Keywords
Desomorphine; Krokodil; Substances
Introduction
The consumption of substances evolves along with society; the emergence of new drugs, consumption patterns and associated pathologies has a bidirectional relationship with this process, determining the course of the same and the clinical prevalence that entails. Many of the determinants of these phenomena are migratory flows, periods of political change or economic deprivation [1] without neglecting the phenotypic or biologically conditioned aspects [2]. The use of LSD is the United States in the 1970s, the abuse of synthetic drugs in Spain during the 1990s, the consumption of inhalants in South America [3] at the end of the last century, are examples of this; various substances appear and reappear, initially in certain spaces of consumption and inexorably in the context of clinical assistance.
Within these substances, and with a great clinical and social repercussion in the last decade, is the desomorphine, krokodile or krokodil as one of the drugs most consumed in certain countries of the north of Europe and the old URRS, with a rapid expansion by the United States and South America [4], due to its high addictive potential, low cost and availability. The increase in consumption of krokodil inexorably entails a high social problem and incidence of serious organic pathologies associated with its use.
Although the beginning of consumption is in Russia, Ukraine and Georgia at the end of the last century, clinical care in the consumption of krokodil is currently focused due to the potential for organic and addictive deterioration of its consumption. There are also determining factors within the high social and media alarm that accompanies the whole process of consumption of krokodil, one of these aspects is the easy access to the substance, beginning in the rudimentary synthesis of krokodil in the home; another condition is the diffusion of the serious clinical manifestations of consumers offered in the media and the internet, sometimes generating a certain social alarm [5].
Krokodil: Pharmacology
The molecule dihydrodesoximorphin: C17H21NO2, desomorphine or commercially Permonid, is an analog of opiate synthesized in the year 1932 in the United States by the chemist Lyndon Frederic Small. Desomorphine is a derivative of morphine, in which the 6-hydroxyl group has been removed and the double bond [7] has been reduced. The traditional synthesis of desomorphine is part of α-chlorocodide, which in turn is obtained by reacting thionyl chloride with codeine. By catalytic reduction, α-chlorocodide produces dihydrodeoxycodone, which leads to the formation of desomorphine by demethylation [6] (Figure 1). Due to its structural similarity to morphine, it is suggested that desomorphine is a potent mu agonist opioid with increased toxicity and an analgesic power 5-10 times greater than morphine. The effect of desomorphine occurs approximately around two minutes of consumption with an average duration of between 60 or 90 min [7].
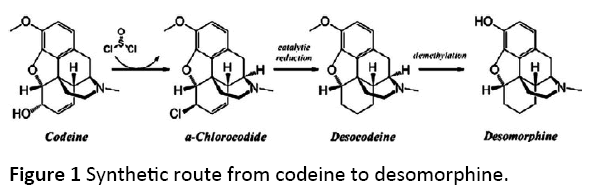
Figure 1: Synthetic route from codeine to desomorphine.
The main medical indications of desomorphine or Permonid marketed by Roche laboratories as a salt of hydrobromic acid varied from analgesic, antitussive and even sedative. Although due to the side effects: hypotension, retention urinary retention, vomiting and drowsiness, coupled with its rapid mechanism for addiction in humans conducive to its withdrawal from the market [8].
From the desomorphine to the krokodil
The krokodil neologism comes from the similarity in the pronunciation of chlorocodida, as well as from the lesions suffered by the consumers at the epithelial level; they recall the skin of a crocodile by the greenish tone and scaly appearance. The preparation of the substance is simple and economical, in most cases patients prepare krokodil in their own home, combining hydrochloric acid, iodine and red phosphorus with codeine, although there are different preparations where they are used to economize the process organic solvents or tropicamide. This process consists of two phases, the first in which codeine is combined either in tablets or syrup with gasoline and a second phase where the solution is mixed with iodine, hydrochloric acid and red phosphorus, after boiling this preparation for about 30minutes, resulting from this process and after distillation, krokodil, a byproduct with a high number of impurities and potential physical damage, which is often added ash or bicarbonate in view of raising the ph. This procedure is similar to the synthesis of methamphetamine from pseudoephedrine [9].This process varies according to countries and supply of substance, Russia, Ukraine and the rest of ex-Soviet republics share a long history of opiate and stimulant consumption dating back to the demise of the Soviet Union where homemade manufacture of heroin was common, methamphetamine, or methcatinone. This manufacturing of its own substances for consumption began in the late 1990s; heroin from Afghanistan was gradually imported and began to replace household variants in many Russian cities, particularly those adjacent to trafficking routes of heroin. The same development is observed in the Baltic States and in Central Asian countries, although imported heroin was never widely available in Ukraine and domestic practice remains in urban and rural areas. Elsewhere, the production of home injectable continues along emerging heroin markets [10].
In the last five years, a growing number of reports on the prevalence of substance use have shown that the consumption of inhaled opium and parenteral heroin has been significantly reduced in Russia, Ukraine, Kazakhstan and Georgia, while a notable increase In the consumption of drugs containing codeine (Solpadeine, Codterpin or Codelac) to produce desomorphine [11].
One of the questions about this manufacturing process is whether or not desomorphine can actually be produced through the rudimentary procedures followed by consumers [12], where the risk environment of production and use of krokodil is shaped by physical, social, economic and political factors. At first the production of krokodil is linked to regions of the former USSR. This homemade synthesis takes place at a time when the enormous police pressure of a totalitarian communist regime against drug use, the criminalization of consumption and trafficking, combined with the enormous blockade on the import of any type of drug, has limited availability of opiates and stimulants of the illegal market. All these factors together with the situation of constant economic crisis and the relative availability of legal precursors in pharmacies, supports until today a culture of the homemade manufacture of substances, as alcohol, krokodil or Pervitin (methamphetamine) in Prague since beginning of 1980 [12].
This model of consumption and self-sufficiency is different from that observed in other countries where drug trafficking dominates the production and distribution of drugs [13]. Although drug trafficking and availability are nowadays a reality in which it seems that the economic conditions are the ones that support this practice of substance use [14], in the case of Krokodil, cases of home-made manufacture of desomorphine are beginning to be detected in areas with high unemployment rates and economic problems [15].
Krokodil: Consumption and consequence
The main routes of consumption of krokodil are oral and parenteral, although oral use is practically symbolic, the parenteral route leads to serious consequences at organic level widely known and almost always linked to heroin consumption: HIV, HCV, endocarditis, etc. The damages associated with the injected consumption of krokodil are considered more serious and unprecedented within the physical consequences of drug use. In addition to the high prevalence of previous prototypical problems of parenteral consumption, in the case of krokodil there is a lack of specific programs of action at tertiary level, harm reduction, etc. In the countries with the highest consumption, the health and socio-health care system is sometimes non-existent [16]. The main object of clinical attention and the major complication of krokodil consumption appear to be the consequences in the blood tissue: abscesses, phlebitis, thrombophlebitis, hemorrhages, ulcers, etc., occurring near injection sites, as well as damage in muscles, soft tissues and bones with rapid necropsy and gangrenation. The intervention in these problems requires in most cases surgery of extreme complexity, with serious results, like the surgical removal of the main veins in the arms or the legs, sometimes needing amputation or skin grafts. The harmful effects of krokodil are not limited to only injection-related organic injuries due to the toxic components of the substance such as iodine thyroid and muscle injuries occur or severe deterioration in cartilage by phosphorus. These toxic compounds in turn lead to neurological and endocrine damage in the organs involved in the metabolism of the chemicals and heavy metals used in the synthesis of the substance. The initial manifestation of these effects occurs within a few days of the initiation of krokodil venoinjection and includes organic symptoms where the most common are: pneumonia, meningitis, periodontitis, osteomyelitis, etc. All this organic process and symptomatology constitutes a progressive physical deterioration of the consumers at the same time as very high mortality rates, although not all the users experience the extreme damages associated with krokodil.
The psychological consequences of consumption are not often so well documented, along with the obvious and progressive process of substance dependence there is a significant neurological damage, speech disorders, loss of motor skills, memory, mood and severe psychotic episodes, most often produced by intoxication due to the chemicals that krokodil brings [17]. No cases or studies have been described to date that address the relationship of consumption of krokodil with dual pathology; in 2013 the first clinical cases within the European Healthcare Network begin to be reported, all of them centered on the clinic of organic typology. Although it seems that, as in opiate consumption, the higher incidence of associated mental disorders is manifested in anorexic and anxiety symptoms [18] and linked to patterns of characteristic dysfunctionality, such as borderline or antisocial personality disorder [19,20].
Treatment
The treatment of any addictive pathology leads to a joint pharmacological intervention to a psychotherapeutic process, the intervention in patients consuming krokodil is complex due to the manifest organic deterioration, marked addictive potential of the substance and high availability. Within the clinical evaluation process, the clinical diagnosis in relation to addictive pathology seems to be much more evident, although an adequate psychopathological evaluation is necessary, where clinical concepts and methodological instruments of evaluation in mental health are used.
A conditioning factor in krokodil´s consumption care is to avoid the delay in access to adequate treatment, as consumption can exacerbate the serious organic damage described above. For many consumers the use of krokodil can end with mutilations, amputations and even death. While most users ask for specialized care when a permanent disability or death seems to be the most likely outcome. On the other hand, it should be kept in mind that the life expectancy of an active heroin addict is up to six or seven years whereas that of a krokodil addict is much shorter, with a maximum of two years, even many patients die after their first dose of this drug, which determines a high need in clinical intervention [21].
Conclusion
The need of clinicians to know, anticipate and intervene in the psychopathological reality so that the prevalence of certain mental disorders does not evolve is one of the objectives that since health care are determined as a guideline of intervention of the first order. However, in the area of substance use disorders, it is shown as an objective sometimes configured not only by the patient's clinical evolution, but also by external factors: health policies, legislation on the regulation of consumption, availability of substances, etc. .These factors sometimes determine the course of the mental illness, the consumption of substances and therefore the achievement of the established purposes. The supposed expansion and perhaps excessive social alarm of the consumption of krokodil, since the consumption rates in the old USSR oscillate around 5% of the consumers of opiates and in other countries their consumption is subject of clinical cases, without a determined prevalence [22], is a clear example of this process and one of the new challenges in clinical care in substance use disorders.
References
- Alexander B (2008) The globalization of addiction: A study in poverty of the spirit. Oxford University Press, New York.
- Hiroi N, Agatsuma S (2005) Genetic susceptibility to substance dependence. Mol Psychiatry 10: 336-344.
- Fernández P, Hernández I (2003) Características farmacológicas de las drogas recreativas (MDMA y otras anfetaminas, Ketamina, GHB, LSD y otros alucinógenos). Adicciones 15: 51-75.
- Heimer R (2013) Patterns of new drug emergence: A comment in light of ‘krokodil”. Int J Drug Policy 24: 275-280.
- Gahr M, Freudenmann RW, Hiemke C, Gunst IM, Connemann BJ, et al. (2012) Desomorphine goes crocodile. J Addict Dis 31: 407-412.
- Eddy NB, Halbach H, Braenden OJ (1957) Synthetic substances with morphine-like effect. Bull World Health Org, pp: 569-863.
- Eddy NB, Howes H (1935). Studies of morphine, codeine and their derivatives X: Desoxymorphine-C, Desoxycodeine-C and their hydrogenated derivatives. J Pharmacol Exp Ther 55: 257-267.
- Maituk D (2014). Krokodil: A monstrous drug with deadly consequences. JAD, pp: 1-14.
- Abdala N, Grund JPC, Tolstov Y, Heimer R (2006) Can homemade injectable opiates contribute to the HIV epidemic among injection drug users in the countries of the former Soviet Union? Addiction 101: 731-738.
- Platt L, Rhodes T, Hickman M, Mikhailova L, Lisetsky K, Sarang A, et al. (2008) Changes in HIV prevalence and risk among new injecting drug users in a Russian city of high HIV prevalence. J Acquir Immune Defic Syndr 47: 623-631.
- Savchuk SA, Barsegyan SS, Barsegyan IB, Kolesov GM (2008) Chromatographic study of expert and biological samples containing desomorphine. J Anal Chem 63: 361-370.
- Zabransky T, Grund J-PC, Latypov A, Otiashvili D, Stuikyte R, et al. (2012) Harm reduction in Central and Eastern Europe.Harm reduction in substance use and high-risk behaviour: International policy and practice summaries. Oxford: Wiley-Blackwell, pp: 301-321.
- Rhodes T (2009) Risk environments and drug harms: A social science for harm reduction approach. Int J Drug Policy 20: 193-201.
- Grund JPC (2002) A candle lit from both sides: The epidemic of HIV infection in Central and Eastern Europe. McElrath K, editors. HIV and AIDS: A global view. Westport, CT: Greenwood Press, pp: 41-68.
- Kwint HM, Kruizinga SP, Kaal M-JH, Bootsma H-PR (2013) Gevaarlijke designer drug 'krokodil' voor het eerst in Nederland. Pharm Weekly 7: 128-130.
- Grund JPC, Latypov A, Harris M (2013) Breaking worse: the emergence of krokodil and excessive injuries among people who inject drugs in Eurasia. Int J Drug Policy 24: 265-274.
- Harris M (2013) The ‘do-it-yourself’ New Zealand injecting scene: Implications for harm reduction. Int J Drug Policy 24: 282-284.
- Havard A, Teeson M, Darke S, Ross J (2006) Depression among heroin users: 12 month outcomes from the Australian Treatment Outcome Study (ATOS). J Subst Abuse Treat 30: 355-362.
- Darke S, Ross J, Williamson A, Mills KL, Havard A et al. (2007) Borderline personality disorder and persistently elevated levels of risk in 36 month outcomes for the treatment of heroin dependence. Addiction 102: 1140-1146.
- Walter m, Degen B, Treugut C, Albrich J, Oppel M, et al. (2011) Affective reactivity in heroin-dependent patients with antisocial personality disorder. Psychiatry Rev 187: 210-213.
- Grund JP, Merkinaite S (2009) Young people and injecting drug use in selected countries of Central and Eastern Europe. Vilnius: Eurasian Harm Reduction Network.
- Mathers BM, Degenhardt L, Phillips B, Wiessing L, Hickman M, et al. (2008) Global epidemiology of injecting drug use and HIV among people who inject drugs: A systematic review. Lancet 37: 1733-1745.

