Keywords
64-Slice computed tomography (64-Slice CT); Coronary arterial fistulae (CAFs); Conventional coronary angiography (CAG); Clinical presentation; Residual fistula
Introduction
Coronary artery fistulae (CAFs) are unusual congenital or acquired coronary artery abnormalities in which blood is shunted into a cardiac chamber, great vessel, or other structure, bypassing the myocardial capillary network. They are the most common congenital coronary anomalies affecting hemodynamic parameters [1]. Surgical correction is indicated for most patients with CAFs; the correct diagnosis and precise evaluation of CAFs are important for determining the treatment plan.
Coronary angiography (CAG) is, at present, the conventional method for the evaluation and diagnosis of CAFs; however, when complex anatomy of a CAFs is expected, especially in the more rare complex cases with a dual origin or giant coronary artery [2], CAG may not be the appropriate test, because this procedure is invasive and has difficulty in delineating or displaying the previous course of the anomalous vessel due to its complex three-dimensional geometry that is fluoroscopically displayed in two dimensions [3]. The ideal investigative technique should be noninvasive, and provide an exact anatomic description of the fistula. The recently developed noninvasive 64-slice CT allows accurate depiction of the origin, course, and termination of CAFs. Sixty-four-slice CT is superior to conventional angiography for delineating the ostial origin, the proximal path of the anomalous coronary arteries, and the drainage site of CAFs [4,5]. Sixty-fourslice CT would be more useful than conventional angiography for evaluating complex CAFs by more exactly displaying the complex vascular relationships with three dimensional and multiplanar reformations. The frequency of incidentally detected CAFs on cardiac 64-Slice CT in the adult population has increased due to the increased use of 64-Slice CT for the evaluation of ischemic heart disease. Therefore, meticulous interpretation of the complex images is essential in CAFs, especially with 64-Slice CT. This technique will help to make the correct diagnosis and guide management. In addition, and it may also improve the outcome in patients with CAFs.
This study has two purposes. First, we wish to summarize the clinical data, to delineate some pathophysiology of CAFs, and to identify clinical features suggestive of the diagnosis of CAFs. Second, we would like to illustrate the 64-Slice CT findings of various types of CAFs.
Materials and Methods
Clinical data
We retrospectively reviewed all patients with congenital coronary artery fistula diagnosed in our hospital from April 2009 to October 2016. This retrospective observational study did not require approval of the institutional review board according to the policy of our hospital. There were 19 patients (eight males and 11 females) screened by CTA, 11 of whom (eight males and three females, mean age: 38 ± 24 yrs; range: 10m to 74 yrs) were confirmed by surgery or CAG to have CAFs. CAF is a condition with protean manifestations. In our study, half of the patients are symptomatic after the age of thirty years. Their symptoms or clinical complications range from trivial to lethal. Seven patients in our study experienced chest tightness or angina pectoris, and in three patients, CAFs manifested as recurrent pneumonia; one patient was asymptomatic.
Methods
A 64-slice CT was used for all patients (64 slice spiral CT scanner PHILPS) with 64 detector rows. The individual detector collimation was 64 × 0.5 mm. Effective pitch was 0.175 or 0.225. The rotation time was 0.4–0.45 s. A tube voltage of 120 kV and an effective tube current of 100400 mA were used. Scan range was from the root of the aorta to 5 cm infra-diaphragmatic. Manual trigger or Sure-star technique was used according to the experience of the cardiologist. The trigger point was set when the root of aorta reached a predefined threshold of 150 or 200 Hounsfield units (HU). The scan times ranged from 810 to 820 seconds depending on the patient. Breath-holding technique was applied to all the patients, but for the patients who could not cooperate, 10% chloral hydrate was applied at a dose of 0.5 mL/kg around 30 minutes before scanning, and the scan was performed without breath-holding. Oral β-blocker (propranolol HCl) was used to control the heart rate at a dose of 1–2 mg/kg 30 minutes to 1 hour before examination by 64-slice CT. The electrocardiogram was recorded simultaneously to allow retrospective gating of the data. The scanning direction was head-to-foot. A 60–75 ml dose of nonionic contrast medium (Iopromide 370 mg/ml) was injected at the rate of 4.0–5.0 ml/s into the antecubital vein followed by 40 mL of saline flush. During imaging construction, retrospective electrocardiographic gating was applied, and images were routinely reconstructed using a 0.5 mm slice thickness and 0.3 mm slice increment during the optimal phase (the phase with the least motion artifact).
All data were transferred to the workstation (Vitrea@2 version 3.7.0). Various methods such as multiplanar reformations (MPR), maximum intensity projections (MIP), curved planar reformation (CPR), and volume rendering technique (VR) were used to demonstrate the anatomy of the coronary arteries, the chambers of the heart, and the great vessels.
Results
We classified CAFs into the following two types: Type 1 (CVFs), in which the fistula terminates in a thoracic vessel [pulmonary artery (PA), superior vena cava (SVC), pulmonary veins (PV), bronchial and cardiac veins, and right ventricular outflow tract (RVOT)]; and Type 2 (CCFs), in which the fistula terminates in a cardiac chamber [right atrium (RA), coronary sinus (CS), right ventricle (RV), left atrium (LA), or left ventricle (LV)] [6].
Coronary artery fistula terminates in a thoracic vessel (CVFs).
Over 90% of these fistulae drain into the venous circulation. Lowpressure structures are the most common sites of drainage of the coronary fistulae. These include the pulmonary artery, superior vena cava, coronary sinus, and right-sided chambers [7].
Coronary-artery-to-pulmonary-artery-fistula
In total, four of our patients had a fistula of a coronary artery to the pulmonary artery. There have been a few reported cases of successful 64-slice CT evaluation of complex CAFs arising from two different feeding arteries [8-12]. Especially in such cases with a dual origin, CAG has limitations in the evaluation of CAF because of the complex configuration of anomalous vessels. Their anatomical relationship with adjacent structures may be obscured on two-dimensional fluoroscopic imaging; however, the three-dimensional volume-rendered images provide an excellent depiction of the tortuous course of the fistula, the anatomic relationships between the fistulous communications, aorta, pulmonary arteries and heart, and other malformations (Figure 1). One patient had a large aneurysm in association with a fistulous connection between the LAD and the PA (Figure 2). Another patient had many tortuous anomalous vessels arising from one of the left coronary arteries (LM, LAD, LCx) communicating with the PA (Figure 3). One of our patients had a more common type of anomaly, in which the lumen of LCA and the LCx was obviously dilated, extending to the fistula (Figure 4). Clinical characteristic of patients with coronary-arteryto- pulmonary-artery fistula (Table 1).
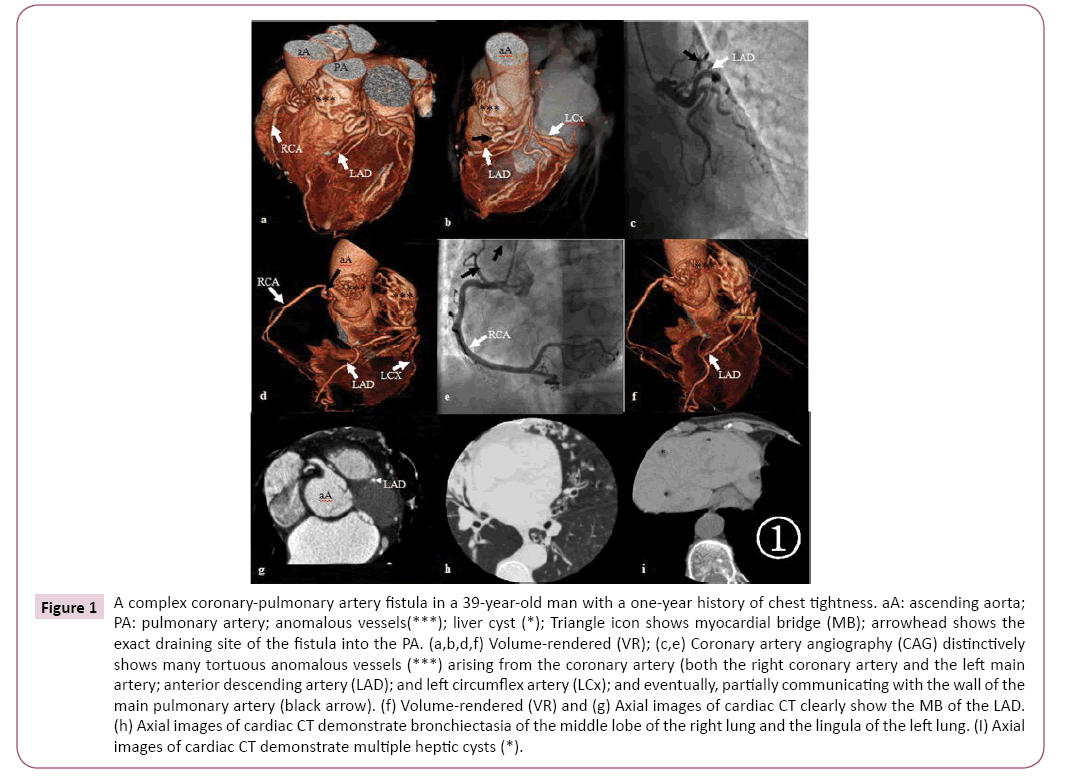
Figure 1: A complex coronary-pulmonary artery fistula in a 39-year-old man with a one-year history of chest tightness. aA: ascending aorta; PA: pulmonary artery; anomalous vessels(***); liver cyst (*); Triangle icon shows myocardial bridge (MB); arrowhead shows the exact draining site of the fistula into the PA. (a,b,d,f) Volume-rendered (VR); (c,e) Coronary artery angiography (CAG) distinctively shows many tortuous anomalous vessels (***) arising from the coronary artery (both the right coronary artery and the left main artery; anterior descending artery (LAD); and left circumflex artery (LCx); and eventually, partially communicating with the wall of the main pulmonary artery (black arrow). (f) Volume-rendered (VR) and (g) Axial images of cardiac CT clearly show the MB of the LAD. (h) Axial images of cardiac CT demonstrate bronchiectasia of the middle lobe of the right lung and the lingula of the left lung. (I) Axial images of cardiac CT demonstrate multiple heptic cysts (*).
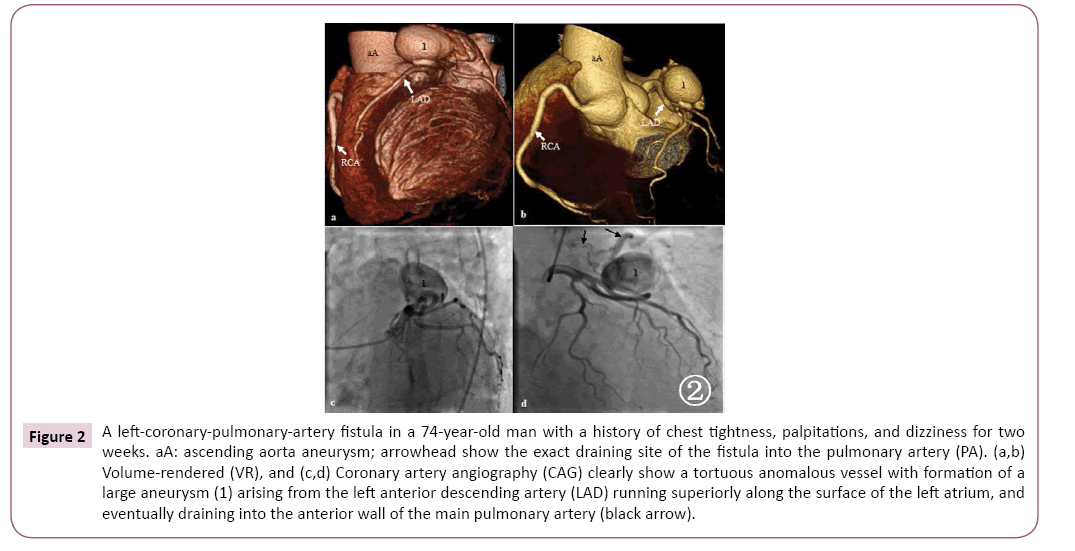
Figure 2: A left-coronary-pulmonary-artery fistula in a 74-year-old man with a history of chest tightness, palpitations, and dizziness for two weeks. aA: ascending aorta aneurysm; arrowhead show the exact draining site of the fistula into the pulmonary artery (PA). (a,b) Volume-rendered (VR), and (c,d) Coronary artery angiography (CAG) clearly show a tortuous anomalous vessel with formation of a large aneurysm (1) arising from the left anterior descending artery (LAD) running superiorly along the surface of the left atrium, and eventually draining into the anterior wall of the main pulmonary artery (black arrow).
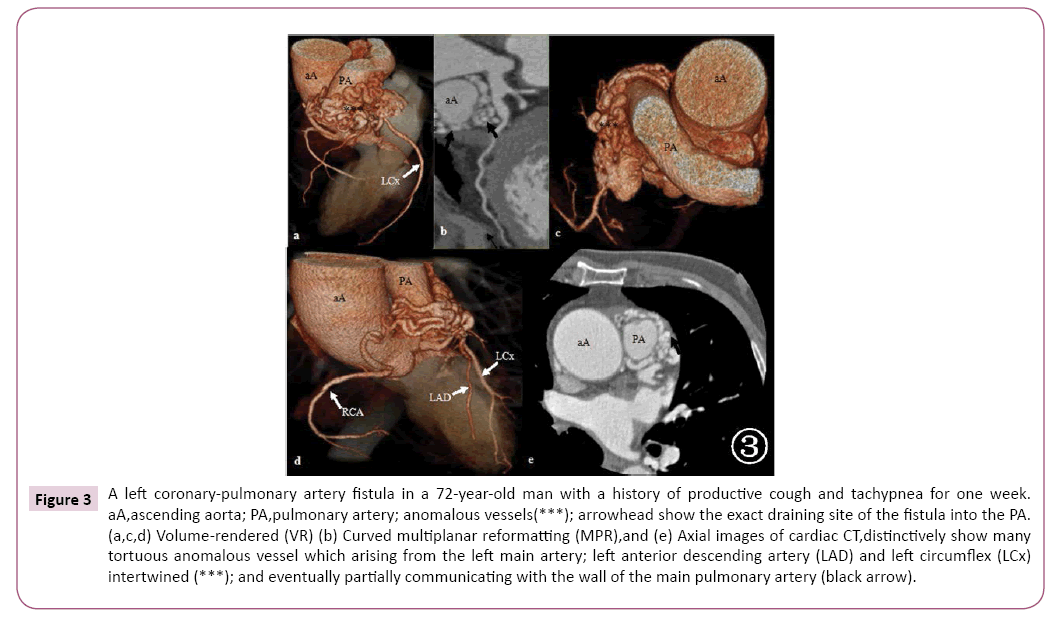
Figure 3: A left coronary-pulmonary artery fistula in a 72-year-old man with a history of productive cough and tachypnea for one week. aA,ascending aorta; PA,pulmonary artery; anomalous vessels(***); arrowhead show the exact draining site of the fistula into the PA. (a,c,d) Volume-rendered (VR) (b) Curved multiplanar reformatting (MPR),and (e) Axial images of cardiac CT,distinctively show many tortuous anomalous vessel which arising from the left main artery; left anterior descending artery (LAD) and left circumflex (LCx) intertwined (***); and eventually partially communicating with the wall of the main pulmonary artery (black arrow).
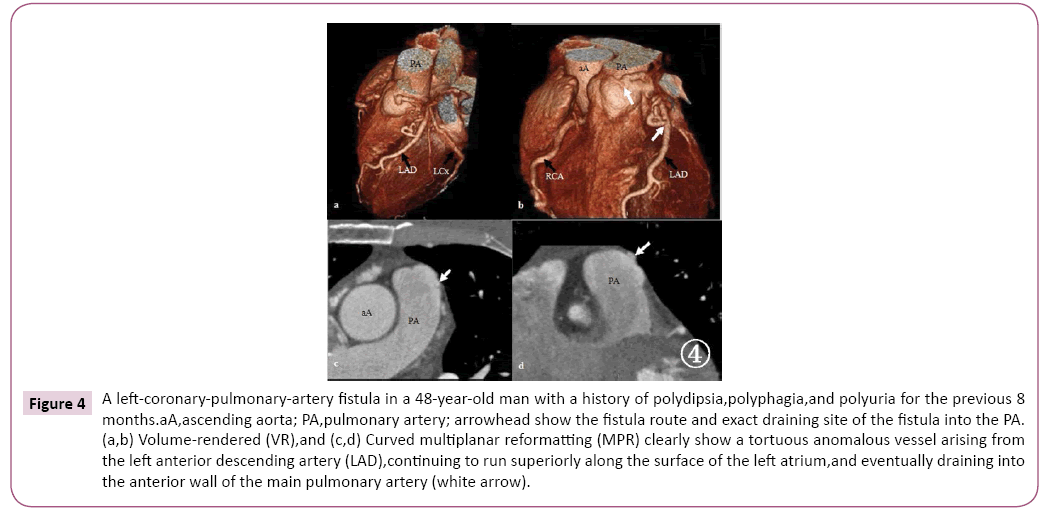
Figure 4: A left-coronary-pulmonary-artery fistula in a 48-year-old man with a history of polydipsia,polyphagia,and polyuria for the previous 8 months.aA,ascending aorta; PA,pulmonary artery; arrowhead show the fistula route and exact draining site of the fistula into the PA. (a,b) Volume-rendered (VR),and (c,d) Curved multiplanar reformatting (MPR) clearly show a tortuous anomalous vessel arising from the left anterior descending artery (LAD),continuing to run superiorly along the surface of the left atrium,and eventually draining into the anterior wall of the main pulmonary artery (white arrow).
Table 1 Clinical data from patients with coronary-artery-to-pulmonary-artery fistula.
| Case/age /gender |
Cardiac murmur |
Clinical presentation |
Comorbidities |
Electrocardiogram |
Management |
| 1. 39 y Male |
Normal |
Chest tightness after intense activity |
Myocardial bridge |
Biphasic T waves (V3–V6) |
b |
| 2. 74 y Male |
Normal |
Chest tightness |
Nasopharyngeal carcinoma,fibrosarcoma |
S-T segment depression and T wave inversion across the precordium |
b |
| Palpitations |
| Dizziness |
| 3. 72 y Male |
Continuous machinery cardiac murmur 5th intercostal space |
Productive cough |
Atherosclerosis |
a |
b |
| Tachypnea |
Aortic aneurysm |
| 4 .48 y Male |
Normal |
Polydipsia,polyphagia,polyuria |
Diabetes mellitus |
ST-T segment changes |
b |
Prior to surgery, we misdiagnosed two first-diagonal-artery-toright- ventricular-outflow-tract (RVOT) fistulas as a left-coronarypulmonary- artery fistula (Figure 5), and a right-coronary-arteryto- superior-vena-cava fistula (Table 2).
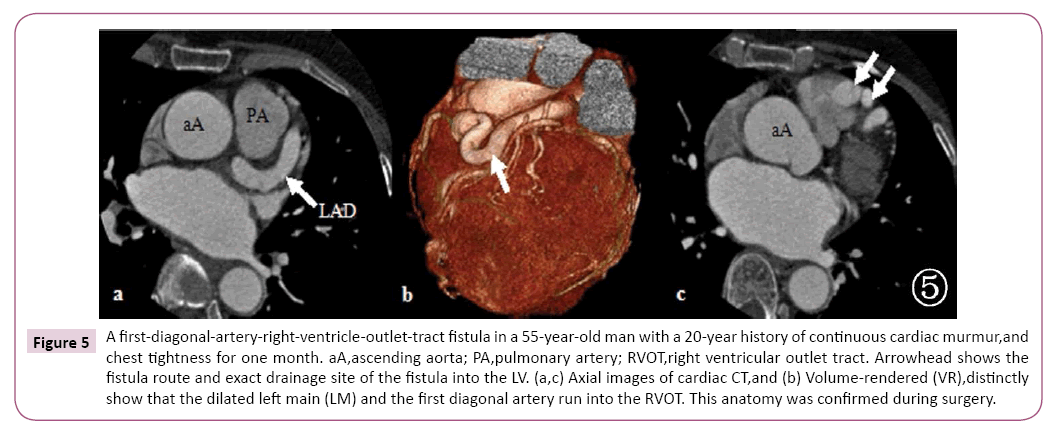
Figure 5: A first-diagonal-artery-right-ventricle-outlet-tract fistula in a 55-year-old man with a 20-year history of continuous cardiac murmur,and chest tightness for one month. aA,ascending aorta; PA,pulmonary artery; RVOT,right ventricular outlet tract. Arrowhead shows the fistula route and exact drainage site of the fistula into the LV. (a,c) Axial images of cardiac CT,and (b) Volume-rendered (VR),distinctly show that the dilated left main (LM) and the first diagonal artery run into the RVOT. This anatomy was confirmed during surgery.
Table 2 Clinical data from two misdiagnosed patients.
| Case/age /gender |
Cardiac murmur |
Clinical presentation |
Comorbidity |
Electrocardiogram |
Management |
Post-operation |
| 1. 55 y Female |
grade 3/4 continuous cardiac murmur in L3/4 |
Chest tightness |
Congenital abnormality of the aortic valve |
Left ventricular high voltage |
Surgery |
Without Residual fistula |
| Dyspnea |
| Palpitations |
ST-T segment changes |
| Edema of the lower extremities |
| 2. 29 y Female |
continuous cardiac murmur at the left or right sternal border |
Recurrent URI |
None |
Left vetricular high voltage |
Surgery |
Without Residual fistula |
| Chest tightness and |
Short P-R interval |
| Chest pain when tire |
URI: upper respiratory infections
The fistula terminates into a cardiac chamber (CCFs)
Coronary-artery-to-left-ventricle fistulae (Figure 6) are exceedingly rare, and they account for about 2–3% of all CAFs [13]. Coronary-artery-cardiac-chamber fistulae are thought to be the result of an abnormality during the embryonic development of the coronary circulatory system. When the intramyocardial trabecular sinusoids, which normally become narrow and persist only as The besian vessels in adults, are not obliterated, a fistulous communication persists between the coronary arteries and a cardiac chamber [13]. They are the most common congenital coronary anomalies that affect the hemodynamic parameters [14]. In previous studies, the drainage site of a coronary artery to a left ventricular fistula, as assessed with 64-slice CT, was the posteroinferior wall of the left ventricle [15]. This type of CAF was observed in two of the eleven patients. The right ventricle is known to be the most common drainage site of CAFs [13]. We had two cases of coronary-artery-to-right-ventricle fistula in our study (Figures 7 and 8). There also was one case of left-coronaryartery– to-right atrium fistula (Figure 9). Clinical characteristics of patients with a fistula terminating in a cardiac chamber (CCFs) (Table 3).
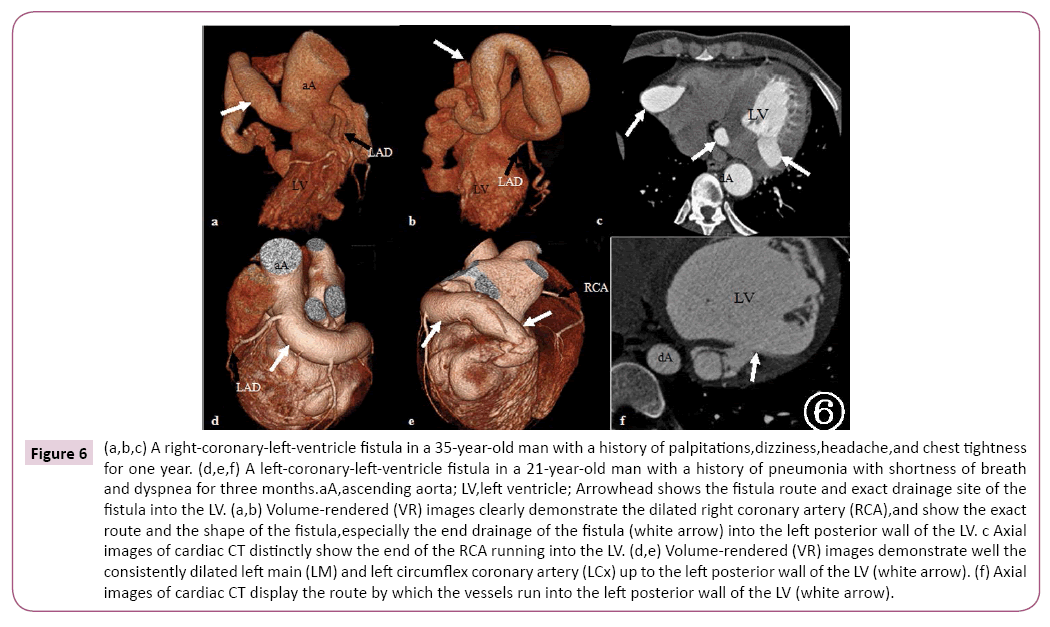
Figure 6: (a,b,c) A right-coronary-left-ventricle fistula in a 35-year-old man with a history of palpitations,dizziness,headache,and chest tightness for one year. (d,e,f) A left-coronary-left-ventricle fistula in a 21-year-old man with a history of pneumonia with shortness of breath and dyspnea for three months.aA,ascending aorta; LV,left ventricle; Arrowhead shows the fistula route and exact drainage site of the fistula into the LV. (a,b) Volume-rendered (VR) images clearly demonstrate the dilated right coronary artery (RCA),and show the exact route and the shape of the fistula,especially the end drainage of the fistula (white arrow) into the left posterior wall of the LV. c Axial images of cardiac CT distinctly show the end of the RCA running into the LV. (d,e) Volume-rendered (VR) images demonstrate well the consistently dilated left main (LM) and left circumflex coronary artery (LCx) up to the left posterior wall of the LV (white arrow). (f) Axial images of cardiac CT display the route by which the vessels run into the left posterior wall of the LV (white arrow).
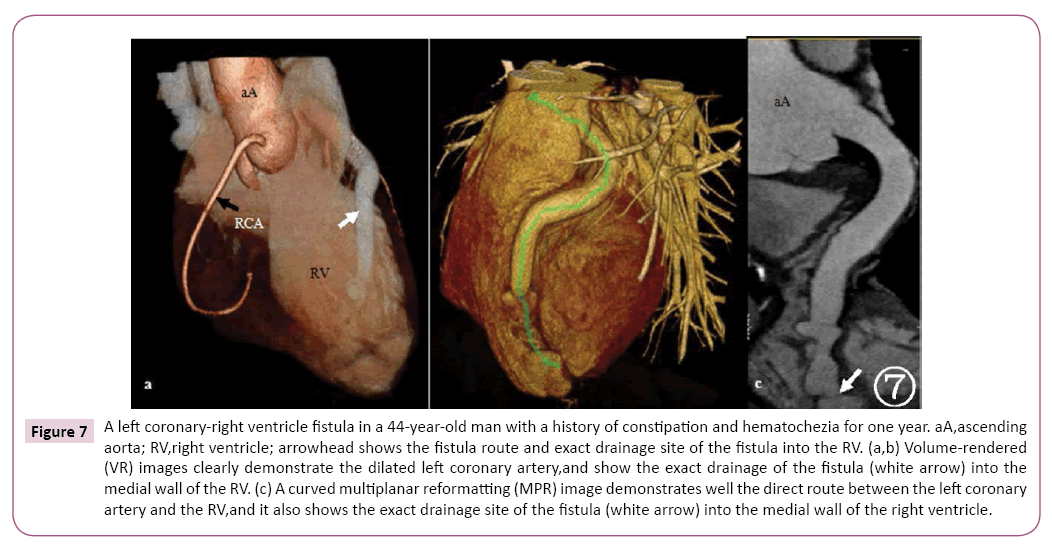
Figure 7: A left coronary-right ventricle fistula in a 44-year-old man with a history of constipation and hematochezia for one year. aA,ascending aorta; RV,right ventricle; arrowhead shows the fistula route and exact drainage site of the fistula into the RV. (a,b) Volume-rendered (VR) images clearly demonstrate the dilated left coronary artery,and show the exact drainage of the fistula (white arrow) into the medial wall of the RV. (c) A curved multiplanar reformatting (MPR) image demonstrates well the direct route between the left coronary artery and the RV,and it also shows the exact drainage site of the fistula (white arrow) into the medial wall of the right ventricle.
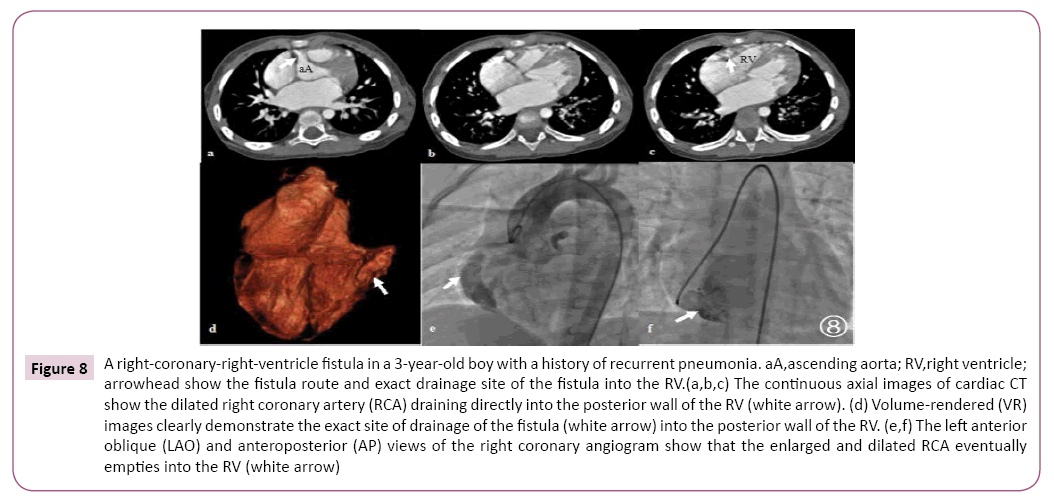
Figure 8: A right-coronary-right-ventricle fistula in a 3-year-old boy with a history of recurrent pneumonia. aA,ascending aorta; RV,right ventricle; arrowhead show the fistula route and exact drainage site of the fistula into the RV.(a,b,c) The continuous axial images of cardiac CT show the dilated right coronary artery (RCA) draining directly into the posterior wall of the RV (white arrow). (d) Volume-rendered (VR) images clearly demonstrate the exact site of drainage of the fistula (white arrow) into the posterior wall of the RV. (e,f) The left anterior oblique (LAO) and anteroposterior (AP) views of the right coronary angiogram show that the enlarged and dilated RCA eventually empties into the RV (white arrow)
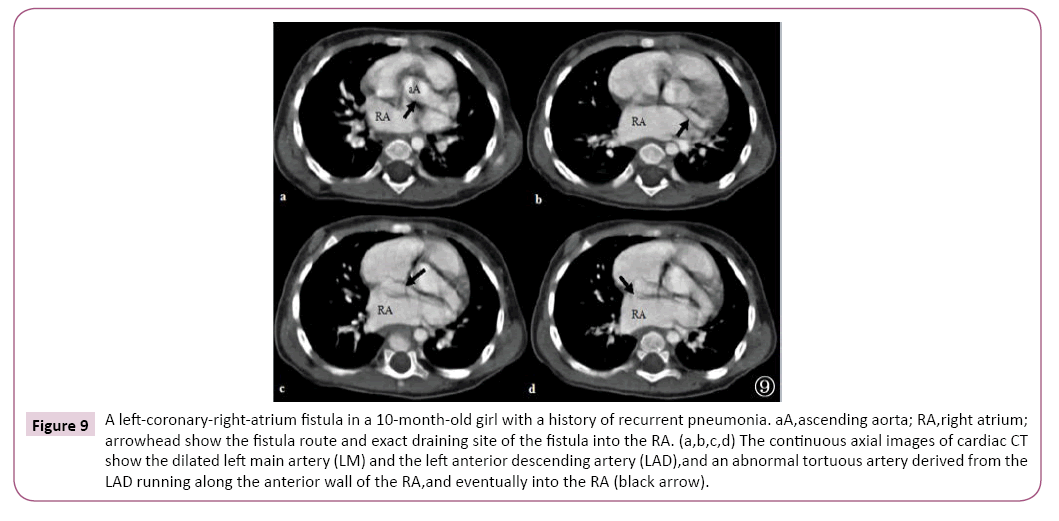
Figure 9: A left-coronary-right-atrium fistula in a 10-month-old girl with a history of recurrent pneumonia. aA,ascending aorta; RA,right atrium; arrowhead show the fistula route and exact draining site of the fistula into the RA. (a,b,c,d) The continuous axial images of cardiac CT show the dilated left main artery (LM) and the left anterior descending artery (LAD),and an abnormal tortuous artery derived from the LAD running along the anterior wall of the RA,and eventually into the RA (black arrow).
Table 3 Clinical characteristics of patients with a fistula terminating in a cardiac chamber.
| Case/age/gender |
Cardiac murmur |
Clinical presentation |
Comorbidity |
Electrocardiogram |
Management |
Postoperative |
| 1 10 m Female |
Grade 3/6 SM cardiac murmur left sternal border 2nd intercostal space |
Recurrent pneumonia |
Aberrant right subclavian artery(ARSA) |
Normal |
b |
# |
| 2 3 y Male |
Continuous cardiac murmur at the left sternal border,4th intercostal space; |
Recurrent pneumonia |
None |
a |
Surgery |
Residual fistula |
| 3 21 y Male |
Grade 3–4/6 DM sighing sound in apical area (mitral valve) |
Pneumonia with shortness of breath |
None |
S-T segment |
Surgery |
Residual fistula |
| Dyspnea |
depression and T-wave inversion across the precordium |
| Chest tightness |
| 4 35 y Male |
Grade 3/6 DM cardiac murmur at left sternal border,3rd intercostal space; |
Palpitations |
None |
Left vetricular high voltage |
Surgery |
Residual fistula |
| Dizziness |
| Grade 2/6 DM sighing sound over mitral valve |
Headache |
| Chest tightness |
Arrhythmia |
| Thrill |
Tachypnea |
| 5 44 y Male |
Normal |
Hematochezia |
Rectal cancer |
Normal |
Surgery for rectal cancer |
# |
| Constipation |
Discussion
Clinical presentation
Clinical presentation varies according to etiology, age, and duration of the shunt. In congenital CAFs, around 20% of patients are symptomatic in the first two decades, which increases to 60% after the age of twenty years [16]. This observation was in accord with our study. Only two patients (18%), had clinical symptoms at <20 years of age. We divided all of our patients into three groups, according to the age of the patient, and designated A (age >30 y), B (20 y(Table 4). We found that the patients in group A mainly manifested chest tightness (57%). Recurrent pneumonia was the dominant clinical manifestation of group C, and group B had recurrent upper respiratory infections or pneumonia, chest tightness, or chest pain when tired. Based on these observations, we assume that children experience recurrent pneumonia. The young may manifest pneumonia and exercise-induced angina. Adults over age 30 are likely to present with chest tightness, shortness of breath, fatigue, exercise intolerance that worsens with shunt augmentation, and progressive enlargement of the fistula. No patient under 30 years of age had fistula-related complications, and all older patients (>30 y of age) had complications, including electrocardiographic findings of myocardial ischemia – classical ST-T wave changes associated with angina. This observation was consistent with the findings of Liberthson et al. in 1979 [17].
Table 4 Clinical symptoms of included coronary artery fistula patients with different age groups.
| Symptoms |
A(Age>30 y) |
B(20 y |
C(Age<20 y) |
| Number of patients: |
7 (63%) |
2 (18%) |
2 (18%) |
| Chest tightness/angina |
4 (57%) |
1 |
0 |
| Tachypnea/dyspnea |
3 (42%) |
1 |
0 |
| Palpitations and Dizziness |
2 (28%) |
0 |
0 |
| Recurrent upper respiratory infections or pneumonia |
0 |
2 |
2 |
| Hematochezia,Constipation |
1 (14%) |
0 |
0 |
| Polydipsia,polyphagia,polyuria |
1 (14%) |
0 |
0 |
| Comorbidity |
All (100%) |
None |
None |
Physical examination and electrocardiogram (ECG)
In our study, on physical examination, seven patients (64%) had a cardiac murmur, four patients (36%) had no obvious cardiac murmur. Accordingly, we divided the patients into two groups A and B, (Table 5). We have found that a mild mid-diastolic murmur is audible when the fistula drains to the left ventricle. Simultaneously, a continuous cardiac murmur at the left or right sternal border is heard when the fistula drains into a thoracic vessel or into the right ventricle. If the cardiac murmur sounds like a working machine, it can mimic a persistent ductus arteriosus; however, in our study, three patients (27%) had coronary arterial drainage into a pulmonary artery fistula without an obvious cardiac murmur. This observation was in conflict with the 1979 study of the Liberthson et al. [17] and with our own study. One possible explanation is that the extreme tortuosity of the fistula route decreased the volume and flow velocity of the shunted blood to such an extent that there was no audible cardiac murmur. Moreover, one patient with a left-coronary-artery-toright- ventricle fistula did not have a cardiac murmur, which may be explained by the small volume of the blood. We observed that the nature of the cardiac murmur is influenced by the origin, route, termination, and size of the fistulae, and by other characteristics of the patient, including age, and comorbidities, although it is difficult to formulate a general principle regarding the association of a murmur with specific characteristics of CAFs. Nonetheless, we can probably deduce that if a cardiac murmur is continuous, the fistula is a CVF.
Table 5 Characteristics of the fistula with (A group) or without (B group) cardiac murmur.
| Case/Age/Gender |
Cardiac murmur |
Single/Multiple Fistulae |
Origin |
Fistula Routea |
Termination |
| A*-1 21 y Male |
grade 3–4/6 DM sighing sound in apical area (mitral valve) |
S |
LCx |
straight |
LV |
| A*-2 35 y Male |
grade 3/6 DM cardiac murmur at the left sternal border 3rd intercostal space; |
S |
RCA |
straight |
LV |
| grade 2/6 DM sighing sound over mitral valve |
| Thrill |
| A*-3 10 m Female |
grade 3/6 SM cardiac murmur at left sternal border 2nd intercostal space |
S |
LM |
straight |
RA |
| A*-4 3 y Male |
continuous cardiac murmur at left sternal border 4th intercostal space |
S |
RCA |
straight |
RV |
| A*-5 55 y Female |
grade 3/4 continuous cardiac murmur at left sternal border 3-4 |
S |
D |
tortuosity |
RVOT |
| A*-6 29 y Female |
continuous cardiac murmur at left or right sternal border |
S |
RCA |
straight |
SVC |
| A*-7 72 y Male |
continuous cardiac murmur at left sternal border 6th intercostal space |
M |
LM,LAD,LCx |
tortuosity |
PA |
| B#-1 39 y Male |
Normal |
M |
RCA,LM,LAD |
tortuosity |
PA |
| B#-2 74 y Male |
Normal |
S |
LAD |
tortuosity |
PA |
| B#-3 48y Male |
Normal |
S |
LM,LCx |
tortuosity |
PA |
| B#-4 44y Male |
Normal |
S |
LM |
straight |
RV |
A: Fistula route=Pathways of coronary fistulae; S: single; M: multiple ; DM: diastolic murmur; SM: systolic murmur; *: with cardiac murmur; #: without cardiac murmur; LM: left main artery ;LAD: Left Anterior Descending Artery; LCx: left circumflex artery; D: diagonal artery; RCA: right coronary artery; LV: left ventricle; RV: right ventricle; RA: right atrium; PA: pulmonary artery; SVC: superior vena cava; RVOT: right ventricular outflow tract.
The ECG findings were non-specific, usually interpreted as myocardial ischemia. In the presence of a large fistula, there may be cardiomegaly and signs of volume overload.
64-slice CT and management
Only one patient in our study, who had a proximal first-diagonalartery- to-right-ventricular-outflow-tract (RVOT) fistula, was misdiagnosed as having a left-coronary-pulmonary-artery fistula. This misinterpretation may have been because the origin of first diagonal artery is from the left coronary artery, and the dilated left main and the left anterior descending artery influenced the observation of the origin of the fistula. Fortunately, the misdiagnosis did not misdirect the surgery.
CAG is, to date, the gold standard for the evaluation of coronary artery disease, but through this study, we found that 64-slice CT can provide high-quality functional and anatomical information regarding CAFs. Thus, 64-slice CT should be the preferred imaging technique for the radiologic evaluation of many types of CAFs, and especially in complex and large CAFs with complex vascular anatomy [18,19]. Because of the recent advances and superior spatial resolution of 64-slice CT, this technique is able to delineate clearly the origin and course of the anomalous coronary artery, and to demonstrate the lung parenchyma distinctly [20].
Surgery and direct epicardial or endocardial ligations traditionally have been regarded as the main therapeutic method for the closure of coronary artery fistulae [21]. Surgical correction is safe and effective, with good results [21-23]; however, in our study, among the five patients who elected to have surgery, to date, three patients have a residual fistula, and two patients are without obvious residual fistula. The CAFs of all three patients with residual fistulae are characterized as CCFs; the predominant reason for this observation may be related to the process of the formation of the CCFs. During the embryonic development of the coronary circulation, system intramyocardial trabecular sinusoids, which normally become narrow and persist only as Thebesian vessels in adults, are not obliterated, and thus, a fistulous communication persists between the coronary arteries and a cardiac chamber [13]. This kind of CAFs always has many small fistulae, making it difficult for the surgeon to ligate all of the fistulae. Other possible contributory factors may include the high ventricle pressure, and the experience of the surgeon. We would need more patients to confirm our conclusion. There is no published report addressing this question. Catheter-based closure of the fistulous connection is a non-surgical treatment option for closure of coronary fistulae. For adult asymptomatic patients with non-significant shunting, treatment of this condition is still a matter of debate.
Conclusion
Correct interpretation of the clinical presentation and physical examination, in consideration of the age of the patient, can call to mind CAFs, in order to include this entity in the different diagnosis. Then, the 64-slice CT can help to confirm and establish the diagnosis. More importantly, the 64-slice CT can provide much anatomic information regarding CAFs, and further delineate the complications of the CAFs. It is critical for the doctor to choose the best management of the CAFs. Only in this way can we successfully treat the patient with CAFs and decrease the associated morbidity and mortality. Additionally, any patient undergoing surgery should undergo CT in follow-up to rule out the residual fistulae, especially in a patient with CCFs.
Limitation
Our study has some limitations. First, this pilot study included only a small number of cases, and larger studies are needed to find statistical correlations. This study, however, highlights the importance of clinical data of the patients with CAFs, and confirms that the 64-slice CT can clearly display the origin, course, and termination of CAFs, and the anatomy of the cardiovascular system. Second, the relatively high dose of radiation of CTA is a general limitation of the technique; however, new developments, such as the recent introduction of dual-source CT scanners, systematically allow the use of ECG pulsing, and individualized regulation of the body mass index (BMI) [24,25] significantly reduces the dose received by the patient.
References
- Agarwal PP, Dennie C, Pena E, Nguyen E, LaBounty T, et al. (2017) Anomalous coronary arteries that need intervention: review of pre- and postoperative imaging appearances. Radiographics 37: 740-757.
- Garçon P, Vaislic C, Mostapha S (2008) Imaging techniques for diagnosing a giant coronary artery fistula. Archives of Cardiovascular Disease 101:425-427.
- Achenbach S, Ulzheimer S, Baum U, Kachelriess M, Ropers D, et al. (2000) Noninvasive coronary angiography by retrospectively ECG-gated multislice spiral CT. Circulation 102(23):2823–2828.
- Schmitt R, Froehner S, Brunn J, Wagner M, Brunner H, et al. (2005) Congenital anomalies of the coronary arteries: imaging with contrast-enhanced, multidetector computed tomography. Eur Radiol 15:1110–1121.
- Datta J, White CS, Gilkeson RC, Meyer CA, Kansal S, et al. (2005) Anomalous coronary arteries in adults: depiction at multi-detector row CT angiography. Radiology 235(3):812–818.
- Gupta M (2017) Coronary Artery fistula. Pediatrics: Cardiac Disease and Critical Care Medicine. Drugs & Diseases 10:18.
- Fujimoto N, Onishi K, Tanabe M, Koji T, Omichi C, et al. (2004) Two cases of giant aneurysm in coronary pulmonary artery fistula associated with atherosclerotic change. Int J Cardiol 97(3):577–578.
- Chan MS, Chan IY, Fung KH, Lee G, Tsui KL, et al. (2005) Demonstration of complex coronary-pulmonary artery fistula by MDCT and correlation with coronary angiography. AJR Am J Roentgenol 184:S28–S32.
- Zenooz NA, Habibi R, Mammen L, Finn JP, Gilkeson RC (2009) Coronary artery fistulas: CT findings. Radiographics 29:781–789.
- Tomasian A, Lell M, Currier J, Rahman J, Krishnam MS (2008) Coronary artery to pulmonary artery fistulae with multiple aneurysms: radiological features on dual-source 64-slice CT angiography. Br J Radiol 81: e218–e220.
- Zhang LJ, Zhou CS, Wang Y, Jin Z, Yu W, et al. (2014) Prevalence and types of coronary to pulmonary artery fistula in a Chinese population at dual-source CT coronary angiography. Acta Radiol 55:1031-1039.
- Verdini D, Vargas D, Kuo A, Ghoshhajra B, Kim P, et al. (2016) Coronary-Pulmonary Artery Fistulas: A Systematic Review. J Thorac Imaging 31:380-390.
- Loukas M, Germain AS, Gabriel A, John A, Tubbs RS, et al. (2015) Coronary artery fistula: a review. Cardiovasc Pathol 24:141-148.
- Gowda RM, Vasavada BC, Khan IA (2006) Coronary artery fistulas: clinical and therapeutic considerations. Int J Cardiol 107(1):7–10.
- Oncel D, Oncel G (2007) Right coronary artery to left ventricle fistula–effective diagnosis with 64-MDCT. Int J Cardiovasc Imaging 23:287-91.
- Abusaid GH, Hughes D, Khalife WI, Parto P, Gilani SA, et al. (2011) Congenital coronary artery fistula presenting later in life. Journal of Cardiology Cases 4: e43-e46.
- Liberthson RR, Sagar K, Berkoben JP, Weintraub RM, Levine FH (1979) Congenital coronary arteriovenous fistula: report of 13 patients, review of the literature and delineation of management. Circulation 59:849-853.
- Shiraishi J, Takahashi A, Kimura M, Miyagawa K, Torii S, et al. (2010) Usefulness of multidetector computed tomography for diagnosis and surgical treatment of large coronary artery fistula. Journal of Cardiology Cases 1: e106-e111.
- Seon HJ, Kim YH, Choi S, Kim KH (2010) Complex coronary artery fistulas in adults: evaluation with multidetector computed tomography. Int J Cardiovasc Imaging 26:261-271.
- Datta J, White CS, Gilkeson RC, Meyer CA, Kansal S, et al. (2005) Anomalous coronary arteries in adults: depiction at multi-detector row CT angiography. Radiology 235:812-818.
- Balanescu S, Sangiorgi G, Castelvecchio S, Medda M, Inglese L (2001) Coronary artery fistulas: clinical consequences and methods of closure: a literature review. Ital Heart J 2(9):669-676.
- Kamiya H, Yasuda T, Nagamine H, Sakakibara N, Nishida S, et al. (2002) Surgical treatment of congenital coronary artery fistulas: 27 years’ experience and a review of the literature. J Card Surg 17(2):173-177.
- Wang S, Wu Q, Hu S, Xu J, Sun L, et al. (2001) Surgical treatment of 52 patients with congenital coronary artery fistulas. Chin Med J 114(7):752-755.
- d'Agostino AG, Remy-Jardin M, Khalil C, Delannoy-Deken V, Flohr T, et al. (2006) Low-dose ECG-gated 64-slices helical CT angiography of the chest: evaluation of image quality in 105 patients. Eur Radiol 16(10):2137-2146.
- Muhlenbruch G, Hohl C, Das M, Wildberger JE, Suess C, et al. (2007) Evaluation of automated attenuation-based tube current adaptation for coronary calcium scoring in MDCT in a cohort of 262 patients. Eur Radiol 17(7):1850-1857.