Bijal M Shrivastava*, Siddharth Budhraja, Kunal Kumar Jaiswal and Abhinav Tiwari
Dr. L H Hiranandani Hospital, Mumbai, Maharashtra, India
Corresponding Author:
Bijal M Shrivastava
Dr. L H Hiranandani Hospital
Mumbai, Maharashtra, India
Received date: August 2, 2017; Accepted date: August 14, 2017; Published date: August 21, 2017
Citation: Shrivastava BM, Budhraja S, Jaiswal KK, Tiwari A (2017) Home Environmental Fungus - The Hidden Killer. J Prev Infect Cntrol. Vol.3 No.2:7.
Introduction
Interstitial lung disease (ILD) refers to a heterogeneous group of disorders, such as interstitial pneumonia, idiopathic pulmonary fibrosis, and hypersensitivity pneumonitis (HP), which affects the lung parenchyma and gas exchange. Interstitial lung disease (ILD) in children (chILD) is different in many aspects to the adult disease. The spectrum of conditions, in particular in infancy, is much wider than in adults. The conditions encompass growth and developmental issues, as well as immunological problems. Pulmonary involvement may be primary, as seen in pulmonary alveolar proteinosis, surfactant protein disorders, and hypersensitivity pneumonitis or secondary, as seen in systemic illnesses like connective tissue disorders, immunodeficiency and lymphoproliferative disorders.
Interstitial lung disease rarely presents as hypersensitivity pneumonitis in children. Hypersensitivity pneumonitis (HP) is an immune-mediated syndrome affecting pulmonary alveoli and interstitium, associated with repeated exposure to varied environmental antigens. Hypersensitivity pneumonitis (HP) is rare in children; primary allergic sources being exposure to pet birds (or feather in bedding) or homes contaminated with pigeons antigens. Molds from prior flooding or damp floors, humidifiers and hot tubs are other sources [1]. Presentation is usually nonspecific, symptoms includes cough, dyspnea, chest tightness, chills, malaise, fatigue; these can occur within 4-6 h or over several years after exposure to antigen [1]. Avoidance of the inciting antigens is the mainstay of treatment. Exposure to specific domestic indoor fungal spores is considered unlikely cause of Hypersensitivity pneumonitis [2], hence we are presenting our case.
Case Summary
4 year old female child initially was brought with complaints of repeated episodes of cough and cold for 6 months. At that time her investigation showed increased IgE levels and she was treated with anti-allergic (montelukast) for 6 weeks following which she showed some improvement. 1 year later she came with acute breathlessness at rest and productive cough on exertion. On examination she was found to have dyspnea at rest, SpO2<85% on room air, bilateral decreased air entry and crepitation. She was reinvestigated, complete blood cell count, 2D echocardiography and cystic fibrosis results were normal. HRCT Chest (Figure 1) was indicative of widespread intra/ centrilobular nodule distributed evenly in upper and lower lobe with intralobular septal thickening, patchy ground glasss oedema and traction bronchiectasis suggestive of Childhood Interstitial lung disease. A suggestive history was that child was clinically better away from home. Also there was history of pigeon dropping and feathers in home environment. To identify if any allergens in home environment would be responsible for her medical condition, a blood allergens test was done for pigeon and mold. Patient’s serum IgE was positive for Aspergillus fumigatus. To identify the source of Aspergillus fumigatus at homes fungal culture of air, sampling of AC duct and pillow cover was done, which was also positive for the same. With the diagnosis of childhood interstitial lung disease and allergens Aspergillus fumigatus identified as the cause, management consisted of treatment with intravenous methylprednisolone and long term oral steroids; along thorough cleaning up of home environment. At present child is 8 years old and asymptomatic with normal growth and development.
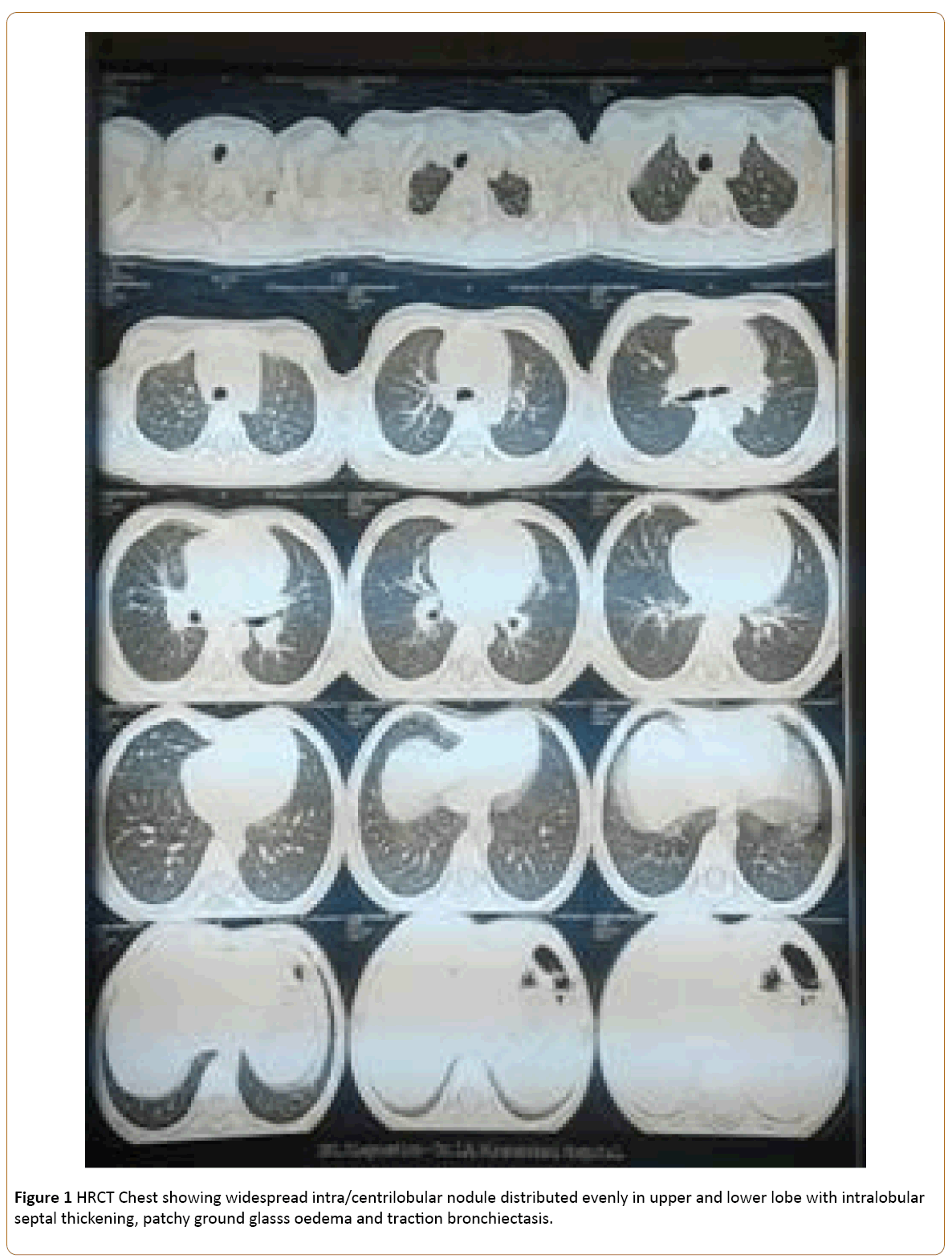
Figure 1: HRCT Chest showing widespread intra/centrilobular nodule distributed evenly in upper and lower lobe with intralobular septal thickening, patchy ground glasss oedema and traction bronchiectasis.
Discussion
Aspergillus fumigatus is one of the commonly detected fungal species in flooded indoor environment and in grain dust. Because of small size (2-3 μm in diameter) and hydrophobic nature, the spore may remain suspended in the air for long time, increasing the chances of deep inhalations into the alveolar spaces [3]. Exposure to Aspergillus fumigates spores is ubiquitous and causes spectrum of disease in susceptible hosts. Severe pulmonary disease associated is allergic bronchopulmonary aspergillosis, severe asthma with fungal sensitization, rhinitis, sinusitis and hypersensitivity pneumonitis as seen in our patient.
Aspergillus fumigatus induced pulmonary disease may or may not involve elevated serum IgE or fungal colonization [4-6]; luckily though both were positive in this child. Incidence of Interstitial lung disease is 30/100000 individual [7] of which that HP was less than 2%. Since 1960. 95 cases of HP in children have appeared in literature [8-10] of which mean age of onset was 10 years and youngest case reported had onset of symptoms at 8 months of age. 97% of children were treated with removal from exposure and 65% with corticosteroids therapy, which is known to induce long term remission; as is the case with our patient who is 8 year old now.
A history of worsening of symptoms on exposure to a potential agents and improvement in symptoms once the affected individual is away from that environmental space is essential for diagnosis and treatment. The interval between exposure to antigens and clinical feature of lung disease is unknown.
It’s known that if its low level of continuous exposure, then onset of symptoms of Hypersensitivity pneumonitis can be insidious as in our case. Our patient had repeated episodes of cold and coughs for 13 months; followed by an episode of acute breathlessness for which she was hospitalized. Her HRCT confirmed diagnosis of chronic hypersensitivity interstitial lung disease and her specific IgE to Aspergillus fumigatus was positive which was also grown from her home environment. Her dramatic clinical improvement away from home had helped us in identifying the source. The mainstay of treatment for HP is removal from the offending agent and treatment with glucocorticoids which fastens the pulmonary function normalization as in our patient.
References
- Nelson Textbook of Pediatrics, 20th Edition, pp: 2067-2069.
- Bush RK, Portnoy JM, Saxon A, Terr AI, Wood RA (2006) The medical effects of mold exposure. J Allergy Clin Immunol 117: 326-333.
- Cramer RA, Rivera A, Hohl TM (2011) Immune responses against Aspergillus fumigatus: What have we learned? Curr Opin Infect Dis 24: 315-322.
- Agarwal R (2011) Severe asthma with fungal sensitization. Curr Allergy Asthma Rep 11: 403-413.
- Knutsen AP, Bush RK, Demain JG, Denning D, Dixit A, et al. (2012) Fungi and allergic lower respiratory tract diseases. J Allergy Clin Immunol 129: 280-291.
- Agbetile J, Fairs A, Desai D, Hargadon A, Bourne M, et al. (2012) Isolation of filamentous fungi from sputum in asthma is associated with reduced post bronchodilator FEV1. Clin Exp Allergy 42: 782-791.
- Girard M, Lacasse Y, Cormier Y (2009) Hypersensitivity pneumonitis. Allergy 64: 322-334.
- Fan LL (2002) Hypersensitivity pneumonitis in children. Curr Opin Pediatr 14: 323-326.
- Fan LL, Kozinetz CA (1997) Factors influencing survival in children with chronic interstitial lung disease. Am J Respir Crit Care Med 156: 939-942.
- Ratjen F, Costabel U, Griese M, Paul K (2003) Bronchoalveolar lavage fluid in children with hypersensitivity pneumonitis. Eur Respir J 21: 144-148.

