger STS diameters as compared to WTW of 0.41 mm and 0.89 mm, respectively [18,21]. However, several other studies have failed to find a statistically significant correlation between WTW and STS diameter [22-26]. It has also been suggested that direct measurement of the STS angle using ultrasound biomicroscopy and very high frequency digital ultrasound may be more reliable for determining overall posterior chamber phakic intraocular lens diameters than using measurements based on the WTW [21,18].
In this study, we have investigated the horizontal WTW corneal diameter using manual and automated measurement techniques. By definition, the normal range (mean ± 2 SD) should include approximately 95% of all values, and approximately 2.5% of values should fall 2-3 standard deviations above and below the mean. Our normal range as determined using calipers was 11.2 to 13.2 mm. Our study shows 12% of WTW values measuring 13.0 mm and larger with calipers, suggesting that corneas measuring at least 13.0 mm should be included within the normal range. Additionally, the extrapolated normal curve on the histogram shows an area under the curve that clearly includes values up to at least 13.2 mm. As for the lower limit of normal, we found 2% of WTW values measuring 11.0 mm and smaller with the calipers, which support the current definition of microcornea as measuring 11.0 mm and smaller. Additionally, our mean WTW obtained with calipers was 12.2 mm, which is larger than the currently accepted mean WTW of 12.0 mm (inferred from a normal range of 11.0- 13.0 mm). This suggests that the true upper limit of normal WTW may be shifted towards the right. Given our findings, it seems reasonable to consider expanding the upper limit of normal to include values up to 13.2 mm.
Mean WTW as obtained with IOLMaster was 0.1 mm smaller than mean WTW obtained with calipers. The current definition of normal WTW has been determined using calipers, as automated devices are newer technologies. In this study, only the results obtained with manual calipers are used for comparison with the currently accepted WTW normal range.
With respect to patient age, both the Rufer and Fu studies found a negative correlation between age and WTW. In our series, a significant correlation between age and WTW was not identified. With respect to patient gender, our results disclosed that males have slightly larger corneal diameters than females (0.08 mm with calipers; 0.15 mm with IOLMaster), which contrasts to the Fu study, which found significantly smaller corneal diameters in males and larger cornealdiameters in females. The Rufer study failed to demonstrate a correlation to gender. We did not find significant differences in mean WTW when comparing left and right eyes, which is consistent with previous studies [27,28].
This study has several weaknesses which are inherent in measuring the corneal diameter in the operating room. While it is generally accepted that the widest corneal diameter is at 180°, it is sometimes difficult to identify the horizontal meridian by inspection alone. Even if the surgeon can accurately locate the horizontal meridian, the variation in limbal anatomy can make the exact endpoint difficult to identify. For example, conjunctival degenerative changes or a posterior embryotoxin can produce an indistinct demarcation line. In addition, we were surprised to find that when the same cornea was measured with two different calipers, a 0.1 mm variation was not an uncommon finding. This is consistent with a small study published in 2013 by Mohamed, et al that concluded that the precision of manual calipers in ophthalmic biometry measurements is limited to 0.1 mm [29]. Still, the senior author had a track record of 35 years of measuring the corneal diameter in every case so his experience implies that the measurements were accurate. Finally, refractive error, previous corneal surgeries, and corneal abnormalities that may affect WTW measurements were not taken into account in this study [30].
In conclusion, this large series reveals that corneal diameters measuring 13.0 mm is more common than previously believed. In addition, IOLMaster produced WTW measurements that were slightly but significantly smaller than caliper WTW measurements, so these two devices should not be considered interchangeable when future population studies are conducted. Based on our results, we can consider expanding the upper limit of normal horizontal corneal WTW range to include values from >11.0 to ≤ 13.2 mm. This implies a definition of macrocornea as a WTW measuring larger than 13.2 mm. Our study supports the current definition of microcornea as WTW measuring 11.0 and smaller.
References
- Auffarth GU, Völcker HE (2000) [Cataract surgery in 79 patients with relative anterior microphthalmus (RAM): a review of anatomy, associated pathology and complications]. KlinMonblAugenheilkd 216: 369-376.
- Leibowitz, Howard M, et al. (1998) Corneal Disorders: Clinical Diagnosis and Management (2ndedn), Philadelphia: Saunders, pp. 204-206.
- Rapuano, Christopher, et al. (2000) Anterior Segment. St. Louis: Mosby, Inc. pp. 47-49.
- Smolin, Gilbert, et al. The Cornea. 3rd Ed. USA: 1994. Pages 538-539.
- Yanoff&Duker: Ophthalmology. 3rd ed. St Louis: Mosby, 2008. Chapter 4.3.
- Khng C, Osher RH (2008) Evaluation of the relationship between corneal diameter and lens diameter. J Cataract Refract Surg 34: 475-479.
- Albert DM (2008) Albert &Jakobiec’s Principles & Practice of Ophthalmology(3rdedn),Elsevier Inc.,Philadelphia.
- Arffa, Robert C (1997) Diseases of the Cornea (4thedn), St Louis: Mosby, p. 86.
- Rüfer F, Schröder A, Erb C (2005) White-to-white corneal diameter: normal values in healthy humans obtained with the Orbscan II topography system. Cornea 24: 259-261.
- Baumeister M, Terzi E, Ekici Y, Kohnen T (2004) Comparison of manual and automated methods to determine horizontal corneal diameter. J Cataract Refract Surg 30: 374-380.
- Fu T, Song YW, Chen ZQ, He JW, Qiao K, et al. (2015) Ocular biometry in the adult population in rural central China: a population-based, cross-sectional study. Int J Ophthalmol 8: 812-817.
- Friedman NJ, Khater TT, Koch DD (2005) Duane’s Clinical Ophthalmology. Chapter 8: Secondary Intraocular Lens Implantation,Lippincott Williams and WilkinsPhiladelphia.
- Kohnen T, Thomala MC, Cichocki M, Strenger A, Dipl-Ing (2006) Internal anterior chamber diameter using optical coherence tomography compared with white-to-white distance using automated measurements. J Cataract Refract Surg 32: 1809-1813.
- Lovisolo CF, Reinstein DZ (2005) Phakic intraocular lenses. SurvOphthalmol 50: 549-587.
- Wilczynski M, Bartela J, Synder A, Omulecki W (2010) Comparison of internal anterior chamber diameter measured with ultrabiomicroscopy with white-to-white distance measured using digital photography in aphakic eyes. Eur J Ophthalmol 20: 76-82.
- Nemeth G, Hassan Z, Szalai E, Berta A, Modis L Jr (2010) Comparative analysis of white-to-white and angle-to-angle distance measurements with partial coherence interferometry and optical coherence tomography. J Cataract Refract Surg 36: 1862-1866.
- Piñero DP, Plaza Puche AB, Alió JL (2008) Corneal diameter measurements by corneal topography and angle-to-angle measurements by optical coherence tomography: evaluation of equivalence. J Cataract Refract Surg 34: 126-131.
- Reinstein DZ, Archer TJ, Silverman RH, Rondeau MJ, Coleman DJ (2009) Correlation of anterior chamber angle and ciliary sulcus diameters with white-to-white corneal diameter in high myopes using artemis VHF digital ultrasound. J Refract Surg 25: 185-194.
- Goldsmith JA, Li Y, Chalita MR, Westphal V, Patil CA, et al. (2005) Anterior chamber width measurement by high-speed optical coherence tomography. Ophthalmology 112: 238-244.
- Sanders DR, Vukich JA, Doney K, Gaston M; Implantable Contact Lens in Treatment of Myopia Study Group (2003) U.S. Food and Drug Administration clinical trial of the Implantable Contact Lens for moderate to high myopia. Ophthalmology 110: 255-266.
- Kawamorita T, Uozato H, Kamiya K, Shimizu K (2010) Relationship between ciliary sulcus diameter and anterior chamber diameter and corneal diameter. J Cataract Refract Surg 36: 617-624.
- Fea AM, Annetta F, Cirillo S, Campanella D, De Giuseppe M, et al. (2005) Magnetic resonance imaging and Orbscan assessment of the anterior chamber. J Cataract Refract Surg 31: 1713-1718.
- Kim KH, Shin HH, Kim HM, Song JS (2008) Correlation between ciliary sulcus diameter measured by 35 MHz ultrasound biomicroscopy and other ocular measurements. J Cataract Refract Surg 34: 632-637.
- Oh J, Shin HH, Kim JH, Kim HM, Song JS (2007) Direct measurement of the ciliary sulcus diameter by 35-megahertz ultrasound biomicroscopy. Ophthalmology 114: 1685-1688.
- Pop M, Payette Y, Mansour M (2001) Predicting sulcus size using ocular measurements. J Cataract Refract Surg 27: 1033-1038.
- Werner L, Izak AM, Pandey SK, Apple DJ, Trivedi RH, et al. (2004) Correlation between different measurements within the eye relative to phakic intraocular lens implantation. J Cataract Refract Surg 30: 1982-1988.
- Zha Y, Feng W, Han X, Cai J (2013) Evaluation of myopic corneal diameter with the Orbscan II Topography System. Graefes Arch ClinExpOphthalmol 251: 537-541.
- Cakmak HB, Cagil N, Simavli H, Raza S (2012) Corneal white-to-white distance and mesopic pupil diameter. Int J Ophthalmol 5: 505-509.
- Mohamed A, Nankivil D, Pesala V, Taneja M (2013) The precision of ophthalmic biometry using calipers. Can J Ophthalmol 48: 506-511.
- Sanchis-Gimeno JA, Sanchez-Zuriaga D, Martinez-Soriano F (2012) White-to-white corneal diameter, pupil diameter, central corneal thickness and thinnest corneal thickness values of emmetropic subjects. SurgRadiolAnat34:167-170.

