Kelly Pennington1,2, Alexander Kogan2,3, Jeffrey Jensen4, Ognjen Gajic2,3and John C O’Horo2,4
1Department of Medicine, Division of Internal Medicine, Mayo Clinic; Rochester, MN, USA
2METRIC Group, Mayo Clinic, Rochester, MN, USA
3Department of Medicine, Division of Pulmonary and Critical Care Medicine, Mayo Clinic, Rochester, MN, USA
4Department of Anesthesiology, Division of Critical Care, Mayo Clinic, Rochester, MN, USA
5Department of Medicine, Division of Infectious Diseases, Mayo Clinic, Rochester, MN, USA
*Corresponding Author:
Kelly Pennington
Department of Medicine
Division of Internal Medicine
Mayo Clinic; Rochester, MN, USA
Tel: 13049202711
E-mail: Pennington.Kelly@mayo.edu
Received Date: October 12, 2016; Accepted Date: November 21, 2016; Published Date: November 28, 2016
Citation: Pennington K, Kogan A, Jensen J, et al. Evaluation of Data Utilization during Transfers of Critically Ill Patients between Hospitals. J Intensive & Crit Care 2016, 2:4.
Keywords
Critically ill patients; Inter-hospital patient; Intensive care unit; Critical care
Introduction
Critically ill patients have an increased risk of morbidity and mortality surrounding inter-facility transport [1]. Risks can be minimized with appropriate planning prior to transfer [2,3]. However, no practice guidelines exist regarding the transfer process, particularly in communication and hand-offs between providers. Hand-offs is a well-recognized risk factor for medical errors, which can lead to delays in diagnosis and/or treatment [4]. Importantly, standardized hand-off tools have been shown to reduce errors in patients transferring from the operating room to the surgical intensive care unit [5].
At transitions of care, information overload and inaccessible medical record data are common and lead to medical errors [2]. Failure to clearly communicate critical information at times of transition, such as transfer of care, significantly increases the risk of patient harm [6]. Previous studies have demonstrated a high degree of misinformation associated with ICU handovers compromising medical judgment [1]. Additionally, a lack of standard hand-off practices increases the risk of medical errors [7]. A potential solution to this problem is to identify data utilized by ICU physicians following transport of critically ill patients and to focus accompanying medical records on these high yield data points. A previous study attempting to understand the information requirements of ICU providers identified that ICU physicians utilized 11 data points, on average, during the admission of all ICU patients to make critical medical decisions [8].
For critically ill patients being transferred, necessary medical record data is often inaccessible, or if available, it may be excessive and unimportant. As such, an opportunity to standardize the hand-off processes and the opportunity to reduce patient harm exists [4,5,7]. Standardization requires the understanding of which data points clinicians require for clinical decision making following a transfer of a critically ill patient.
Materials and Methods
Our Institutional Review Board reviewed this study and approved it as a minimal risk study.
Study design
We conducted a prospective observational study of the initial physician-patient interactions taking place upon transfer of patients from outside hospitals to the Medical ICU at Mayo Clinic Hospital, St. Mary’s Campus (SMC). We observed the initial bedside patient-provider interactions upon admission to the medical ICU. We recorded data that was verbally requested by the clinicians and if that information was available in the accompanying records. Following the observation, we asked the treating providers to complete a survey regarding the information that they deemed critical and/or useful for clinical decision making. We administered a total of 45 surveys with 100% completion.
Study subjects
Data collection
Instruments
We developed the study instruments through expert consensus. The final instruments are shown in Addendum 1. The instruments consisted of pre-defined data points and open-ended responses. The additional self-reported responses were sorted into broad categories and analyzed as such.
Procedures
Once a direct admission episode was identified for inclusion in the study, we approached admitting team members, and the initial encounter with the transferring patient was observed. Immediately following the observation, admitting team members completed the study questionnaire.
Data analysis
Observation data
We conducted a primary analysis for the most requested and least requested items with a secondary analysis examining discordance between available and requested data.
Survey data
We performed a primary analysis for the data points most often and least often identified as critical/useful for clinical decision making. A secondary analysis to identify the effect that admission diagnosis had on the data points providers found useful was also conducted. Survey data was additionally analyzed to identify the number and type of data providers utilized as it correlated to their perceived patient acuity.
Results
Of the 25 provider-patient encounters observed, 4 patients were admitted for sepsis, 16 for respiratory failure, 1 for diabetic ketoacidosis, 2 for gastrointestinal bleed, 1 for hemodynamically unstable atrial fibrillation, and 1 for drug overdose. Of the 45 surveys completed, 16 were completed by the junior resident, 14 by the senior resident, 8 by the critical care fellow, 5 by the nurse practitioner/physician assistant, and 2 by the consultant physician.
Observation data
The most requested data were blood culture results, code status, and medications administered to the patient (Figure 1). Blood culture and code status were requested on 19/25 (76%) admissions observed and medications previously administered was requested on 16/25 (64%) observations. The least requested data were components of the basic metabolic panel and complete blood count. Creatinine was requested on 6/25 (24%) observations, electrolytes were requested on 2/25 (8%) observations, white blood cell count was requested on 9/25 (36%) observations, and hemoglobin/platelet count was requested on 4/25 (16%) observations. Code status, arterial/venous blood gas, lactate, and medical power of attorney were the most frequently unavailable data points when requested (Figure 2). Code status was unavailable on only 7 out of 19 occasions (37%). Arterial/ venous blood gas was unavailable on 5 out of 12 occasions (42%). Lactate was unavailable on 4 out of 10 occasions (40%). Medical Power of Attorney (MPOA) was unavailable 3 out of 5 occasions when requested (60%) Alternatively, vital signs, blood culture results, components of the basic metabolic panel and complete blood count were available to providers more than 90 percent of the time when requested (Figure 2).
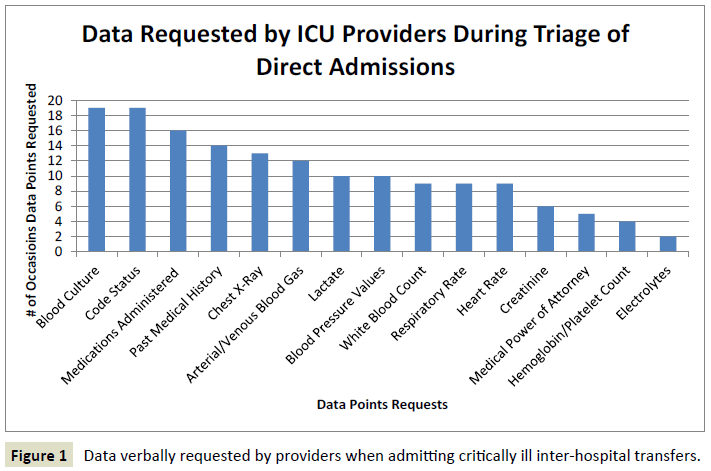
Figure 1: Data verbally requested by providers when admitting critically ill inter-hospital transfers.
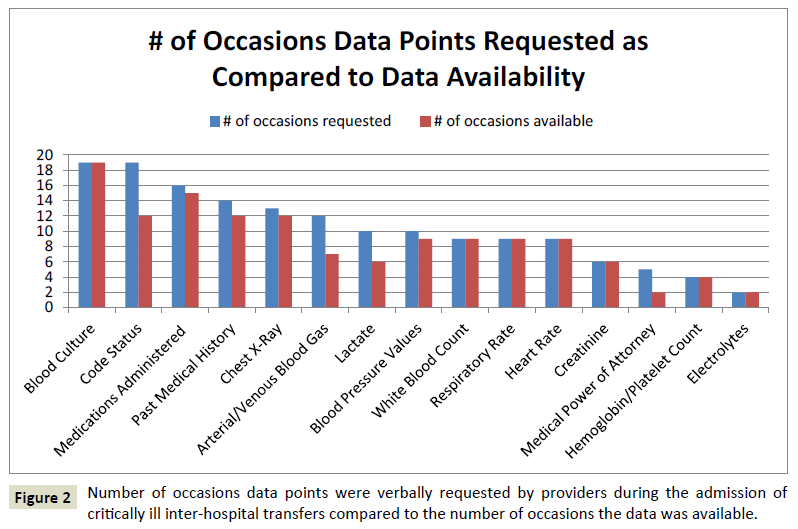
Figure 2: Number of occasions data points were verbally requested by providers during the admission of critically ill inter-hospital transfers compared to the number of occasions the data was available.
Survey data
Survey of practitioners demonstrated that code status was most often identified as being helpful for clinical decision-making (43/45, 96%) (Figure 3). Code status (43/45, 96%), medications administered (37/45, 82%), vital signs (33/45, 73%), white blood cell count (32/45, 71%), past medical history (31/45, 69%), chest x-ray (29/45, 64%), lactate (28/45, 62%), components of arterial/ venous blood gas (26/45, 58%), hemoglobin (25/45, 56%), and blood culture status(25/45, 56%) were identified as useful information by providers on more than 50% of occasions (Figure 3).
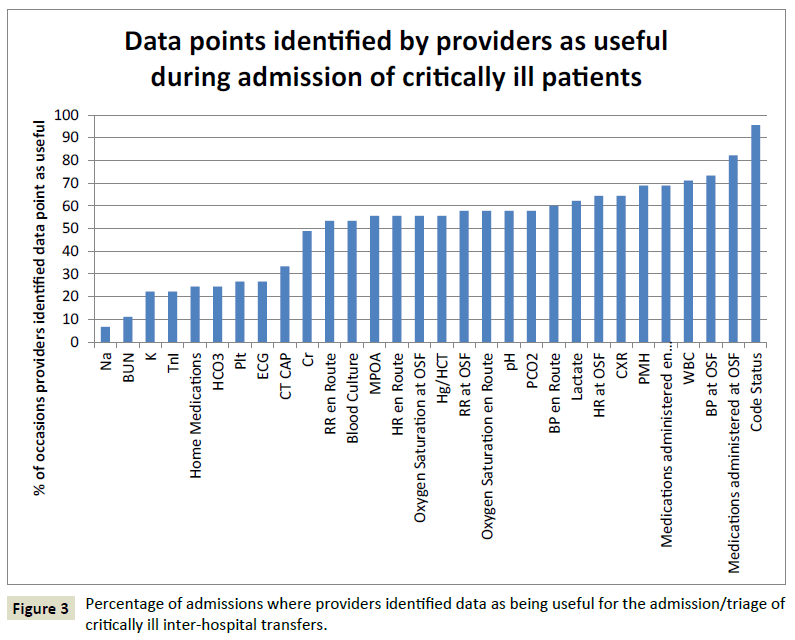
Figure 3: Percentage of admissions where providers identified data as being useful for the admission/triage of critically ill inter-hospital transfers.
Code status was deemed useful by providers on all admissions except when the reason for an intentional overdose (Figure 4). Reason for ICU admission also did not change providers’ opinions regarding the utility of blood pressure (70-76 percent of occasions), heart rate (61-63 percent of occasions), and electrolytes (15-38 percent of occasions). Oxygen saturation, respiratory rate, pH, and pCO2 were deemed useful on more occasions when the patient was admitted to the ICU for respiratory failure rather than sepsis or other diagnosis. Oxygen saturation was selected as useful on 87 percent of admissions for respiratory failure versus 31 percent and 13 percent of admissions for sepsis and other etiologies, respectively. Similarly, respiratory rate and pH were useful on 79 percent of admissions for respiratory failure versus less than 50 percent of admissions for sepsis and other diagnoses. pCO2 was identified as useful on 83 percent of admissions for respiratory failure compared to 46 and 12 percent of admission for sepsis and other diagnoses. Alternatively, blood cultures, lactate and white blood cell count were desired on 84, 82 and 94 percent of admissions for sepsis versus 50, 58 and 67 percent of admissions for respiratory failure.
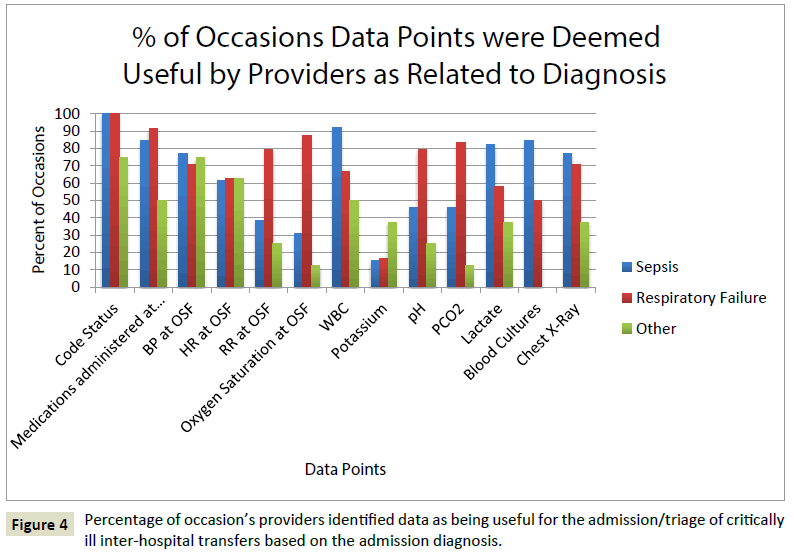
Figure 4: Percentage of occasion’s providers identified data as being useful for the admission/triage of critically ill inter-hospital transfers based on the admission diagnosis.
Perceived degree of illness
The average number of data points utilized by healthcare providers increased with the perceived severity of illness. On average, 13 data points were utilized for patients with perceived “mild” illness versus 18 data points for patients with “severe” illness. The number of historical (“mild”=4, “moderate”=5, “severe”=4) and imaging (“mild”=1, “moderate”=1, “severe”=1) data points utilized did not vary based upon the perceived severity of illness. The number of physical exam (“mild”=4, “moderate”=5) and laboratory (“mild”=4, “moderate”=5) data points utilized did not change between “mild” and “moderate” illness, but was increased with “severe” illness (physical exam=6, laboratory=6).
Discussion
Our study appears to demonstrate that critical care providers of varying degrees of experience use a small number of data points during the initial assessment of critically ill inter-hospital transfers. The most requested data were blood culture status, code status, and medications administered to the patient. Other data points identified as useful were past medical history, vital signs, white blood cell count, hemoglobin, lactate, pH, PaCO2 and chest x-ray findings. Unfortunately, we identified a deficiency in the availability of this data. Despite being the most requested data point, code status was one of the most unavailable data points along with arterial/venous blood gas, lactate and medical power of attorney. The admission diagnosis appeared to have minimal effect on the data points providers deemed as useful. Oxygen saturation, respiratory rate and components of arterial/ venous blood gas were intuitively identified as useful more frequently when patients were transferred for respiratory failure. Likewise, lactate, blood cultures, and white blood cell count were more frequently identified as useful in patients being admitted for sepsis. The overall quantity of data points utilized by ICU providers during the direct admission process varied with the perceived severity of illness of the patient. Historical and imaging data points were constant across the spectrum of illness; however, objective data points utilized increased if the patient was perceived to be “severely” ill.
Data that was easily reproducible for providers, such as components of the complete blood count and metabolic panel were the least requested and deemed the least valuable. Data that could not be easily reproduced, such as pre-antibiotic blood cultures and early arterial/venous blood gas, were frequently requested by providers, and not reliably available. The types of information utilized in the admission process were similar to those identified by Pickering et al. [8], however, the number of data points utilized during the admission of critically ill patients was found to be greater in our study. This is most likely secondary to previous care and complex hospital courses that are unique to inter-hospital transfers. In addition, we found a higher value placed on historical items such as code status, past medical history, and medications. We believe this is likely secondary to inter-hospital transfer patients having an already varied hospital course at another institution making medications administered and medical history more relevant to the patient’s current clinical situation. Interestingly, providers requested and identified code status as an important decision-making data point in all but one clinical encounter, yet this was also the most frequently unavailable data point. Recent emphasis on end-of-life care and research on hospital admission code status discussions [9] is likely driving the desire for this data point. It is understandable that accepting providers want to know what a patient wish was at the referring facility in the case of cardiac and/or respiratory arrest as many times they may not be able to have a thoughtful discussion or an appropriate surrogate may not be present to confirm shortly after arrival to the referring facility.
While previous studies have demonstrated that Critical Care physicians use a small number of available clinical information to make medical decisions [8], they fail to clearly identify relevant data points, the factors that influence the utility of different data points, and the frequency of data point availability to providers during inter-hospital transfers. Additionally, the concept of limited data point utilization for medical decision making, to the best of our knowledge, has never been applied to interhospital hand-offs of critically ill patients. Assessment and care of critically ill patients generates numerous data points. One study of critically ill pediatric patients demonstrated that 1,348 data points were generated per patient per day [10].
While the number of data points generated per critically-ill patient prior to transfer to a tertiary or quaternary care facility has never been examined secondary to varied hospital courses and duration of care, we know that information overload and inaccessible medical records lead to medical errors [2] and standardized hand-off practices can prevent these errors [7]. Multiple studies have examined the intra-hospital hand-off process in the intensive care unit [11,12] and have found that structured patient-centered handoff tools effectively support communication and improve patient safety. It stands to reason that a standardized handoff tool for inter-hospital transfer of critically ill patients would reduce medical errors and improve the care continuum.
Limitations
This study was performed in a single center and the reported clinical information may be idiosyncratic to that center. We only examined the Medical Intensive Care Unit; as such, the reasons for admission to the ICU were limited predominantly to sepsis and respiratory failure. Additionally, this study occurred at a teaching institution and the information we gathered was from residents, fellows, mid-level providers, and consultants. Most of the data was obtained from junior level physicians. Due to the limited number of patient observations, an individual clinician bias to particular data points may be reflected in the results. In order to prevent a bias toward over-reporting of data utilization by providers, we attempted to capture both perceived data use and actual data use by doing both observations of requested data and surveys. The data patterns appeared similar in both groups leading us to believe that providers were accurately reporting data utilization patterns.
While this study was performed in a single center, it highlights the importance of local culture and practice. Further multiinstitutional studies are warranted; however, this study highlights the feasibility of the study design and concept that a limited number of data points can be identified to formulate standardized hand-off tools for inter-facility transfers of care.
Conclusion
Critical care providers used a small number of data during the inter-hospital transfer process and many perceived critical points were frequently unavailable or unknown. Admission diagnosis appeared to minimally affect which data points providers deemed useful. The overall quantity of data points utilized by ICU providers during the direct admission process varied with the perceived severity of illness of the patient. A formal structured hand off tool is needed to improve information management during inter-hospital transfer of critically ill patients, emphasizing ongoing interventions, time-sensitive tests and goals of care.
References
- Pickering BW, Hurley K, Marsh B (2009) Identification of patient information corruption in the intensive care unit: Using a scoring tool to direct quality improvements in handover. Crit Care Med 37: 2905-2912.
- Harrahill M, Bartkus E (1990) Preparing the trauma patient for transfer. J Emerg Nurs 16: 25-28.
- Warren J, Fromm RE Jr., Orr RA, Rotello LC, Horst HM (2004) Guidelines for the inter and intra hospital transport of critically ill patients. Crit Care Med 32: 256-262.
- Horwitz LI, Moin T, Krumholz HM, Wang L, Bradley EH (2008) Consequences of inadequate sign-out for patient care. Arch Intern Med 168: 1755-1760.
- Lane-Fall MB1, Beidas RS, Pascual JL, Collard ML, Peifer HG, et al. (2014) Handoffs and transitions in critical care (HATRICC): Protocol for a mixed methods study of operating room to intensive care unit handoffs. BMC Surg 14: 96.
- Bracco D, Favre JB, Bissonnette B, Wasserfallen JB, Revelly JP, et al. (2001) Human errors in a multidisciplinary intensive care unit: A 1 year prospective study. Intensive Care Med 27: 137-145.
- Sherlock C (1995) The patient handover: A study of its form, function and efficiency. Nurs Stand 9: 33-36.
- Pickering BW, Gajic O, Ahmed A, Herasevich V, Keegan MT (2013) Data utilization for medical decision making at the time of patient admission to ICU. Crit Care Med 41: 1502-1510.
- Anderson WG, Chase R, Pantilat SZ, Tulsky JA, Auerbach AD (2010) Code status discussions between attending hospitalist physicians and medical patients at hospital admission. Journal of General Internal Medicine 26: 359-366.
- Manor-Shulman O, Beyene J, Frndova H, Parshuram CS (2008) Quantifying the volume of documented clinical information in critical illness. J Crit Care 23: 245-250.
- Abraham J, Kannampallil TG, Patel VL (2012) Bridging gaps in handoffs: A continuity of care based approach. J Biomed Inform 45: 240-254.
- Collins SA, Mamykina L, Jordan D, Stein DM, Shine A, et al. (2012) In search of common ground in handoff documentation in an Intensive Care Unit. J Biomed Inform 45: 307-315.

