Barick Uttam*, Vijay Kanth Anto, Gowda Arun, Mohanty Rituraj and Zomorodi Behsad
Focus Scientific Research Center, Part of Phamax Market Access Pvt. Ltd., KMJ Ascend, #19, 1st Cross, 17th C Main, Fifth Block, Koramangala, Bangalore, 560095, Karnataka, India
*Corresponding Author:
Uttam Barick
Focus Scientific Research Center, Part of Phamax Market Access Pvt. Ltd., KMJ Ascend, #19, 1st Cross
17th C Main, Fifth Block, Koramangala, Bangalore, 560095, Karnataka, India
Tel: 9741011822
E-mail: uttam.barick@phamax.ch
Received date: June 10, 2016; Accepted date: September 22, 2016; Published date: September 26, 2016
Citation: Uttam B, Anto VK, Arun G, et al. Evidence-Based Studies – Their Advantages and Disadvantages in the Data Collection Ecosystem. Insights in Biomed. 2016, 1:1.
Keywords
Real World Evidence (RWE); Data analytics; Big data in pharma
Contextual
Evidence-based research has now attained an important position in the biopharmaceutical product development and industry. Real World Evidence (RWE), a significant contributor to evidence based research, is a distinctive standard used to understand a drug’s cost-efficiency in the real world. It is instrumental in improving the quality of healthcare [1]. It is a means of broader information on the effectiveness and safety of a product. It also aids in directing the reimbursement policy and the further utilization of new products. Again, it drives stakeholders to better understand the impact of a new product in the real-world set-up. Thus, it has secured a concrete position in the early research and developmental phase [2].
Experts are of the opinion that ‘RWE’ should not be viewed as a business strategy. Rather, it is a part of the proof of concept that a pharmaceutical company carries out to demonstrate the realities of healthcare. It is also considered as the medical equivalent of ‘Big Data’ or ‘Big DIP’ (Big data in pharma) - the use of massive data sets to see how medicines perform outside the tightly corseted world of clinical trials. While Randomized Clinical Trials (RCTs) usually limit participation to selected patients, RWE looks at substantial blocks of information from patients of every type and band [3].
Argument
Recent developments in the RWE ecosystem in context of the drug development process
A new era of healthcare innovation could be realized by integrating various sources of patient data to generate insights. Real-world evidence and its utilization - outside of clinical trials - are seen as a way to tailor healthcare decision making more closely to the characteristics of individual patients. It is thus a step towards making healthcare additionally customized and more effective. RWE not only taps increasing volumes of data, but also weaves together different sources of data, such as clinical, socioeconomic and genomic data, to understand individual patient characteristics better and to improve medicine’s ability to cater to individual patient needs.
RWE challenges the traditional pattern in which evidence is generated through prospective randomized clinical trials [4]. Regulatory authorities require post-approval research or monitoring to determine real-world safety due to disquiet about a product's safety when it becomes broadly prescribed, while payers may require validation of a product's real-world clinical value and cost-effectiveness to decide optimal formulary placement. Data about real-world patient experience has the potential to improve the quality and delivery of medical care and it reduces overall costs and improves results by quickening the understanding of how best to incorporate new therapies and technologies into everyday clinical practice [2].
Real-world evidence is relevant in the product development as well as post product launch stages. The addition of real-world evidence to clinical trial evidence helps healthcare system stakeholders decide whether a specific treatment existing in the market should be given consent to, reimbursed, or reexamined. Real-world studies provide evidence of comparative safety and effectiveness. Prior to the launch of a new healthcare involvement, real-world studies can be conducted to define the market scenario, as well as the economic and patient burden of illness and existing treatment pathways [5]. Drug and device companies develop a more comprehensive image of what happens to patients over their treatment journey with RWE.
RWE provides the following important values to different stakeholders in the healthcare ecosystem:
1. Helps to understand the patient journey, treatment paths and effectiveness;
2. Builds a better understanding of disease patterns;
3. Arranges further safety data;
4. Enlightens the launch strategy and market access;
5. Demonstrates product value;
6. Maximizes possible return on investment;
7. Creates constant value across the product lifecycle and disease portfolios [6].
Technology as a means of innovations and opportunity – The positive and negative limits
Pharma can no longer ignore the interconnectivity or close bond between RWE and digital healthcare. Digital gadgets can economically and reliably collect information from patients and respond to it aptly. They can likewise encourage drug development and enhance responses to public health threats. The interest for RWE is expanding as resources for subsidizing medicinal services turn out to be more constrained. But, advances in technology offer great promise to reduce inefficiencies and support innovation and digital data acquisition. Technology can do more than just deliver services when combined with computational capabilities of modern analytics. Integration of Electronic Health Records (EHR) has been a major driver behind innovation in RWE [7].
The development of real world data generation, collection and analytics heavily relies on electronic systems and infrastructures. This has led to the term ‘eHealth’ - an umbrella term describing the use of such structures. e-Health depicts the 'utilization of Internet and other related advances in the healthcare industry to improve the access, efficiency, effectiveness, and quality of clinical and business processes used by healthcare organizations, practitioners, patients, and also consumers with an end goal to enhance the health status of patients. e-Health comprises institutional structures, data architecture systems, competence centers and legal frameworks. Competencies of eHealth authorities cover a range of e-Health instruments, including e-prescriptions, tele-health and patients’ electronic health records (EHRs) systems. An EHR is ‘the longitudinal electronic record of a patient that comprises or virtually links records together from multiple Electronic Medical Records (EMRs) which can then be shared across healthcare settings (interoperable). It aims to contain a history of contact with the healthcare framework for individual patients from numerous associations that convey care (Figure 1) [8,9].
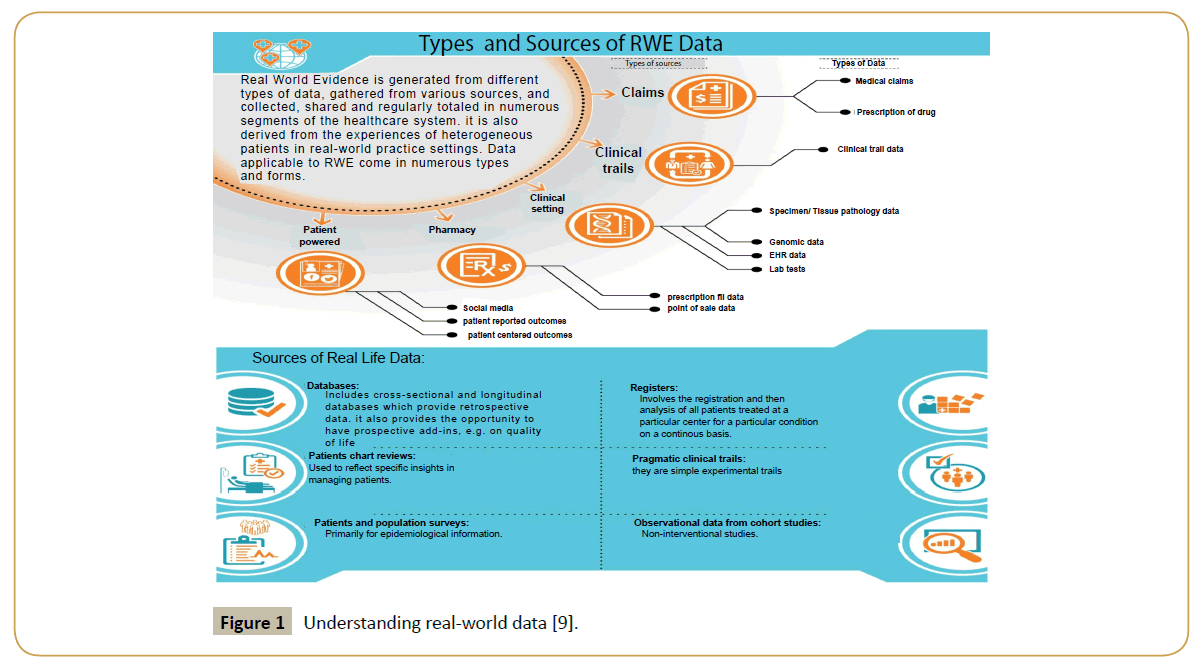
Figure 1 Understanding real-world data [9].
A major issue is a lack of a clear policy framework that suggests when and where RWE is useful. Hence it is imperative to get a clearer definition of RWE that can allow stakeholders from different organizations and groups to have a shared understanding of RWE [10]. Following are some of the real challenges that are experienced during the execution of a RWE project.
Lack of alignment within the stakeholders across geographies: RWE and its outcomes touch many different functions in pharmaceutical companies, across R&D, through medical affairs/ pharmacovigilance onto sales, marketing and market access. Conveying on all the above solutions accordingly requires the right expectation, destinations, individuals and structures set up hierarchically [11]. Patients, providers, and the public might be too far expelled from choices to use RWE to acknowledge its credentials to enhance the quality and efficiency of care. Thus, a deeper understanding of the value of RWE is required. Some contemporary RWE initiatives do not get meaningful participation by all stakeholders. Different stakeholders have different perspectives and they have different needs. There lies a lack of a ‘safe space’ for various stakeholders to come together and have open conversations about RWE that focuses on the issues around similar objectives. Thus, understating the diversity of stakeholders needs:
Continued change: In various markets, the public spotlight has moved to patient privacy. Changing and frequently conflicting, perspectives are being conveyed by privacy campaigners, suppliers, specialists and patient support foundations as they look to accomplish public confidence in the privacy of their information to understand the maximum capacity of healthcare information to change patient results [12].
Unclear regulatory landscape: Due to a great deal of recent developments in real world evidence, conventional regulatory models are becoming obsolete. Without a reasonable structure, market participants must tread carefully amongst different regulators and decision makers (e.g. those responsible for ethics, patients’ privacy and pharmacovigilance) [12]. The current regulatory framework and limited access to generate high-quality real world data is a primary challenge [13].
Scope of improvement on data linkage for real world data: There is still a need to utilize common healthcare information technology (IT) data structures and terminologies for better linkage and examination so that RWE can become more useful in making healthcare decisions [10] The greatest challenge in using real world data is that it is not always available and in the desired form when needed [14]. Thus, there is a huge space for scope of improvement in the art of state for real time analytics.
Time: Conventionally, evidence based studies have been restricted to the post-launch phase of a drug to be able to demonstrate the real world effectiveness of a drug. However, based on the application of data from well-designed evidence based studies, these can be conducted and the data leveraged across various stages of a product development life-cycle. In the pre-clinical phase, the studies could be leveraged for understanding the disease management scenario and natural progression of disease in hitherto understudied disease areas like rare diseases. Evidence generated will be useful inputs to R&D teams for designing clinical studies and understand the need-gaps. In early stage of clinical research, parallel evidence based study can help determine the right patient population for the candidate drug in late-stage research. Immediately post-launch evidence based studies can be leveraged for health technology assessment and demonstrating cost-benefit. Towards the lag phase of a product cycle, these studies help to determine differentiators and identifying uses beyond those demonstrated or tested in the RCT environment [15].
Cost: While the cost of gathering and keeping information might be an established cost of doing business for manufacturers (clinical trial and outcomes data) and payers (claims data), financial models for data maintained by other stakeholders (patient groups, professional societies, providers) are much less certain, particularly to the extent they rely on government funding [4]. Many stakeholders collect and maintain data as a normal part of their business strategies. Health plans collect and store claims data, and manufacturers do the same with clinical trial and outcomes data. Other groups (e.g. patient groups) do not necessarily do this as part of their business model, and funding to maintain their efforts can be difficult to get [16].
If pharmaceutical companies fail to build an effective RWE-based capabilities system, they are at risk of rapidly losing control over the worth of the communication around their own drugs, as other stakeholders such as payers, data analytics companies, and academia are as of now upgrading their own capabilities. Consequently, use and reimbursement may significantly decline [13].
Data quality: In this new world of RWE, there is a large variety of data that needs to be collected and analyzed. Specifically, semistructured and unstructured data, some of it originating from the patients and their social networks, make an impressive challenge for Data Scientists. Complex data types (i.e. video and images) yield large volumes of data to be analyzed. However, it is not the measure of data fundamentally that makes the challenge. The true challenge is analyzing unstructured and semi-structured data, and doing it in a way that yields scientifically important bits of knowledge [17]. Data collection in RWE is not meant for use in research many a times. Often, researchers have to clean the data for it to be usable [16].
A number of challenges to maximizing the potential of real world evidence remain, most notably a lack of clarity in its role in regulatory and Health Technology Assessment (HTA) decision- making. Regulators and HTA bodies need to throw more light on the prominence of real world evidence (e.g. around different data sources, applications of real world evidence), with better arrangement and cooperation between the regulatory and HTA requirements [18].
The challenge lies in using routinely collected data (data rarely collected for the purpose of clinical study) that is cleansed and formatted - or, a “data janitor” - to make it useful for research. There are challenges like patient consent and privacy, issues of transparency and replication, unsystematic regulation of RWE studies etc. [19].
Bottom-line benefits of RWE
Real world evidence increases efficiency in R&D and bridges the gap between the proof of adequacy required to pass regulatory scrutiny and the demonstration of likely effectiveness needed to satisfy health technology assessment bodies [20]. RWE can:
Research the effectiveness of interventions or practice: This could be used to inform the modeling of clinical and/or cost effectiveness as part of guidance production. Real-world data can also help to resolve uncertainties identified in existing NICE guidance
Audit the implementation of guidance: For example, to assess the equity of implementation across different groups (including socioeconomic, geographic, demographic and groups differentiated by different diseases/health conditions); this may also form part of performance monitoring systems
Provide information on resource use and evaluate the potential impact of guidance.
Provide epidemiologic information: For example, prevalence/ incidence of diseases, natural history, co-morbidities and information on current practice [21]
Conclusion
Despite the evident benefits of evidence-based studies and their increasing acceptance in decision making, challenges are present. The lack of a well-designed scientific study could potentially lead to non-acceptance of the data reducing the generalizability of results. Concerns in terms of ethical considerations and investigators’ lack of confidence prevail as well. But with cost, both for treatment and the conduct of studies, becoming increasingly prohibitive, evidence-based studies could form a useful and relatively economic tool. These studies will soon be able to allay the concerns of regulatory bodies and physician community with the right timing and outcomes based on quality data. The evolution of technology will enable patients and caregivers the freedom to track and report their health status as well as outcomes, fast-tracking evidence-based studies focused on patient outcomes into being accepted as mainstream research. The potential of evidence-based studies becomes more attractive considering the data sources from where these can be derived. In the emerging world, there is an oft-repeated concern about the lack of locally relevant research and evidence. The ability to leverage existing patient records and other forms of survey data could be a way of hastening the arrival of informed decisionmaking in these countries as well.
Acknowledgement
The authors would like to acknowledge the efforts of Nidish Narayanan, Senior Editor at phamax for his invaluable support in the development of this article.
Conflict of Interest
The authors declare that there are no conflicts of interests regarding the publication of this paper.
References
- Saha YK, Pateria D (2015) Real-world evidence: A better life journey for pharmas, payers and patients.
- https://www.appliedclinicaltrialsonline.com/real-world-evidence-studies.
- Durand M (2013) Why health care companies are turning to real-world evidence and what it means for communicators.
- Hubbard E, Paradis R (2016) Real world evidence: A new era for health care innovation.
- Parmenter Lvan-Engen A (2016) HTA and market insights real-world evidence generation for evolving stakeholder needs.
- https://www.medpace.com/PDF/Articles/Get-real-demonstrating-effectiveness-RWE.pdf
- Fimińska Z (2015) Real world evidence: Maximize benefits to healthcare, thought leadership and innovation for the pharmaceutical industry – Eye for pharma.
- Miani C, Robin E, Horvath V, Manville C, Cave J, et al. (2014) Health and healthcare: Assessing the real-world data policy landscape in Europe.
- Annemans L, Aristides M, Kubin M (2007) Real-life data: A growing need. International Society for Pharmaco-economics and Outcomes.
- Nason E, Husereau D (2014) Roundtable on real world evidence system readiness – Are we ready to use routinely collected data to improve health system performance? Institute on Health Economics.
- https://www.adelphicommunications.com/news/article-detail.aspx?id=7
- Ronte H, Foxcroft R (2016) Real world evidence enabling the life science industry to transform patient care.
- Rönicke D, Ruhl D, Solbach D (2016) Revitalizing pharmaceutical R&D and the value of real world evidence.
- https://www.parexel.com/files/5514/5639/9299/RWEDataStrat_Article_021916.pdf.
- https://www.sas.com/content/dam/SAS/en_us/doc/solutionbrief/life-sciences-real-world-data-107697.pdf.
- https://www2.deloitte.com/us/en/pages/life-sciences-and-health-care/articles/health-care-current-october6-2015.html.
- Murphy A (2015) Overcoming real challenges in real world evidence adoption. Saama technologies.
- https://www.acmedsci.ac.uk/viewFile/56cab22108cf9.pdf.
- https://catalyst.phrma.org/real-world-evidence-not-just-big-data.
- https://efpiamapps.eu/get-real-using-real-world-data-for-decision-making-in-R&D-and-health-technology-assessment/
- Toussi M (2015) Realizing the potential of Real World Evidence. IMS health.

