Keywords
Topical Aminolaevulinic Acid (ALA); Hydroxypyridinone; Iron Chelation; Photodynamic Therapy (PDT); Protoporphyrin IX (PpIX); Skin
Introduction
Protoporphyrin IX (PpIX)-induced photodynamic therapy (PDT) is used clinically as topical method of localised ablation of certain non-melanoma skin cancers and precancers [1]. This light activated drug treatment requires a photosensitising agent (in this case aminolaevulinic acid (ALA)-induced PpIX), light of a specific wavelength (635 nm) and molecular oxygen [2] in order to work. When combined concurrently in sufficient amounts these three components result in the production of reactive oxygen species (ROS) and oxidative stress [3], which damages cellular components producing cell death via necrosis, apoptosis and/or autophagy depending on the dose parameters utilised [4]. Excellent cosmetic results also make PpIX-induced PDT particularly suitable for many dermatological applications [5].
ALA-PDT was first introduced experimentally in 1987 [6], with the first clinical treatments being reported in 1990 [7]. Extensive clinical trials have since been conducted on many malignant and non-malignant skin conditions. Within the clinical dermatology setting, topical PpIX-PDT now involves the application of a cream formulation to the area to be treated. This cream contains a PpIX precursor, usually ALA or its methyl ester (MAL). The area is then covered with a light-occluding dressing for a number of hours (usually 3 h) during which time the precursor is absorbed into the lesion and converted via haem biosynthesis to produce the naturally occurring photosensitiser, PpIX. Endogenously applied ALA therefore acts as a substrate for the production of haem and its precursors whilst avoiding the negative feedback loop that haem has on its own production. The intermediate immediately preceding haem in the haem biosynthesis pathway is PpIX and this accumulates following ALA administration because the last step of haem biosynthesis (the insertion of ferrous iron into the porphyrin ring of PpIX by ferrochelatase to form haem) [8] is relatively slow. This conversion is the secondary rate limiting step of the pathway. The primary rate limiting step of haem biosynthesis being the formation of ALA by ALA synthase which is bypassed by exogenous ALA administration.
Once PpIX accumulation has occurred within the tumour cells in this manner (it should be noted that haem biosynthesis tends to be upregulated in diseased cells and so occurs faster in tumours than in the normal surrounding tissues), visible light matching both the absorption spectrum of the photosensitiser (PpIX) and the optimum wavelength for tissue transmission is applied to the tumour. Normally red light of the wavelength 635 nm is utilised in dermatology for all but the most superficial lesions and is frequently delivered using a LED array [9]. PpIX absorbs energy from the light and type-I or type-II reactions proceed to produce cellular damage, which if sufficient can be cytotoxic [10].
Substantial subsets of skin tumours still exist clinically that are relatively difficult to treat with conventional therapies such as surgery and cryotherapy because of their size, location or number within an area of field change [11]. In these situations, PDT can be advantageous and has the added benefit of being associated with excellent cosmesis. This makes it particularly attractive as a treatment option for lesions located in highly visible sites [12]. Standardised topical dermatological PpIX-PDT protocols utilising either ALA (Ameluz, Spirit Healthcare, UK) or MAL (Metvix, Galderma, UK) now exist and are highly effective when the disease is superficial [13] but improvement is required to treat thicker or acrally located conditions [14]. Many adaptations to standard PDT treatment have been considered to improve efficacy in these more difficult to treat clinical applications (including skin stripping with tape [15] and combinations with other techniques such as lowdose Photofrin® [16], hyperthermia [17,18], iontophoresis [19] and bioreductive drugs [20], however one of the most promising techniques is utilising an iron chelating agent to increase cellular accumulation of PpIX. This works by reducing the bioconversion of PpIX to haem by ferrochelatase (an iron dependent process) thus increasing cell kill on subsequent irradiation.
The concurrent use of iron chelating agents to enhance PpIXinduced PDT in general, has been investigated with some success and includes iron chelating agents such as ethylenediamine tetraacetic acid (EDTA) [21-24] and desferrioxamine (DFO) [21, 25-28]. The novel hydroxypyridinone iron chelator 1, 2-diethyl- 3-hydroxypyridin-4-one hydrochloride (CP94) is a member of the hydroxypyridinone family of oral iron chelators, which were originally developed to try supersede DFO in the treatment of iron overload as this compound has to be administered intravenously clinically via long infusion. CP94 is particularly effective at chelating intracellular iron and has a lower molecular weight and higher lipophilicity than either DFO or EDTA [29] and has been found to be superior to DFO in the production of elevated PpIX levels when directed compared in vitro [30]. Additional in vitro investigation has indicated that this effect can also be elucidated when using HAL (the hexyl ester of ALA) as well as ALA or MAL as the PpIX precursor [31]. In vivo, CP94 has been utilised intravenously to enhance ALA-induced PpIX fluorescence and necrosis in the normal rat colon [32] and to also produce greater tumour necrosis within a colonic rat tumour model [33]. However because CP94 experiences rapid first pass glucuronidation when administered orally to humans [34], a topical administration route for a dermatological PDT application may be preferable. Two small clinical pilot studies of CP94 in combination with ALA or MAL-induced PDT have been conducted to date and have demonstrated the safety and feasibility of adding this iron chelator to the photosensitising cream [35,36]. Additionally, although these clinical investigations were only designed to assess safety, some promising initial enhancements in tumour clearance were observed when CP94 was included within the photosensitising cream. However due to clinical constraints, it was not possible to assess PpIX production/excised tumour fluorescence within these pilot studies and the clinical protocol still requires optimisation prior to randomised controlled trials being conducted to consider efficacy. An additional in vivo investigation has therefore been conducted here to further investigate the topical availability of CP94 to enhance PpIX accumulation and subsequent PDT effect on irradiation within normal rat skin.
Methods
Chemicals
ALA (ALA.HCl powder (99.0% purity) DUSA Pharmaceuticals Inc., New York, USA) and the iron chelator CP94 (synthesised with 95.0% purity and kindly donated in powder form by the Department of Pharmacy, Kings College London), were prepared in a simple polyethylene glycol (PEG) base for topical application. A basic PEG cream (containing neither compound) was used as a blank (containing no compounds) control. PEG base preparations containing 200 mg/ml ALA, 100 mg/ml CP94 or 200 mg/ml ALA plus 100 mg/ml CP94 were also used. No adverse effects were observed when administering any of the compounds.
Animal model
Normal female Wistar rats (120 - 200 g) were used throughout. The animals were anaesthetised for all parts of the procedure using inhaled halothane (ICI Pharmaceuticals, Cheshire, UK). All animal work was conducted humanely and according to regulations under license from the Home Office, HM Government, UK.
Fluorescence studies
An area of skin on the animal’s flank was prepared prior to cream application. This was done by removing the animal’s hair using electric clippers followed by hand shaving using a scalpel blade. A foil stencil was applied so that only a 1 cm2 area of skin was exposed. 0.1 ml of the appropriate cream (ALA in PEG, CP94 in PEG, combined ALA plus CP94 in PEG or blank PEG control (containing no compounds)) was then spread over the 1 cm2 spot and covered with a dressing, two animals being treated with each set of parameters. Completely blank untreated control animals were also studied and these animals received no cream application whatsoever. The animals were recovered and killed serially at various times after topical application (1 - 8 hours). The treated area of skin (hereafter denoted as “treated”) along with a similar untreated (but shaven) area of skin from the opposite flank (hereafter denoted as “untreated”) were removed and snap frozen in liquid nitrogen, so that frozen sections could be analysed by fluorescence microscopy. Ten micrometre thick cryosections were prepared together with adjacent sections for Haematoxylin and Eosin (H & E) staining.
Phase contrast microscopy with a slow-scan cooled charge coupled device (CCD) camera (Wright Instruments Ltd., Enfield, London, UK) was used to image and quantify fluorescence on the frozen sections. The fluorescence was excited using an 8 mW helium-neon laser (632.8 nm) and detected between 665 and 710 nm using bandpass and longpass filters as described previously [37]. A pseudo colour-coded image of the fluorescence signal in counts per pixel was produced and the fluorescence intensity in each tissue layer was quantified digitally by averaging over specified areas. All fluorescence measurements were corrected for background autofluorescence and structures were identified by correlation with the adjacent H & E stained section. Two measurements were made and averaged per section. Intensity calibrations were performed using a 0.1 mm thick ruby disc which emits near 690 nm under 633 nm excitation. A previous study using the same system [38] on normal rat colon using intravenous ALA has demonstrated that the CCD fluorometric measurements of porphyrin fluorescence correlated well with chemical extraction measurements. Statistical analysis between the means of the ALA only and ALA plus CP94 groups, at the time of maximum fluorescence, was conducted using an unpaired student t-test and error bars were determined by the standard error of the mean.
Fluorescence emission spectra were also recorded from separate representative frozen specimens to confirm that the fluorescence observed in the imaging was indeed produced by PpIX and no other fluorescent porphyrin. This was carried out by placing the skin specimen on a glass slide under the plate well reader of a luminescence spectrometer (Perkin Elmer Ltd., Beaconsfield, Buckinghamshire, UK). This was set to read over the range of 600 - 750 nm, exciting with 410 nm light and using 10 nm slits with a 530 nm cut off filter in place to remove scattered excitation light. Normal autofluorescence was detected in skin from untreated control animals and subtracted from the treated spectra. Calibration using a rhodium disc was conducted both before and after taking spectra.
PDT studies
All compounds were administered to prepared skin (in the same way as the fluorescence studies) 5 hours prior to irradiation. The light source was a Medi-Sun arclamp (Medical Light Technologies, Glasgow, Scotland) irradiating at 630 nm (+/- 20 nm). A total energy dose of 100 J was administered to 1 cm2 areas of skin (with the surrounding skin shielded) at a fluence rate of 150 mW/ cm2. The shielding was then removed and the animals recovered. Each treatment site was assessed regularly over 14 days using the scale presented in Table 1 (adapted from [39,40].
| Value Recorded |
Observation Made |
| 0 |
No effect |
| 1 |
Minimal redness |
| 2 |
Redness |
| 3 |
Dry desquamation |
| 4 |
Thin scab formation |
| 5 |
Thick scab formation |
Table 1: Scale (adapted from [39, 40]) used to assess each treatment site following PDT treatment with each set of parameters investigated.
This enabled the effect of each treatment (ALA + light, CP94 + light, ALA plus CP94 + light, light only control, ALA only control, CP94 only control and blank control) to be compared, with four animals being treated with each set of parameters. Statistical analysis between the means of the ALA + light and ALA plus CP94 + light groups at the time of maximum PDT damage was conducted using a Wilcoxon signed-rank test.
Results
Tissue fluorescence quantification
A representative set of photographs can be seen in Figure 1. One pair (Figures 1a and b) shows a typical pseudo colour coded CCD image of the skin with its matched H & E stained photograph, five hours after topical administration of 0.1 ml of 200 mg/ml ALA cream to a 1 cm2 area of skin. The other pair (Figures 1c and d) shows the same images, five hours after administration of 0.1 ml of 200 mg/ml ALA + 100 mg/ml CP94 cream to another 1 cm2 area of skin. The fluorescence observed in the epidermis is much greater with the administration of CP94 in combination with ALA, than ALA administration alone. In both cases the hair follicles can be seen to fluoresce greatly, as does the stratum corneum.
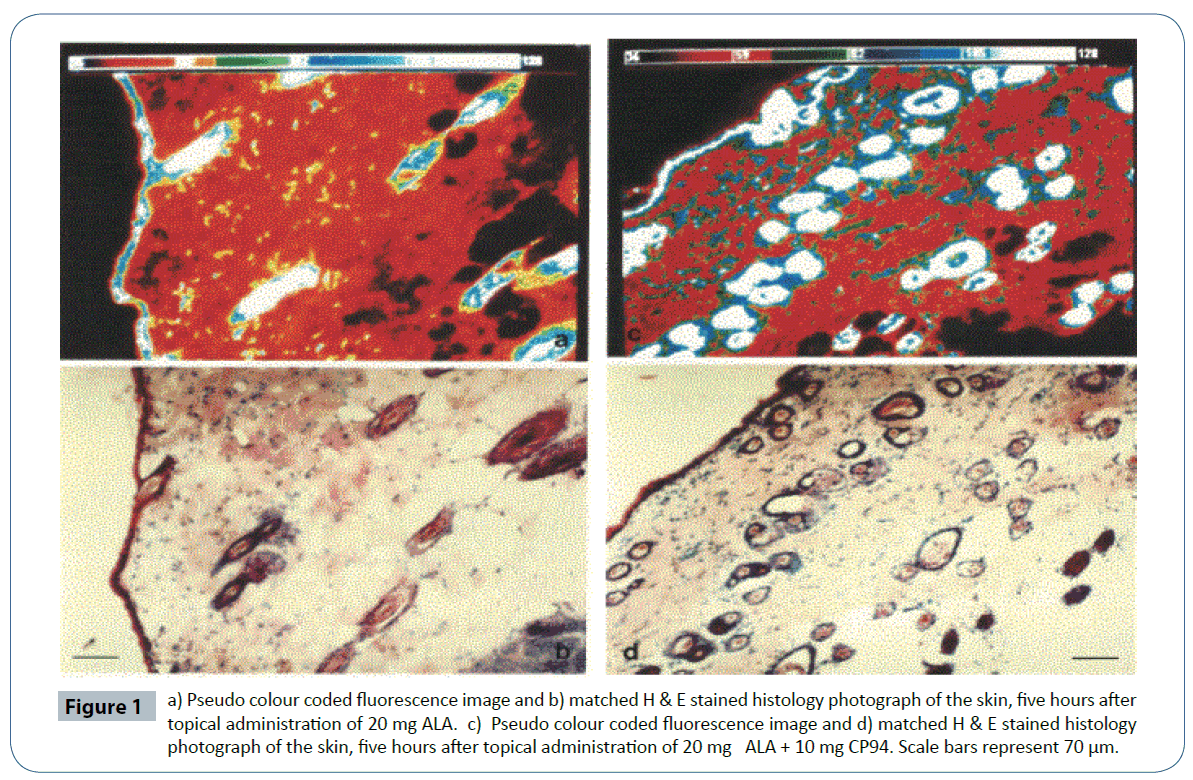
Figure 1 a) Pseudo colour coded fluorescence image and b) matched H & E stained histology photograph of the skin, five hours after topical administration of 20 mg ALA. c) Pseudo colour coded fluorescence image and d) matched H & E stained histology photograph of the skin, five hours after topical administration of 20 mg ALA + 10 mg CP94. Scale bars represent 70 μm.
(Figure 2a) shows how the fluorescence in the epidermis of the skin varied with time after topical application of ALA alone and ALA plus CP94. Measurements were taken from the epidermis of each section avoiding the highly fluorescent hair follicles and stratum corneum. The combination of ALA plus CP94 produced a substantial increase in fluorescence in the tissue (29.0% elevation) over that achieved with ALA administration alone and statistically (in this small sample), this observation did not quite reach significance at the p < 0.05 level (p < 0.09). This elevated level of PpIX peaked at 5 hours however, which was the time chosen for the subsequent photodynamic studies. (Figure 2b) shows the fluorescence profile from the matched untreated skin specimens taken from the opposite flank of the same animals. Fluorescence in these untreated areas hardly rose above background levels (which have been subtracted from all fluorescence measurements).
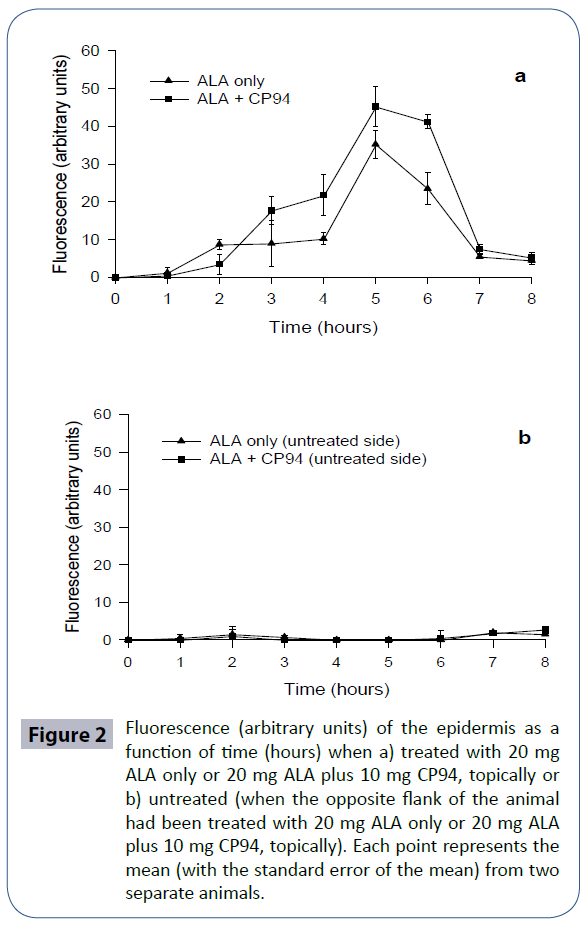
Figure 2 Fluorescence (arbitrary units) of the epidermis as a function of time (hours) when a) treated with 20 mg ALA only or 20 mg ALA plus 10 mg CP94, topically or b) untreated (when the opposite flank of the animal had been treated with 20 mg ALA only or 20 mg ALA plus 10 mg CP94, topically). Each point represents the mean (with the standard error of the mean) from two separate animals.
Fluorescence spectroscopy
Fluorescence spectra were recorded (using the spectrometer) from frozen specimens of tissue taken from animals given each treatment regime and representative spectra are shown in (Figure 3). The spectra from blank control sections (no compounds administered) were subtracted from each spectrum to correct for endogenous autofluorescence. No significant differences were observed between the ALA only (Figure 3a) and the combination of CP94 and ALA (Figure 3b) spectra or any other spectra recorded during this study, indicating that the administration of the CP94 iron chelating agent did not induce significant production of fluorescent species other than PpIX. Maxima were at 636 +/- 2 nm in each case.
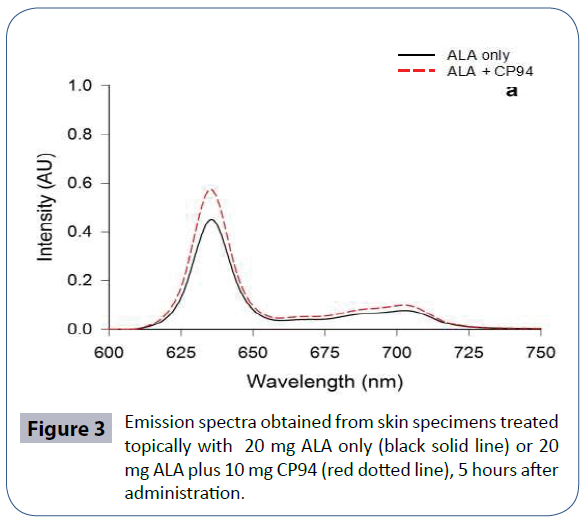
Figure 3 Emission spectra obtained from skin specimens treated topically with 20 mg ALA only (black solid line) or 20 mg ALA plus 10 mg CP94 (red dotted line), 5 hours after administration.
Photodynamic effects
The effect of CP94 on ALA induced PDT is presented in Figure 4. Each point represents the four animals treated in each group, the assessment scale score of each being averaged for each day. A much greater effect (an increase by up to a factor of three) was obtained when using the combination of ALA plus CP94 rather than ALA alone and again this observation did not quite reach significance at the p < 0.05 level (p < 0.07) in this limited sample size. It should be noted, however, that the assessment score recorded was the highest that occurred within the treated area and in general “patchy” effects were produced, some parts of the 1 cm2 spot being affected more than others. No effect was seen until day 2. The maximum effect was observed at 4 days and was resolved completely by day 7. At day 14, all treatment sites appeared normal and in all but one instance, substantial hair regrowth had occurred. CP94 only plus light, light only, ALA only, CP94 only, PEG only and blank controls were also conducted, none of which produced any effect.

Figure 4 Treatment effect (arbitrary units) as a function of time (days) following topical PDT treatment with 20 mg ALA only or 20 mg ALA plus 10 mg CP94 and 100 J/cm2, 630 nm irradiation (150 mW) 5 hours later. Each group represents the mean (with the standard error of the mean) from four separate animals.
Discussion
PDT using topical ALA has been shown over the last few years to be an effective treatment for conditions like actinic keratosis, Bowen’s disease and superficial basal cell carcinomas, with the only main side effect being discomfort/pain during irradiation [11,41]. The treatment of nodular basal cell carcinomas and other thicker cutaneous lesions with a single topical PpIX-induced PDT treatment is as yet, however, unsatisfactory, with low complete response rates and high recurrence rates [42] as the depth of necrosis produced remains insufficient [43]. One way to overcome this problem may be the administration of an iron chelating agent in combination with ALA, as reported here. This simple pharmacological modification may enhance the effect of the treatment by producing more damage, without prolonging the duration of treatment protocol.
Clinically Fijan et al. [26] have already demonstrated the feasibility of combining the iron chelator DFO with ALA-PDT to treat 34 superficial basal cell carcinomas (BCCs) and 22 nodular BCCs with ALA. Lui et al. [23] have also found a promising and significant (p<0.01) reduction in tumour depth in lesions treated with EDTA in combination with ALA-PDT. Choudry et al. [25] however, could not detect any significant differences in surface fluorescence between lesions co-incubated with ALA±DFO despite DFO being demonstrated to be superior to EDTA in its ability to enhance PpIX-induced PDT [21]. Further work is therefore required to find a better suited and more effective iron chelating agent for this purpose (enhancement of PpIX-PDT), preferably with the benefit of a topical route of administration for these dermatological applications.
Previous in vitro experimentation with the hydroxypyridinone iron chelating agent CP94 has already indicated that that CP94 was consistently significantly superior to DFO in the production of elevated PpIX levels particularly within epidermal squamous carcinoma cells (A431) with minimal enhancement being observed in the normal skin fibroblasts and keratinocytes also investigated [30]. Furthermore, additional studies undertaken with CP94 alone within A431 cells have indicated that significantly increased PpIX levels and subsequent cytotoxicity can be produced when using HAL (the hexyl ester of ALA) as well as ALA or MAL as the PpIX precursor, when PDT is conducted within a variety of different oxygen conditions [31]. This experimentation has been extended here to consider the effect of topical CP94 administration in vivo in a normal rat skin model. In light of our previous findings with CP94 augmentation of PpIX-PDT demonstrated in epidermal squamous carcinoma cells (A431) [30,31], a colonic tumour model [33] and dermatological skin lesions [35,36], it was not deemed necessary to create a neoplastic skin model here when our main focus was to assess PpIX production/excised tumour fluorescence (which we have been unable to do clinically due to ethical constraints).
The quantitative CCD fluorescence microscopy presented here determined that the CP94 (when administered topically in combination with ALA) was able to increase the PpIX fluorescence detected in the epidermis of the normal rat skin by 29.0% at the fluorescence peak and this enabled an increase in the photodynamic effect by up to a factor of three to be achieved when compared with the effect of ALA alone. These findings both support and extend the previous in vivo experimentation conducted with intravenously administered ALA +/- CP94 in the rat colon [32,33] to a topical application. They also permit insight to the mechanisms that may explain the promising initial clinical results obtained with this enhanced treatment regime in the first clinical safety pilot studies [35,36]. As the increased therapeutic effects are most likely being conveyed through the elevated dermal PpIX accumulation observed following effective iron chelation achieved via topical CP94 administration. Pleasingly, no significant production of PpIX was detected in the untreated skin from the opposite flank in any of the animals studied. This was investigated as there have been reports in the literature [44] which describe porphyrins in untreated areas of skin indicating that some systemic effect may be produced when ALA is applied topically. There was no evidence of this in this study however, indicating that application of a simple light occlusive dressing to the treatment area alone should be sufficient to prevent clinical cutaneous photosensitivity even when hyper-accumulating even greater amounts of PpIX with an iron chelating agent.
The PDT changes produced in the normal rat skin were not found to affect all parts of the treatment site to the same extent. The reasons for this currently remain unclear. It could be explained by uneven drug distribution in the cream base employed or small scratches (produced during shaving) allowing uneven drug absorption. However, all preparations were thoroughly mixed prior to use and great care was taken during the shaving procedure. Furthermore, these potential causations should have been evident in the fluorescence microscopy and corresponding histology. The patchy effect may have also theoretically been caused by uneven light irradiation, although the damage appeared to be completely random and the power was checked both before and after the treatment and did not vary significantly over this period. Alternatively, it may have been due to naturally occurring irregularities in skin thickness or follicle distribution (which are particularly fluorescent). It should also be noted that the preparation employed to administer the compounds topically within this investigation was a simple polyethylene glycol (PEG) base. Clinically an emulsion type cream is typically employed to administer the PpIX prodrugs and the composition of this preparation varies depending on the commercial product being employed [1 and 13]. We have been able to circumvent this issue within our clinical investigations of CP94 to date [35, 36] by simply mixing the experimental CP94 compound into the commercially available preparation. However these formulations are complex in nature and design, vary from product to product and are expensive to purchase for non-clinical use. Furthermore emulsion creams are emollients with known moisturising properties that may have affected the results observed with our treatment assessment scale (Table 1; adapted from [39,40]. It was therefore decided utilise a simple PEG base here. However, looking to the future it is going to be important to derive a clinical formulation that includes CP94 as well as the PpIX-precursor of choice for maximum efficacy.
Although normal skin was investigated in this study, it is expected that the PDT effect induced by the treatment would be greater in a clinical application of this modification to abnormal skin. This is because the accumulation of PpIX occurs more rapidly within (pre) cancerous lesions/cells due to their disrupted stratum corneum (which facilitates better cream absorption), upregulation of the haem biosynthesis pathway within diseased cells that have greater metabolic demands as well as alterations in the expression of the porphobilinogen deaminase and ferrochelatase enzymes within the haem biosynthesis pathway [3,45]. These factors in combination all result in a window of opportunity for therapeutic light delivery (around 3 hours following cream application in human skin lesions), where PpIX is preferentially accumulated within the target diseased cells and as a result the surrounding normal cells are relatively spared by this localised ablative therapy [1]. It is interesting to note that the peak fluorescence observed in the normal rat skin investigated here occurred at the delayed time point of 5 hours after cream application. It would have been preferable to have been able to increase the group size of these fluorescence studies as statistically significance was not reached at the p < 0.05 level utilising this small sample size. Fluorescence spectral analysis using a spectrometer did confirm however, that the increased fluorescence observed could be attributed to PpIX and no other fluorescent porphyrins of the haem biosynthesis pathway (which may have feasibly been produced in elevated amounts by altering the biochemistry of this system with an iron chelating agent in this manner).
These findings also demonstrate the importance of the role of iron within the mechanism of PpIX-induced PDT with the increased PDT damage observed being related to the increased accumulation of PpIX pre-irradiation, an effect which was solely produced by the topical co-administration of the iron chelating agent, CP94. However, due to its multiple valences, iron can also play an important role in ROS biology [46] and has the potential to increase cytotoxicity from PDT as iron is important in the generation of the hydroxyl radical as well as in lipid peroxidation [47]. Singlet oxygen generated by PpIX-induced PDT can itself react with oxygen to generate superoxide, which is dismutated by superoxide dismutase within cells to form hydrogen peroxide. Hydrogen peroxide is usually detoxified via catalase to produce water and oxygen. However if hydrogen peroxide comes into contact with metal ions (especially Fe2+) then the highly reactive hydroxyl radical can be formed via Fenton reactions and this can lead to damage to cellular proteins, lipids and DNA [48]. Limiting the availability of iron via chemical chelation could therefore theoretically reduce the efficacy of PpIX-PDT by blocking or limiting this hydroxyl radical generating pathway so that a response less than that maximally feasible was produced by the treatment.
Previous experimental work undertaken with cultured human cells in an iron controlled/standardised environment has suggested however, that the role of limited iron levels in elevating PpIX accumulation has a greater effect on the level of cellular damage produced by PpIX-induced PDT than the role of excess iron availability in the formation of ROS (as the level of damage/ death was related to the differences in the accumulation of PpIX observed) [49]. A possible explanation for this may be that other transition metals (such as zinc or copper) may be able to mediate Fenton-type reactions instead of iron in the ROS cascades triggered by PpIX-PDT. Furthermore, although cellular iron levels are tightly regulated under normal circumstances, during oxidative stress iron homeostasis can be disrupted resulting in the release of labile iron [50-52]. This might mean that although iron chelation initially reduces iron availability, so that PpIX accumulation during PpIX-PDT is elevated, once a state of oxidative stress begins to occur on irradiation other transition metals and freshly released labile iron could perpetuate the ROS cascades via Fenton reactions in a timely and efficacious fashion.
It is important to note that no attempt was made in this time course investigation to determine the depth of the PDT effect and future studies should investigate this factor, which is obviously crucial to the success of this technique in dermatological applications. Nonetheless, it has been established that it is feasible to use the hydroxypyridinone iron chelating agent, CP94, topically in normal rat skin, to increase the PDT effect produced by ALA-induced PpIX photosensitisation. With continued investigation this pharmacological modification has considerable potential to improve dermatological PpIX-PDT practice.
Acknowledgement
We would like to thank Professor Robert Hider, King’s College London, for synthesising the iron chelating agent, CP94 and the Histopathology Unit of Cancer Research UK for conducting the histology required by this study. Financial support from an unrestricted research grant from DUSA Pharmaceuticals is also gratefully acknowledged.
References
- Morton CA, Szeimies RM, Sidoroff A, Braathen LR (2013) European guidelines for topical photodynamic therapy part 1: treatment delivery and current indications - actinic keratoses, Bowen's disease, basal cell carcinoma. J Eur Acad Dermatol Venereol 27: 536-544.
- Henderson BW, Dougherty TJ (1992) How does photodynamic therapy work? See comment in PubMed Commons below Photochem Photobiol 55: 145-157.
- Luna MC, Ferrario A, Wong S, Fisher AM, Gomer CJ (2000) Photodynamic therapy-mediated oxidative stress as a molecular switch for the temporal expression of genes ligated to the human heat shock promoter. Cancer Res 60:1637?1644.
- Buytaert E, Dewaele M, Agostinis P (2007) Molecular effectors of multiple cell death pathways initiated by photodynamic therapy. See comment in PubMed Commons below BiochimBiophysActa 1776: 86-107.
- Kennedy JC1, Pottier RH (1992) Endogenous protoporphyrin IX, a clinically useful photosensitizer for photodynamic therapy. See comment in PubMed Commons below J Photochem Photobiol B 14: 275-292.
- Malik Z1, Lugaci H (1987) Destruction of erythroleukaemic cells by photoactivation of endogenous porphyrins. See comment in PubMed Commons below Br J Cancer 56: 589-595.
- Kennedy JC, Pottier RH, Pross DC (1990) Photodynamic therapy with endogenous protoporphyrin IX: basic principles and present clinical experience. J Photochem Photobiol B 6:143?148.
- Dailey HA (1997) Enzymes of heme biosynthesis. J Biol Inorg Chem 2:411? 417.
- Ericson MB, Wennberg AM, Larkà O (2008) Review of photodynamic therapy in actinic keratosis and basal cell carcinoma. See comment in PubMed Commons below TherClin Risk Manag 4: 1-9.
- Plaetzer K, Kiesslich T, Oberdanner CB, Krammer B (2005) Apoptosis following photodynamic tumor therapy: induction, mechanisms and detection. See comment in PubMed Commons below Curr Pharm Des 11: 1151-1165.
- Morton CA, McKenna KE, Rhodes LE (2008) British Association of Dermatologists Therapy Guidelines and Audit Subcommittee and the British Photodermatology Group. Guidelines for topical photodynamic therapy: update. Br J Dermatol 159:1245?1266.
- Svanberg K, Andersson T, Killander D, Wang I, Stenram U, et al. (1994) Photodynamic therapy of non-melanoma malignant tumours of the skin using topical delta-amino levulinic acid sensitization and laser irradiation. Br J Dermatol 130:743?751.
- Dirschka T, Radny P, Dominicus R, Mensing H, Brüning H, et al.(2012) AK-CT002 Study Group. Photodynamic therapy with BF-200 ALA for the treatment of actinic keratosis: results of a multicentre, randomized, observer-blind phase III study in comparison with a registered methyl-5-aminolaevulinate cream and placebo. Br J Dermatol 166:137:146.
- Tyrrell JS, Morton C, Campbell SM, Curnow A (2011) Comparison of protoporphyrin IX accumulation and destruction during methylaminolevulinate photodynamic therapy of skin tumours located at acral and nonacral sites. Br J Dermatol 164:1362?1368.
- Ibbotson SH, Jong C, Lesar A, Ferguson JS, Padgett M, et al. (2006) Characteristics of 5-aminolaevulinic acid-induced protoporphyrin IX fluorescence in human skin in vivo. See comment in PubMed Commons below Photodermatol Photoimmunol Photomed 22: 105-110.
- Peng Q, Warloe T, Moan J, Godal A, Apricena F, et al. (2001) Antitumor effect of 5-aminolevulinic acid-mediated photodynamic therapy can be enhanced by the use of a low dose of photofrin in human tumor xenografts. Cancer Res 61:5824?5832.
- Juzeniene A, Juzenas P, Bronshtein I, Vorobey A, Moan J (2006) The influence of temperature on photodynamic cell killing in vitro with 5-aminolevulinic acid. See comment in PubMed Commons below J Photochem Photobiol B 84: 161-166.
- Orenstein A1, Kostenich G, Kopolovic Y, Babushkina T, Malik Z (1999) Enhancement of ALA-PDT damage by IR-induced hyperthermia on a colon carcinoma model. See comment in PubMed Commons below Photochem Photobiol 69: 703-707.
- Lopez RF, Bentley MV, Delgado-Charro MB, Salomon D, van den Bergh H, et al. (2003) Enhanced delivery of 5-aminolevulinic acid esters by iontophoresis in vitro. See comment in PubMed Commons below Photochem Photobiol 77: 304-308.
- Bremner JC, Adams GE, Pearson JK, Sansom JM, Stratford IJ, et al. (1992) Increasing the effect of photodynamic therapy on the RIF-1 murine sarcoma, using the bioreductive drugs RSU1069 and RB6145. See comment in PubMed Commons below Br J Cancer 66: 1070-1076.
- Berg K1, Anholt H, Bech O, Moan J (1996) The influence of iron chelators on the accumulation of protoporphyrin IX in 5-aminolaevulinic acid-treated cells. See comment in PubMed Commons below Br J Cancer 74: 688-697.
- Hanania J, Malik Z (1992) The effect of EDTA and serum on endogenous porphyrin accumulation and photodynamic sensitization of human K562 leukemic cells. See comment in PubMed Commons below Cancer Lett 65: 127-131.
- Liu HF1, Xu SZ, Zhang CR (2004) Influence of CaNa2 EDTA on topical 5-aminolaevulinic acid photodynamic therapy. See comment in PubMed Commons below Chin Med J (Engl) 117: 922-926.
- Malik Z, Kostenich G, Roitman L, Ehrenberg B, Orenstein A (1995) Topical application of 5-aminolevulinic acid, DMSO and EDTA: protoporphyrin IX accumulation in skin and tumours of mice. See comment in PubMed Commons below J Photochem Photobiol B 28: 213-218.
- Choudry K, Brooke RC, Farrar W, Rhodes LE (2003) The effect of an iron chelating agent on protoporphyrin IX levels and phototoxicity in topical 5-aminolaevulinic acid photodynamic therapy. See comment in PubMed Commons below Br J Dermatol 149: 124-130.
- 26.Fijan S, Honigsmann H, Ortel B (1995) Photodynamic therapy of epithelial skin tumours using delta-aminolaevulinic acid and desferrioxamine. See comment in PubMed Commons below Br J Dermatol 133: 282-288.
- Uehlinger P, Ballini JP, van den Bergh H, Wagnieres G (2006) On the role of iron and one of its chelating agents in the production of protoporphyrin IX generated by 5-aminolevulinic acid and its hexyl ester derivative tested on an epidermal equivalent of human skin. Photochem Photobiol 82:1069?1076.
- Ortel B1, Tanew A, Honigsmann H (1993) Lethal photosensitization by endogenous porphyrins of PAM cells--modification by desferrioxamine. See comment in PubMed Commons below J Photochem Photobiol B 17: 273-278.
- Smith AG1, Clothier B, Francis JE, Gibbs AH, De Matteis F, et al. (1997) Protoporphyria induced by the orally active iron chelator 1,2-diethyl-3-hydroxypyridin-4-one in C57BL/10ScSn mice. See comment in PubMed Commons below Blood 89: 1045-1051.
- Pye A1, Curnow A (2007) Direct comparison of delta-aminolevulinic acid and methyl-aminolevulinate-derived protoporphyrin IX accumulations potentiated by desferrioxamine or the novel hydroxypyridinone iron chelator CP94 in cultured human cells. See comment in PubMed Commons below Photochem Photobiol 83: 766-773.
- Blake E, Allen J, Curnow A (2013) The effects of protoporphyrin IX-induced photodynamic therapy with and without iron chelation on human squamous carcinoma cells cultured under normoxic, hypoxic and hyperoxic conditions. PhotodiagnosisPhotodynTher 10:575?582.
- Curnow A, McIlroy BW, Postle-Hacon MJ, Porter JB, MacRobert AJ, et al. (1998) Enhancement of 5-aminolaevulinic acid-induced photodynamic therapy in normal rat colon using hydroxypyridinone iron-chelating agents. Br J Cancer 78:1278?1282.
- Curnow A, MacRobert AJ, Bown SG (2006) Comparing and combining light dose fractionation and iron chelation to enhance experimental photodynamic therapy with aminolevulinic acid. See comment in PubMed Commons below Lasers Surg Med 38: 325-331.
- Porter JB, Abeysinghe RD, Hoyes KP, Barra C, Huehns ER, (1993) Contrasting interspecies efficacy and toxicology of 1,2-diethyl-3-hydroxypyridin-4-one, CP94, relates to differing metabolism of the iron chelating site. Br J Haematol 85:159-168.
- Campbell SM, Morton CA, Alyahya R, Horton S, Pye A, et al. (2008) Clinical investigation of the novel iron-chelating agent, CP94, to enhance topical photodynamic therapy of nodular basal cell carcinoma. See comment in PubMed Commons below Br J Dermatol 159: 387-393.
- Pye A, Campbell S, Curnow A (2008) Enhancement of methyl-aminolevulinate photodynamic therapy by iron chelation with CP94: an in vitro investigation and clinical dose-escalating safety study for the treatment of nodular basal cell carcinoma. J Cancer Res ClinOncol 134:841?849.
- Bedwell J, MacRobert AJ, Phillips D, Bown SG (1992) Fluorescence distribution and photodynamic effect of ALA-induced PP IX in the DMH rat colonic tumour model. See comment in PubMed Commons below Br J Cancer 65: 818-824.
- Loh CS, Vernon D, MacRobert AJ, Bedwell J, Bown SG, Brown SB (1993) Endogenous porphyrin distribution induced by 5-aminolaevulinic acid in the tissue layers of the gastrointestinal tract. J Photochem Photobiol B: Biol20:47-54.
- Robinson DJ, de Bruijn HS, van der Veen N, Stringer MR, Brown SB, et al. (1998) Fluorescence photobleaching of ALA-induced protoporphyrin IX during photodynamic therapy of normal hairless mouse skin: the effect of light dose and irradiance and the resulting biological effect. Photochem Photobiol 67:140?149.
- Robinson DJ1, de Bruijn HS, van der Veen N, Stringer MR, Brown SB, et al. (1999) Protoporphyrin IX fluorescence photobleaching during ALA-mediated photodynamic therapy of UVB-induced tumors in hairless mouse skin. See comment in PubMed Commons below Photochem Photobiol 69: 61-70.
- Szeimies RM1, Calzavara-Pinton P, Karrer S, Ortel B, Landthaler M (1996) Topical photodynamic therapy in dermatology. See comment in PubMed Commons below J Photochem Photobiol B 36: 213-219.
- Peng Q1, Warloe T, Berg K, Moan J, Kongshaug M, et al. (1997) 5-Aminolevulinic acid-based photodynamic therapy. Clinical research and future challenges. See comment in PubMed Commons below Cancer 79: 2282-2308.
- Curnow A, Tyrrell J (2015)The mechanism of action of topical dermatological photodynamic therapy. In: Hugo A, ed. Photodynamic therapy: Fundamentals, applications and health outcome effects. New York: Nova Science 59-102.
- Stringer M, Collins P, Robinson D, Stables G, Sheehan-Dare R (1996) The accumulation of protoporphyrin IX in plaque psoriasis after topical application of 5-aminolaevulinic acid indicates a potential for superficial photodynamic therapy. J Invest Dermatol 107:76-81.
- Peng Q, Berg K, Moan J, Kongshaug M, Nesland JM (1997) 5-Aminolevulinic acid-based photodynamic therapy: principles and experimental research. See comment in PubMed Commons below Photochem Photobiol 65: 235-251.
- Flora SJ (2009) Structural, chemical and biological aspects of antioxidants for strategies against metal and metalloid exposure. See comment in PubMed Commons below Oxid Med Cell Longev 2: 191-206.
- Ryter SW, Alam J, Choi AM (2006) Heme oxygenase-1/carbon monoxide: from basic science to therapeutic applications. See comment in PubMed Commons below Physiol Rev 86: 583-650.
- Sutton HC1, Winterbourn CC (1989) On the participation of higher oxidation states of iron and copper in Fenton reactions. See comment in PubMed Commons below Free Radic Biol Med 6: 53-60.
- Curnow A, Pye A (2015)The importance of iron chelation and iron availability during PpIX-induced photodynamic therapy. Photonics & Lasers in Medicine 4:39-58.
- Sorg O1 (2004) Oxidative stress: a theoretical model or a biological reality? See comment in PubMed Commons below C R Biol 327: 649-662.
- Zhong JL1, Yiakouvaki A, Holley P, Tyrrell RM, Pourzand C (2004) Susceptibility of skin cells to UVA-induced necrotic cell death reflects the intracellular level of labile iron. See comment in PubMed Commons below J Invest Dermatol 123: 771-780.
- Valko M1, Rhodes CJ, Moncol J, Izakovic M, Mazur M (2006) Free radicals, metals and antioxidants in oxidative stress-induced cancer. See comment in PubMed Commons below Chem Biol Interact 160: 1-40.