Keywords
Digital Health; Health rhetoric; Thematizing; Transcribing; Ethnic groups
Introduction
Digital health technologies are described as promoting communication between healthcare providers and patients, encouraging lay people to engage in preventive health activities and improving patient adherence to treatment protocols and their self-management of chronic diseases [1-4]. This research pursues how digital health information is consumed and is useful for in Nepal and, second, how it affects doctor-patient communication in Nepal. With the sudden explosion of digital media content and access devices in the last generation, there is now more information available to more people from more sources than at any time in human history [1]. But the innovations in care delivery also could exacerbate disparities in access to care across racial/ethnic or economic groups or between the technologically sophisticated and native [2].
Health care providers are beginning to deliver a range of internetbased services to patients; however, it is not clear which of these digital health services patients need or desire [3]. This research will dig out what kinds of digital resources do the doctors in the Nepalese hospitals use to cater better care, and whether or not telemedicine is the alternative to digital health. Though the research site is in Nepal, the findings can imply to the global contexts.
In many parts of the world, hitherto local healing methods are more popular, health education is still expensive and technology very scarce. Even in urban areas relation between patients and doctors is not reciprocal as the latter always have upper hand in medication. Either the communication between patient and health staffs is very less or ineffective. “In the doctor’s office, the patient is not only an ill person or a person with a complaint; he or she is also an interlocutor in a persuasive encounter in which the reward of credibility may be best care, and the price of lack of credibility may be more sickness or pain” [5].
Significance
Because of time constraints, medical jargon, and emotion are all in the mix, communication between a doctor and patient may ripe for misunderstanding. Many times digital health information is sought to find the remedies of the illness that the family or friends have been suffering from, it is very difficult to get the accurate remedies. This led to do research on this topic so that in future many patients and the policy makers will be benefited by this research. Therefore, the study does have the importance and relevance to Nepal and then to other countries around the world, and the researcher has scrutinized digital health with the help of the respondents (15 male and 15 female doctors).
Literature reviews
While doctors may feel that digital health slow them down, interfere with face-to-face care, and intrude upon their patient relationships, patients do not see it that way. The survey done elsewhere found sixty nine percent of people have noticed a difference in the amount of technology being used by their doctor over the last five years, and ninety seven percent are comfortable with it, most notably desktop computers or laptops, followed by mobile devices such as a tablet or smartphone, telemedicine and image-sharing in Germany [6]. Additionally, fifty eight percent of people feel the use of technology in the exam room positively affects their healthcare experience. As technology adoption trends continue to rise, patients will be exposed to more types of tools, which may impact their comfort levels. For instance, EHR deployments have made laptops and desktop computers a standard piece of equipment in the modern-day exam room, and patient comfort levels reflect this acclamation.
To quote Clark and Harrison again, “According to patients, the use of health technology as a collaborative tool in the exam room adds value to their experience, however nearly three-quarters of people do not use a patient portal to access their personal health information”. In a decade, the widespread adoption of computers, new internet technology, and other software has changed health rhetoric. There are significant changes in the ways in which people obtain health information, and the way they communicate about health in their daily life. New technologies will continue to develop and impact hugely in the way people make health care decisions.
The internet has become a common tool for providers to communicate with other providers, for patients to receive social supports and for health campaign designers to reach a large number of audiences with a peculiar health oriented messages. However, not all people have access to the Internet on the skills to use it. The ability to cash the available health information is still depressingly low. Digital health—here, the public use of information Web sites to facilitate decision making on matters of health and illness—is a rhetorical practice, involving text and trajectories of influence [5]. A fulsome account of it requires attention to all parts of the rhetorical triangle—the speaker, the subject matter, and the audience—yet most scholarship on digital health focus on the speaker only: it typically raises concerns primarily about the dangers of unreliable sources, suggesting that, where speakers are reliable and information is accurate, digital health simply empowers patients.
It is suggested for patients who are already connected to the Internet; health care providers should be prepared to offer suggestions for Web-based health resources and to assist patients in evaluating the quality of medical information available on the World Wide Web [7]. I agree with Judy Segal that the Internethealth user is not simply a rational health consumer, abstracted from culture and from history, and digital health is part of a discursive field with interlocking roles and genres, agents and actions. There are so many modes and issues available online today. Segal further clarifies digital health the following way:
“Digital health” (sometimes “cybermedicine” or “digital health”) refers in different contexts to different activities including, among others, accessing electronic health records, consulting doctors by e-mail, shopping online for pharmaceuticals, and blogging about illness experience. In this essay, I use the term to refer to a single online practice: visiting health-information Web sites in advertisements of making decisions about one’s own and one’s family’s care.
Nonetheless, the Internet clearly is an important tool with the potential to improve information dissemination and perhaps to improve health care delivery and outcomes [8]. Continuing efforts to maximize the potential of this tool could have great value. While some rhetorical critics are specifically trained in rhetorical history, theory, and analysis, scholars from many disciplines play a role in forming and elaborating a rhetorical view of the theory and practice of medicine [9]. Some researchers have observed that online health information is also not patient friendly. Patients tended to give higher ratings to the quality of health information on the Internet. Other researchers also debunk the notion that technology boosts health communication:
Improved technology is not the answer to making better use of this enticing resource. We need to be clearer about the web's clinical role and the evaluation problems that it raises—how to recruit suitable subjects, develop valid and reliable methods of measurement, and carry out many more rigorous evaluations [10].
This raises a concern, “As we recently noted, that patients using the Web for medical information may have difficulty “finding complete and accurate information [11].” They suggested that deficiencies with health information online may “negatively influence” patients' decisions [7]. It is something patients have grumbled about for a long time. Doctors are rude. Doctors don't listen. Doctors have no time. Doctors don't explain things in terms patients can understand [12]. Numerous debates have been on how to best communicate in health institutions:
The “art of medicine” has been the topic of much discussion but has never been subjected to scientific scrutiny. Whereas other aspects of medical practice are included in the doctor’s training, the approach to the patient is expected to be on the basis of intuition, and it is traditionally learned only by precept and by experience [13].
That the Health Information National Trends Survey data portray a tectonic shift in the ways in which patients consume health and medical information, with more patients looking for information online before talking with their doctors [14]. Relevant government bodies need to support service providers who embrace change and do not fall back on dislocated, isolated and expensive feefor- service models [15]. In a research conducted suggests how patients who choose to explicitly share health data within a community may benefit from the process, helping them engage in dialogues that may inform disease self-management [16].
It has been shown that a low-cost telemedicine link is technically feasible, is of great educational value, and can be of a great beneï¬ÂÂÂÂt for the diagnosis and management of medical conditions in Nepal [17]. It can readily be emulated elsewhere in the developing world. However, in a developing country like Nepal, digital health can impact differently, and be more in/appropriate, because social hierarchy is more prominent and more generally accepted here.
Method
The full-scale administration of the survey is conducted to estimate the reliability and validity of the mechanism.
The independent variables
The independent variables are gender, age, qualification, and years of experience. This project trialed of the research method first at Dhulikhel Hospital, Kavre to ensure that the research design is feasible, and will provide the information required. For the study first, it is carefully considered if the online forum could be the best data collection method for their research questions. Second, the characteristics of my participants are contemplated. Third, computer and Internet jargons are defined before starting an online forum discussion so that consistent definitions for the jargon can be used throughout the research process.
Data management
Next decision is how to deal with the automatic transcripts from the online forum site and/or databases before starting the online forum discussion. Finally, potential security issues throughout the data collection process are considered, and carefully monitored online interactions.
Online survey and field notes
They suggest that whilst previously we often conduct interviews because direct observation was too difficult and time consuming, the Internet has now made acquiring observational data less laborious than interviews [18]. There are many benefits of online research methods. However, cautionary notes include the need to establish ethical grounds for accessing online data, and the possibly of various forms of bias shaping the data [18]. The online form is developed according to the justification by Im and Chee [19]. For the study, data are collected for the study from a number of sources as web-based questionnaires could replace traditional paper questionnaires with minor effects on response rates and lower costs [20]. Using data from websites, forums and social networking sites continues a long tradition of unobtrusive methods in social research.
A working manual for use by the interviewer is prepared. In the field, completed questionnaires are reviewed for completeness, accuracy and legibility at the end of each day. The interviewer solves specifically for mismatched age and gender of participants and the information from the participants. When minor mistakes are seen, it is corrected after discussion with the interviewer; major mistakes or missing data are corrected by revisiting the respondent. Then, the following devices are considered as per the need to take their interviews: Face to face method. Kvale Steinar draws a similar distinction between the research question and the interview question (Figure 1).
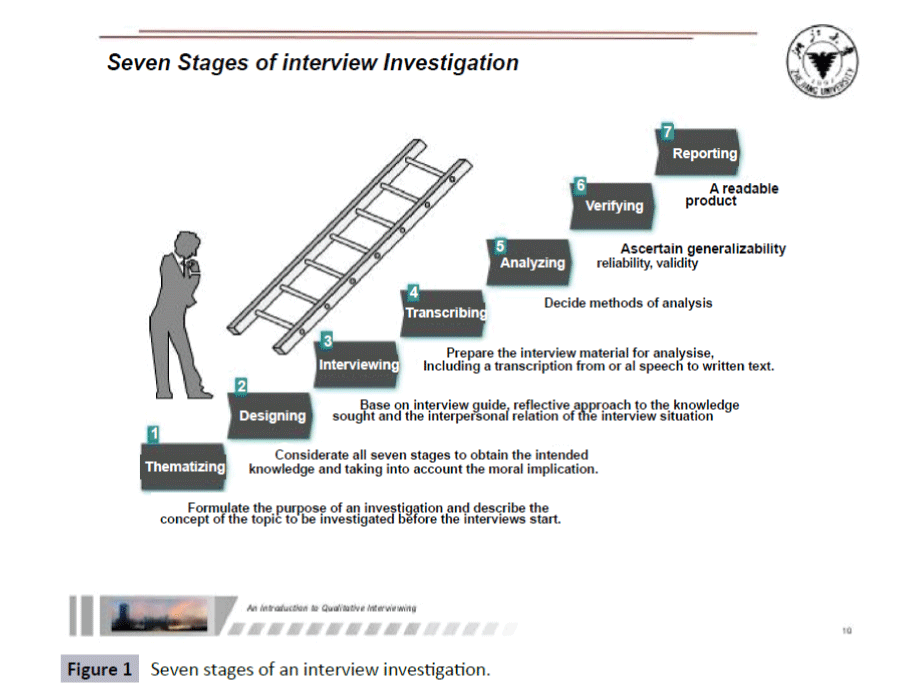
Figure 1: Seven stages of an interview investigation.
These are presented through the seven stages of an interview investigation [21]:
Thematizing: Formulate the purpose of the investigation and describe the concept of the topic to be investigated before the interviews start.
Designing: Plan the design of the study, taking into consideration all seven stages, before the interview starts.
Interviewing: Conduct the interviews based on an interview guide and with a reflective approach to the knowledge sought.
Transcribing: Prepare the interview material for analysis, which commonly includes a transcription from oral speech to written text.
Analyzing: Decide, on the basis of the purpose and topic of the investigation, and on the nature of the interview material, which methods of analysis are appropriate.
Verifying: Ascertain the generalizability, reliability, and validity of the interview findings. Reliability refers to how consistent the results are, and validity means whether an interview study investigates what is intended to be investigated.
Reporting: Communicate the findings of the study and the methods applied in a form that lives up to scientific criteria, takes the ethical aspects of the investigation into consideration, and that results in an readable product. The choice of data collection procedures should be guided by the research question and the choice of design. However, the choice of data collection methods is also subject to constraints in time, financial resources, and access.
Interview with one participant is effective for this study as it is a sensitive topic. So in case of in-depth interview, my respondents’ views are recorded (whenever it is impractical, field notes are taken too). Then, it is transcribed.
Respondents, questionnaire and sites
First, a survey is taken on thirty doctors working in different (Government, Teaching, Missionary, Community and Private) hospitals of Nepal. Then survey of 300 outpatients of chronic diseases is done. In the survey each respondent is asked to rate each questionnaire on a response scales. They can rate each item on a 1-to-5 response scale where:
1: Strongly disagree
2: Disagree
3: Undecided
4: Agree
5: Strongly agree
However, for the open ended questions, they have to compose their responses. For purposeful (or purposive) sampling, a clear purpose is taken as it needed to define which patient or doctor fit with the goals. The researcher plan to survey about 45 doctors, out of them, 30 can turn up to help in this research. Moreover, the researcher request 20 doctors and 20 patients for the interviews that would take place after a month. The data are valid for this research.
While doing the main survey, the questionnaires are used to explore perceptions of doctors, and Patients regarding the use of digital health resources. Each questionnaire is about their perceptions of online health information. The first draft of questionnaire is prepared and handed over to the experts and doctors for comments and amendments. Data are being collected over one-month period, and a reminder letters are sent to those who have not yet responded. Hospitals are selected from 5 representative districts out of 75 in the country.
As the main task in interviewing is to understand the meaning of what the interviewees say, the researcher uses semi-structured and structured questionnaires, and in-depth interviews to collect the data. For survey and field notes, the researcher will store all completed questionnaires safely in a plastic-coated envelop at the end of each day. After completion of data collection, they are sealed in a plastic bag and brought back to my home. The recordings are first transferred to the interviewer's laptop via Bluetooth, and then those are copied on a CD to send to me by the courier. Finally, the researcher will enter, transcribe and translate the data with the help of two linguists. Double checking of entries is made, with inconsistencies reconciled by reference to the original documents.
Possible biases
To avoid the possible biases, the questionnaires go to the dual reviews—having two expert reviewers independently assess the questions that is one method of reducing the risk of biased decisions on study inclusion, as is recommended in the Institute of Medicine's “What works in healthcare: standards for systematic reviews.” The dual review will be done at each stage to reduce the potential for random errors and bias. Reviewers will compare decisions and will resolve differences through discussion, consulting a third party when consensus cannot be reached. The third party will be an experienced senior reviewer.
Scientific conduct
The researcher would obtain the Ethical Approval from Nepal Health Research Council (NHRC), an apex body of Ministry of Health and Population having shown a solid and feasible framework of this research. There are no instances of plagiarism.
Analysis
“The more you communicate, the healthier people get and the more knowledgeable doctors become. Without open lines of communication, important details can be missed, patients might put off appointments for too long and trust can’t be built” [22]. Doctors who are working in the rural hospitals and are more likely to need digital health materials tended to use the new digital health less frequently compared with doctors working in big hospitals in the cities. Honest patient feedback is certainly valuable information for a doctor or clinic whether or not it’s posted online (Chart 1) [22].
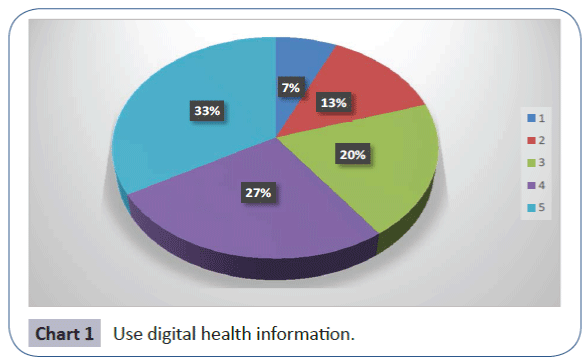
Chart 1: Use digital health information.
Over the coming decade, face-to-face patient/doctor contacts will become less common and exchanges between consumers and providers will increasingly be mediated by electronic devices [23]. With digital health and awareness in patients, not only is there communication between doctors with doctors, but also patient-patient communication. Now many cases and rich digital health resources are available on the Internet. The substantial amount of health-related information available on the Internet little is known about the accessibility, quality, and reading grade level of that health information.
Similarly Gunther Eysenbach [24] reveals browsing the site, users frequently posted their remarks on one another’s profiles, in some cases sharing their own relevant experience. “Those who searched online the most tended to be younger, women, and better educated, and tended to have higher incomes than those who searched the least” [14]. Therefore, the researcher wants to research on a rhetorical view of advice and adherence suggests the usefulness of a negotiation of expertise [5] available on the Internet in terms of ethos, logos and pathos (Chart 2).
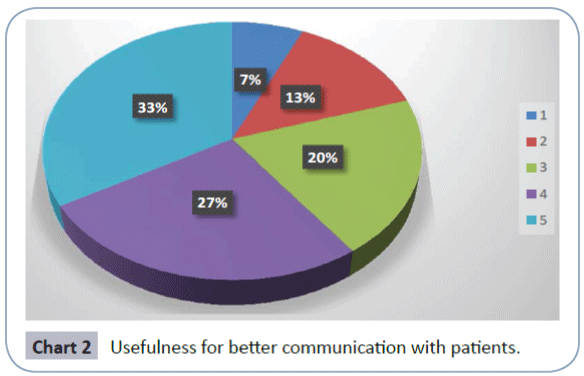
Chart 2: Usefulness for better communication with patients.
The Internet clearly is an important tool with the potential to improve information dissemination and perhaps to improve health care delivery and outcomes. Continuing efforts to maximize the potential of this tool could have great value [8]. However, Hickie et al. [15] think variability in both content and quality of medical information to the public is not exclusive of the internet, as wide differences also exist in other forms of public communication, such as print and broadcast media.
Like Diaz et al. [7] suggest for patients who are already connected to the Internet, health care providers should be prepared to offer suggestions for Web-based health resources and to assist patients in evaluating the quality of medical information available on the World Wide Web. I agree with Judy Segal [25] that the Internet-health user is not simply a rational health consumer, abstracted from culture and from history, and digital health is part of a discursive field with interlocking roles and genres, agents and actions. There are so many modes and issues available online today. Results of the doctors' thoughts that they use online resources to diagnose and treat the patient's diseases are promising. Forty-two percentages agree and 12.5 percentages of the doctors strongly agree that they use online resources to diagnose and treat the patient's diseases. However, 12.5 percentages strongly disagree and 33.3 percentages disagree on that (Chart 3).
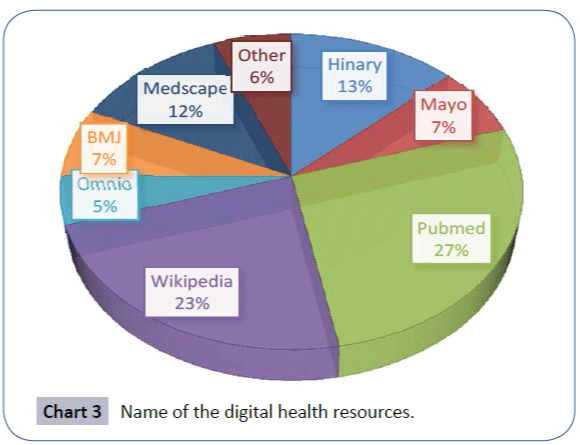
Chart 3: Name of the digital health resources.
Regarding the use of digital health information, the doctors opted for HINARI (13%), Mayo (7%), Pubmed (27%), Wikipedia (23%), Omnio (5%), BMJ (7%) online, various medical sites including Medscape (12%), and anything available on other resources (3%). They use those since such online data help them remove their queries regarding certain health problems or in some confusing cases and help them make a better diagnosis and opt for the best treatment available. With a long experience and specialization, the male doctor utilizes logos well, for the most part, with his use of questions and clear steps. He also integrates pathos excellently due to an appropriate placement of this strategy and the fact that he is not so knowledgeable about the cure of the patient's problem weakens his ethos.
For example, although majority of male doctors utilizes digital health well for the most part, only a little fraction of the female doctors often uses it. One of the female respondents agrees, "Yes, I do. They are essential as most of the times information regarding an adverse effect of the drugs which my patients may face during the use are not found in our books. And it helps me to make them aware if the resulting symptom is something to worry about or not". Another doctor reveals sometimes he uses online Medscape and some other resources online. Of course, some of them are very useful while workings in the remote healthcare settings as the information they contain are incomparable.
The majority of the respondents (doctors) found to be using this or that online resources for updating themselves to a have better communication and a good treatment. However, the more experiences they have, the less they tend to use digital health information. It means the younger generation is quite familiar and used to with the technology.
The use of the resources will create a continuous and integrated care cycle that helps drive the best patient care outcomes. While technology is a key component in the healthcare ecosystem, it should only play a supporting role. Patients need to be center stage. For patients, the Art of Medicine hinges on good communication. They have come to see and listen to their doctors. In return, they expect to be seen and heard by their doctors. Unlike the doctors, though the patients are comfortable with the growing role digital health is playing in their care experience, they are less accepting of the technology if it distracts or interferes with their conversation time with their doctors. Besides, they value certain elements of their visit more than others: Time for discussion; advice and recommendations; privacy; and engagement.
Doctors will have greater success conveying their concern and interest in their patients’ wellbeing if they are able to focus on these aspects. Nepali hospitals should look for ways to connect patients and their doctors in both old and new ways through personal focus, and innovations that deliver insights and answers quickly.
Patients expect their doctors to care for them with both their hearts and minds. Patients look to them to provide with their clinical knowledge in a compassionate way, and patients seek their counsel as doctors try to understand their conditions and treatment options during some of the happiest and scariest moments of patients’ lives. The doctor's sensitivity and logos concentrated to the patient will also influence the doctor-patient communicative interaction. Such personality variables and virtues invariably form a part of the doctor's communicative style, and so may play a significant role in structuring the communication between the doctor and the patient.
One of the respondents claims that doctors communicate well with patients, why everyone does talk about the manner of doctors? Does the patient have all right to misbehave with his or her doctor. First doctor-patient ratio should be minimized as the hospitals are overcrowded. There should be less workload and healthy working environment where patients can be open up more. Doctors must have the perception of security so that they will go to the deputed sites willingly. The relatives of the patients shouldn't get involved between doctor and patient and the patient should trust their doctors. According to some doctors unless the general public is educated, communication will never improve in Nepal.
Fifty percentages agree and 45.8 percentages of the doctors strongly agrees that they believe she/he understands the language the doctor uses. But none strongly disagrees and only 4.2 percentages disagree on that. Speaking more clearly and being empathetic with politeness and enough time to a patient is another aspect. The doctors should give them time (even in teaching hospital like would if they were patient in your clinics) where healthy interactions can take place. Legal strictness is required to monkeys (quacks) who think "we (doctors) are gods" when in reality patients are gods and they are just the attendants.
One doctor suggests understanding the profession first and then taking patients as the one who are in pain or suffering. Treat them as their own. Show compassion as politeness does not cost anything, no matter how hard it is. As far as possible, communicate in local languages they will feel comfortable. Treat the patient as you like to be treated when you are sick. Therefore, doctors should not give much pressure. This way, they are able to think freely for the betterment of the patient and will result in a healthy communication.
However, 95% of the respondents still do not see the scope of telemedicine well in Nepal. According to them it is useless because of the barriers listed below (i) No internet access everywhere and every time and with good service; (ii) no technical men power are available; (iii) the experts are not available during emergency; and (iv) where it is needed, the situation is far more pathetic, need to supply the medicine and setting of a basic lab facility throughout year. Not all parts of the country are as developed as we see from an eye of a person born and raised in the city. So they now think that it is a waste of time and money to think of telemedicine at least for next 10 years in a country like Nepal. It still will take plenty of time.
In this study of use of digital health materials, my findings propose that both access to and use of digital health resources are growing rapidly recently. Some respondents, however, do not use digital health repertoires because of the cost, accessibility of internet, and lack of trainings. The findings also suggest that there is a significant and growing digital divide with respect to digital health services across gender, type of hospital and the location of the hospital.
Conclusion
Despite of variations in their background, fifty percentage of the doctors interviewed used plenty of digital health resources. They are New England Journal of Medicine, Journal of American Medical Association, Wall Street Health Journal, CNN Medical Health, BBC Health, Epocrates, and Skyscape as these are plenty of articles, legal and ethical issues encountered by doctors. Though the future of telemedicine is increasingly bleak now, the implications of the results of the use of digital health pose quite promising future in Nepal and other parts of the world as well.
In terms of experience, more experienced doctors use digital health resources less whereas the recent graduates get largely benefitted. Similarly, the female doctors use that less frequently than their male counterparts. Moreover, trainings and foreign exposures have accelerated the use of digital health resources. Consequently, doctor-patient communication gets enhanced with the use of more digital health resources.
References
- Flanagin AJ, Metzger MJ (2008) Digital media and youth: Unparalleled opportunity and unprecedented responsibility. Digital Media, Youth and Credibility 5: 27.
- Hsu J, Huang J, Kinsman J, Fireman B, Miller R, et al. (2005) Use of e-Health services between 1999 and 2002: a growing digital divide. JAMIA 12: 164-171.
- Wilson EV, Lankton NK (2004) Modeling patients' acceptance of provider-delivered e-health. JAM A 11: 241-248.
- Lupton D (2013)The digitally engaged patient: Self-monitoring and self-care in the digital health era. Social Theory & Health 11: 256-270.
- Segal J (2005) Health and the rhetoric of medicine. SIU Press.
- Clark PA, Capuzzi K, Harrison J (2010) Telemedicine: medical, legal and ethical perspectives. Med Sci Monit 16: RA261-RA272.
- Diaz JA, Griffith RA, Ng JJ, Reinert SE, Friedmann PD, et al. (2002) Patients' use of the internet for medical information.J Gen Intern Med 17: 180-185.
- Baker L, Wagner TH, Singer S, Bundorf MK (2003) Use of the internet and e-mail for health care information: results from a national survey. JAMA 289: 2400-2406.
- Derkatch C, Segal JZ (2005) Realms of rhetoric in health and medicine. University of Toronto Medical Journal 82: 138-142.
- Impicciatore P, Pandolfini C, Casella N, Bonati M (1997) Reliability of health information for the public on the World Wide Web: systematic survey of advice on managing fever in children at home. BMJ 314: 1875.
- Berland GK, Elliott MN, Morales LS, Algazy JI, Kravitz RL, et al. (2001) Health information on the Internet: accessibility, quality, and readability in english and spanish. JAMA 285: 2612-2621.
- Landro L (2006) Hospitals combat errors at the "Hand-Off”. The Wall Street Journal28.
- Koch JW (1998) Political rhetoric and political persuasion: the changing structure of citizens preferences on health insurance during policy debate. Public Opinion Quarterly 209-229.
- Hesse BW, Nelson DE, Kreps GL, Croyle RT, Arora NK, et al. (2005) Trust and sources of health information: the impact of the Internet and its implications for health care providers: findings from the first health information national trends survey. Arch Intern Med 165: 2618-2624.
- Hickie IB, McGorry PD (2007) Increased access to evidence-based primary mental health care: will the implementation match the rhetoric? Medical Journal of Australia 187: 100.
- Frost J, Massagli M (2008) Social uses of personal health information within patients like me, an online patient community: what can happen when patients have access to one another’s data. J Med Internet Res 10: e15.
- Graham LE, Zimmerman M, Vassallo DJ, Patterson V, Swinfen P, et al. (2003) Telemedicine-the way ahead for medicine in the developing world. Trop Doct 33: 36-38.
- Hine J (1996) Pedestrian travel experiences: Assessing the impact of traffic on behaviour and perceptions of safety using an in-depth interview technique. Journal of Transport Geography 4: 179-199.
- Im EO, Chee W (2006) An online forum as a qualitative research method: practical issues.Nurs Res55: 267.
- Hohwü L, Lyshol H, Gissler M, Jonsson SH, Petzold M, et al. (2013) Web-based versus traditional paper questionnaires: a mixed-mode survey with a Nordic perspective. J Med Internet Res 15: e173.
- Kvale S (2008) Doing interviews. Sage Publications.
- HIT (2016) How digital health is opening up communication between doctors & patients.
- Weiner JP (2012) Doctor-patient communication in the e-health era. Isr J Health Policy Res 1: 1.
- Eysenbach G, Jadad AR (2001) Evidence-based patient choice and consumer health informatics in the internet age. JMIR Publications 3: e19.
- Segal JZ (2009) Internet health and the 21stcentury patient a rhetorical view. Written Communication26: 351-369.

