Abdurrahman Sönmezler1* and Şakir Özgür Keşkek2
1Department of Neurology, Adana City Research and Training Hospital, Adana, Turkey
2Department of Internal Medicine, Adana City Research and Training Hospital, Adana, Turkey
*Corresponding Author:
Abdurrahman Sönmezler
Assistant Professor
Department of Neurology
Adana City Research and Training Hospital, Adana, Turkey
Tel: +905323951977
E-mail: sonmezlera@gmail.com
Received Date: February 05, 2019; Accepted Date: March 04, 2019; Published Date: March 11, 2019
Citation: Sönmezler A, Kekek SO (2019) Dysphagia in Patients with Acute Ischemic Stroke in a Tertiary Care Hospital. J Intensive Crit Care Vol.5 No. 1:8
Objective: The aim of this study was to investigate the frequency of dysphagia in acute ischemic stroke and relation with Glasgow Coma Score (GCS).
Methods: The data of 54 patients with acute ischemic stroke were retrospectively analyzed. Glasgow Coma Scores were recorded. Modified Massey Bedside Swallow Screen (MBSS) was used for the diagnosis of dysphagia. For statistical evaluation MedCalc 15.8 software program (MedCalcBelgium) was used.
Results: Fifty-four patients (n: 54) with acute ischemic stroke who were admitted to the study were followed up in our hospital Neurology Intensive Care Unit (NICU). Fortynine of the patients were alive, transferred to our service, then discharged. Twenty-six patients had dysphagia (48.1%) while 28 patients did not have dysphagia (51.9%). Glasgow Coma Scores were lower in patients with dysphagia (r=-0.628, p<0.0001. Moreover, survival was inversely correlated with dysphagia (r=-0.331, p= 0.014).
Conclusions: Swallowing disorders can be associated with adverse clinical outcomes in patients with acute ischemic stroke in intensive care unit. It is also associated with survival and GCS. Dysphagia is common in ICU patients and should be carefully diagnosed since it can be an independent predictor of death.
Keywords
Acute ischemic stroke; Dysphagia; Glasgow Coma Score
Introduction
Swallowing is a complex function resulting from dysfunctions of the oral, pharynx, larynx, oesophagus, and respiratory muscles with other structures [1]. A swallowing disorder or decrease in swallowing ability is called dysphagia [2]. Dysphagia can be a life-threatening symptom in patients with stroke. Stroke has been the second most common cause of death and third most common cause of disability in the world [3,4]. People who have suffered stroke are susceptible to multiple complications. Most of complications can recover within a few week but complications of dysphagia can continue. Dysphagia is a common complication that affects 76% of patients in stroke patients. It may persist for up to 6 months [5,6]. Stroke is the most common cause of neurogenic oropharyngeal dysphagia [7]. Dysphagia is a common morbidity after stroke, but widely different frequencies have been reported [8]. Dysphagia can cause aspiration pneumonia, dehydration, malnutrition and decreased functional independence [9]. The swallowing function is indispensable for life. It is known to be a complex procedure that requires voluntary and involuntary coordination of more than 40 pairs of muscles and several cranial nerves [10]. Many areas of the brain, especially the brain stem, thalamus, basal ganglia, cerebellum and motor and sensory cortex, associated with spontaneous and involuntary control of swallowing [11,12]. On the other hand cerebral lesions may block voluntary chewing control and bolus transport during the oral phase. Lesions of the pre-central gyrus may provide contralateral disruption in the face, lip and tongue motor control, and contralateral weakness in pharyngeal peristalsis. In case of cognitive functions impairment due to the cerebral lesions, such as concentration or selective attention also cause of disruption of swallowing control. Brainstem lesions are less common but reason of the largest swallowing weakness. These lesions may affect sensation of the mouth, tongue, and cheek, timing in the trigger of the pharyngeal swallow, laryngeal elevation, glottic closure and cricopharyngeal relaxation [13,14]. In this study, 54 patients with acute ischemic stroke were investigated for the presence of dysphagia and its association with GCS and survival.
Materials and Methods
This study was performed at Adana City Training and Research Hospital between September 2017 and Jun 2018. A total of 54 patients with acute ischemic stroke were included in this retrospective study. Patients who stayed at least 24 hours in NICU were included the study. Patients with haemorrhagic stroke, progressive neurological disease, tubal intubation and previously existing situations were excluded from the study. Additionally patients with a history of any gastrointestinal tract disease, pregnant or lactating women were also excluded. Finally, 54 patients were recruited due to the having enough alertness level and ability to process further for swallowing evaluation. To assess the ability to swallow safely a standardized screener that is Modified Massey Bedside Swallow Screen (MBSS) was used. In all cases, measurements were taken of the participants’ glucose, lipids, AST, ALT, creatinine levels and complete blood counts. Glucose, lipids, ASTs, ALTs, creatinine levels were analysed on the Beckman Coulter Synchron LX 20 (Massachusetts, USA). Complete blood counts were measured by on the Sysmex XE 2100i (Japan). For statistical evaluation MedCalc 15.8 software program (MedCalcBelgium) was used. Mean standard deviation values of the data were recorded. The Student's t-test was used to compare normal quantitative independent data and the Mann-Whitney U-test was used to compare independent quantitative data without normal distribution. Pearson or Spearman's correlation coefficient was used to analyse the degree of association between two variables. A log transformation was used for the variables that were not normally distributed. Chi-square test was used to compare qualitative data. Data were assessed at 95% confidence interval and p<0.05 values were considered as significant. Multiple regression tests (backward method) were used to analyse the relationship between a dependent variable and one or more independent variables (predictor variables or explanatory variables).
Result
A total of 54 patients (n: 54) with acute ischemic stroke who were admitted to the study were followed up in our hospital Neurology Intensive Care Unit (NICU). Forty-nine of the patients were alive, transferred to our service, then discharged. Twentysix patients had dysphagia (48.1%) while twenty-eight of them did not have dysphagia (51.9%). Demographic data and biochemical values of the groups were shown on Table 1.
| |
Dysphagia (+) |
Dysphagia (-) |
p |
| Age (year) |
69.7 ± 11.9 |
70.8 ± 9.5 |
0.697 |
| Female N (%) |
16 (59.3%) |
12 (46.2%) |
0.442 |
| Glasgow Coma Score |
13.0 ± 0.19 |
13.8 ± 0.72 |
<0.001 |
| Ex N (%) |
5 (19.2%) |
0 |
0.02 |
Table 1 shows characteristics of the groups
The mean age of the patients with dysphagia was 69.7 ± 11.9 and it was 70.8 ± 9.5 in patients without dysphagia (p=0.697). Female/male ratio was 14/12 in dysphagia group while it was 11/17 in the control group (p=0.288). The mean GCS was low in patients with dysphagia (13.0 ± 0.19 vs. 13.8 ± 0.72, p<0.001). A negative correlation was found between GCS and presence of dysphagia (r=-0.628, p<0.0001) (Figure 1).
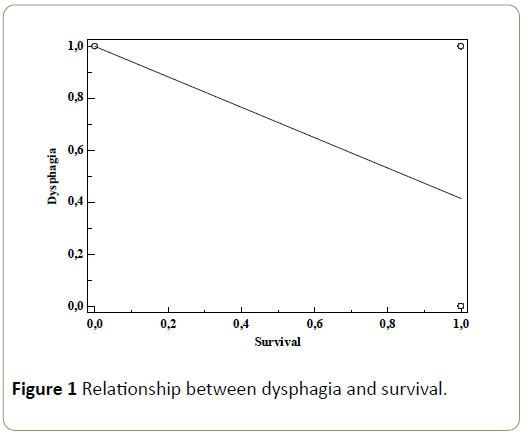
Figure 1: Relationship between dysphagia and survival.
The frequency of dysphagia was also low in survived patients (r=-0,331, p=0.014) (Figure 2). Multiple regression analyses (backward method) were performed with dysphagia as a dependent variable and with age, gender, and GCS, magnesium and lesion localization as independent variables. A significant correlation persisted between GCS and lesion localization (p<0.001, respectively) (Table 2 and Figure 3).
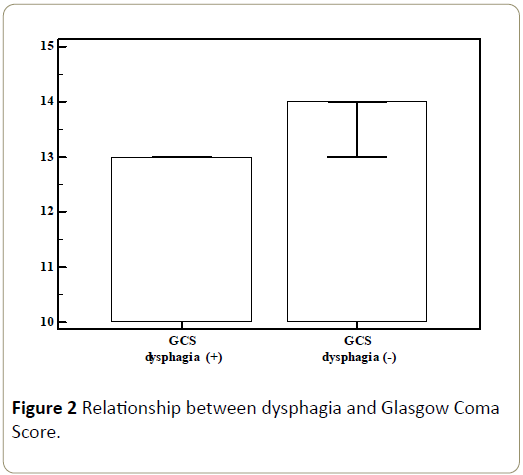
Figure 2: Relationship between dysphagia and Glasgow Coma Score.
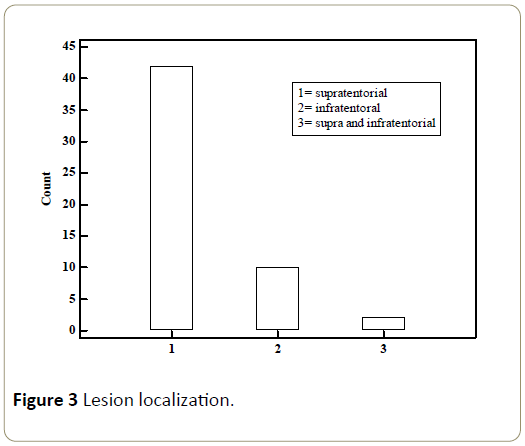
Figure 3: Lesion localization.
| Classification X |
Lesion localization count |
| Supratentorial |
42 |
77.80% |
| Infratentorial |
10 |
18.50% |
| Supra and Infratentorial |
2 |
3.70% |
| Total |
54 |
100.00% |
| Chi-squared test |
| Chi-squared |
49,778 |
| DF |
2 |
| Significance level |
P<0.0001 |
Table 2 Lesion localization.
Discussion
In this study, we investigated the frequency of dysphagia in patients with acute ischemic stroke in our NICU. We also analysed its association with GCS and survival. We have diagnosed dysphagia in an important part of the patients. Patients with dysphagia had lower GCS and survival rate. An important part of acute stroke management is detection of dysphagia. Literature suggested that swallowing difficulties can affect variable percentage of patients. Its incidence varies in different studies that may depends on the different screening procedure used, or be related to lesion localization. Dysphagia after stroke is an indicator of persistent disability, increased risk of chest infection, prolonged hospital stay, malnutrition, poor prognosis and mortality. The literature reported that frequency of dysphagia in the acute stroke is variable, ranging from 13% 100% especially to Wallenberg's syndrome. According to studies that dysphagia is common in stroke patients. Although its incidence is different which is because of different screening methods, it can persist for a long time and may affect morbidity and mortality [15-21]. Hamidon et al. [22] reported that 41% of patient had dysphagia in their study. Ickenstein et al. [23] concluded that 21/50 (42%) patients had post-stroke dysphagia during their hospital course. The Glasgow Coma Score is generally used as a measure of the level of consciousness. Low Glasgow Coma Score affects swallowing function in a negative way. This situation a natural consequence of a reduction in cognitive status. Stroke related aspirations are believed to be due to dysphagia result of aspiration of oropharyngeal material or gastric content after brain injury. Studies reported that dysarthria can cause mental stress and may increase gastric acid secretion. Stress-related mucosal diseases and ulcers may be the cause of acid aspiration. Acute stroke is regularly accompanied by dysphagia, impaired consciousness and other factors that lead to malnutrition. Due to unconsciousness and difficulty in swallowing, acute stroke patients are at great risk for acute respiratory distress syndrome associated with high mortality [24]. We have diagnosed dysphagia in 48.1% of the patients. Moreover, we were observed an inversely correlation between dysphagia and survival in our study. This situation was predictable and not surprising for us. Even more compatible with literature findings [25].
Crary et al. [26] concluded that there was significant differences between GCS score of patient had dysphagia and patients did not have dysphagia (GCS: dysphagia subgroup: 13.4, no dysphagia subgroup: 14.8). The results of Crary and colleagues were similar but only 69 patients were included in their study. In addition, only 39 were ischemic strokes. The number of patients was limited (72 patients) in another study that Ikenaga et al. [27] was found Glasgow Coma Scale lower in patients with difficulty in oral intake. Brogan et al. [28] concluded that mild GCS disorder was statistically significant with dysphagia according to normal. They received ischemic and haemorrhagic total 378 cases. In our study which consisted of only ischemic cases, we saw such a result. We observed that dysphagia decreased as Glasgow Coma Score increased (r=-0.628, p<0.0001).
There were limitations and shortcomings in this study. The data of 54 patients with acute ischemic stroke were retrospectively analysed. Number of cases was not enough. Only intensive care processes were evaluated. More precise techniques such as video fluoroscopy could not be used.
Conclusion
Swallowing disorders can be associated with adverse clinical outcomes in patients with acute ischemic stroke in intensive care unit. It is also associated with survival and GCS. Dysphagia is common in ICU patients and should be carefully diagnosed since it can be an independent predictor of death. The presence of swallowing difficulties must be recognized early and meticulously. In some patients, swallowing difficulties may persist for too long. This condition, which can affect morbidity and mortality, should be managed very well.
Acknowledgement
The authors have no financial or personal relationships with other people or organizations that could pose a conflict of interest in connection with the present work.
References
- De Pauw A, Dejaeger E, D'hooghe B, Carton H (2002) Dysphagia in multiple sclerosis. Clin Neurol Neurosurg 104: 345-351.
- Tassorelli C, Bergamaschi R, Buscone S, Bartolo M, Furnari A, et al. (2008) Dysphagia in multiple sclerosis: from pathogenesis to diagnosis. Neurol Sci Suppl 4: S360-363.
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, et al. (2012) Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380: 2095-2128.
- Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, et al. (2012) Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380: 2197-2223.
- Schelp AO, Cola PC, Gatto AR, Silva RG, Carvalho LR (2004) Incidence of oropharyngeal dysphagia associated with stroke in a regional hospital in São Paulo State - Brazil. Arq Neuropsiquiatr 62: 503-506.
- Smithard DG, O'Neill PA, Parks C, Morris J (1996) Complications and outcome after acute stroke. Does dysphagia matter? Stroke 27: 1200-1204.
- Wiles CM (1991) Neurogenic dysphagia. J Neurol Neurosurg Psychiatry 54:1037–1039.
- Meng NH, Wang TG, Lien IN (2000) Dysphagia in patients with brainstem stroke: incidence and outcome. Am J Phys Med Rehabil 79: 170-175.
- Ickenstein GW, Kelly PJ, Furie KL, Ambrosi D, Rallis N, et al. (2003) Predictors of feeding gastrostomy tube removal in stroke patients with dysphagia. J Stroke Cerebrovasc Dis 12: 169-174.
- Daniels SK, Foundas AL, Iglesia GC, Sullivan MA (1996) Lesion site in unilateral stroke patients with dysphagia. J Stroke Cerebrovasc Dis 6: 30-34.
- Zald DH, Pardo JV (1999) The functional neuroanatomy of voluntary swallowing. Ann Neurol 46: 281-286.
- Daniels SK, Brailey K, Foundas AL (1999) Lingual discoordination and dysphagia following acute stroke: analyses of lesion localization. Dysphagia 14: 85-92.
- Veis SL, Logemann JA (1985) Swallowing disorders in persons with cerebrovascular accident. Arch Phys Med Rehabil 66: 372-375.
- Martino R, Terrault N, Ezerzer F, Mikulis D, Diamant NE (2001) Dysphagia in a patient with lateral medullary syndrome: insight into the central control of swallowing. Gastroenterology 121: 420-426.
- Hines S, Kynoch K, Munday J (2013) Identification and nursing management of dysphagia in individuals with acute neurological impairment: a systematic review protocol. JBI Database of Systematic Reviews and Implementation Reports. 11: 312-323.
- DePippo KL, Holas MA, Reding MJ, Mandel FS, Lesser ML (1994) Dysphagia therapy following stroke: a controlled trial. Neurology 44: 1655-1660.
- Kuhlemeier K, Rieve J, Kirby N, Siebens A (1989) Clinical correlates of dysphagia in stroke patients. Arch Phys Med Rehabil 70: A56.
- Currier RD, Giles CL, Dejong RN (1961) Some comments on Wallenberg’s lateral medullary syndrome. Neurology 11: 778-791.
- Kameda W, Kawanami T, Kurita K, Daimon M, Kayama T, et al. (2004) Lateral and medial medullary infarction: a comparative analysis of 214 patients. Stroke 35: 694-699.
- Sacco RL, Freddo L, Bello JA, Odel JG, Onesti ST, et al. (1993) Wallenberg's lateral medullary syndrome. Clinical-magnetic resonance imaging correlations. Arch Neurol 50: 609-614.
- Hughes SM (2011) Management of dysphagia in stroke patients. Nurs Older People 23: 21-24.
- Hamidon BB, Nabil I, Raymond AA (2006) Risk factors and outcome of dysphagia after an acute ischaemic stroke. Med J Malaysia 61: 553-537.
- Ickenstein GW, Stein J, Ambrosi D, Goldstein R, Horn M, et al. (2005) Predictors of survival after severe dysphagic stroke. J Neurol 252: 1510-1516.
- Zhao JN, Liu Y, Li HC (2015) Aspiration-related acute respiratory distress syndrome in acute stroke patient. PLoS One 10: e0118682.
- Patel DA, Krishnaswami S, Steger E, Conover E, Vaezi MF, et al. (2018) Economic and survival burden of dysphagia among inpatients in the United States. Dis Esophagus 31: 1-7.
- Crary MA, Carnaby GD, Sia I, Khanna A, Waters MF (2013) Spontaneous swallowing frequency has potential to identify dysphagia in acute stroke. Stroke 44: 3452-3457.
- Ikenaga Y, Nakayama S, Taniguchi H, Ohori I, Komatsu N, et al. (2017) Factors Predicting Recovery of Oral Intake in Stroke Survivors with Dysphagia in a Convalescent Rehabilitation Ward. J Stroke Cerebrovasc Dis 26: 1013-1019.
- Brogan E, Langdon C, Brookes K, Budgeon C, Blacker D (2014) Respiratory infections in acute stroke: nasogastric tubes and immobility are stronger predictors than dysphagia. Dysphagia 29: 340-345.

