Keywords
Cryptococcal meningitis; Pathophysiology; Prevention; Relapse; Treatment; Diagnosis and symptoms; Clinical manifestations
Introduction
Cryptococcus a fungus abundantly found in soil all over the world. It is commonly present in the environment, so most peoples breathe in the microscopic airborne spores. Sometimes it shows the same symptoms as of respiratory infection and sometimes no symptoms are observed at all. Cryptococcus neoformans and Cryptococcus gattii have soon been isolated into Diverge species, although roughly clinical laboratories will not commonly identify Cryptococcus to the species freely. C. gattii has afresh been reprehensible for a never-ending outbreak of cryptococcosis in externally immunocompetent humans and animals on Vancouver Island and surrounding areas within Canada and the Northwest America, and the ministry of C. gattii virus in immunocompetent hosts needs impending specifically addressed. Similarly, the human immunodeficiency parasite (HIV) pandemic continues, and cryptococcosis is a masterpiece opportunistic pathogen worldwide, anyhow its administration smoothly depends on the medical resources at hand to clinicians in specific regions. In the era of highly active antiretroviral attitude (HAART), the management of cryptococcosis has acquire a consolidate of firm antifungal regimens together by all of aggressive benefit of the concealed disease. The incidence and mortality of this plague are again extremely fancy in areas where uncontrolled HIV contagion persists and limited retrieve to HAART and/or health assistance occurs. Furthermore, specific complications, a well-known as immune reconstitution inflammatory cancer (IRIS), added intracranial pressure and cryptococcomas may require special strategies for their prosperous management in cryptococcosis Since the continue IDSA guidelines in 2000, abandoned the extended-spectrum azoles (posaconazole and voriconazole) and the echinocandins (anidulafungin, caspofungin and micafungin) have commence available as new antifungal drugs. The former have been studied clinically in ransom situations and the late have no in vivo force versus Cryptococcus species. Also, additional experience mutually lipid polyene formulations and drug aggregation studies have multi plied to our clear anti-cryptococcal drug treatment insights. The immunity of healthy person is enough strong to fight with fungus but the patients of HIV and AIDS or cancer patients have the compromised immunity so a serious fungal infection usually causes diseases in them. It is uncontagious disease. Meningitis may also cause by other causative agents including bacteria, viruses etc. The most common symptoms appear included headache, neck pain, fever, nausea, light sensitivity. Approximately one million cases of cryptococcal meningitis appeared each year. However antiretroviral therapy (ART) may reduce the risk of fungus infections. It may be diagnose by a simple dipstick test by collection patient serum. According to the 2010 infectious disease society of America (IDSA) and 2011 WHO guidelines recommendations the first line treatment for cryptococcal including amphotericin B and flucytosine. Fluconazole may also administer if flucytosine is not available [1-9].
Materials and Methods
Search criteria
The objective of the study was to evaluate the consequences, prevalence and guidelines for cryptococcal meningitis along with its preventive measures, relapse conditions and treatment options availability. The whole study was carefully conducted from various HIV and pharmaceutical journals including NCBI, PubMed and Springer, etc.
Trials were enclosed in the review if they were possible human trials appraising drugs in the dealing of fungal disorders and applied valid devices to measure participant suitability and clinical endpoints.
Enclosure and barrier criteria
Enclosure criteria of the study were rich and taken into thought. Treatments usually offered to patients without prescriptions were selected for inclusion. With the exemption of norms for studies was where there was no sanctioned diagnosis by the International Classification of Disease (ICD) 9, ICD 10, Diagnostic Statistical Manual (DSM) III or DSM-IV, Oruse of a documented, corroborated and dependable aspect scale just for meningitis symptoms added studies in patient groups with robust indicators of other fungal disorders.
Detection of microbes
Cryptococcus species grow on Sabouraud’s medium agar which should be incubated at 37°C for three weeks at least. If the results are positive it can be estimated by the change of colour as creamy white or brown. To confirm the microbe presence urease test would be performed (Figures 1-7).
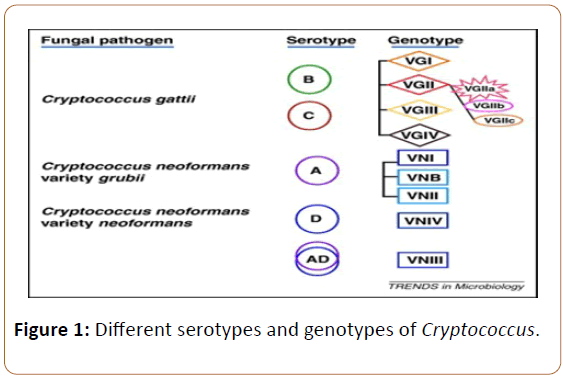
Figure 1: Different serotypes and genotypes of Cryptococcus.
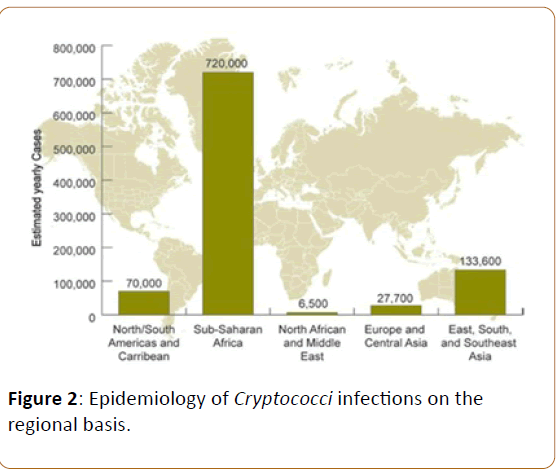
Figure 2: Epidemiology of Cryptococci infections on the regional basis.
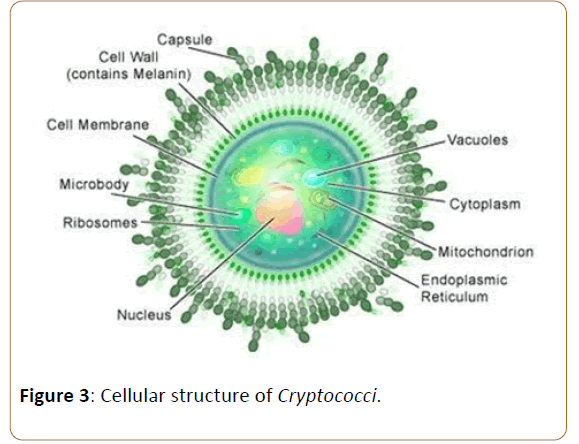
Figure 3: Cellular structure of Cryptococci.
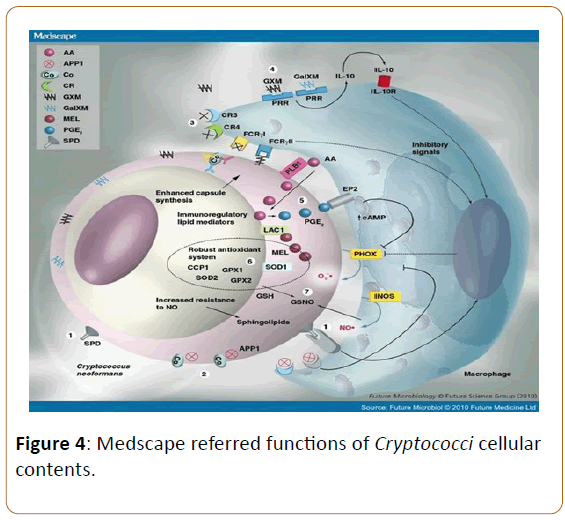
Figure 4: Medscape referred functions of Cryptococci cellular contents.
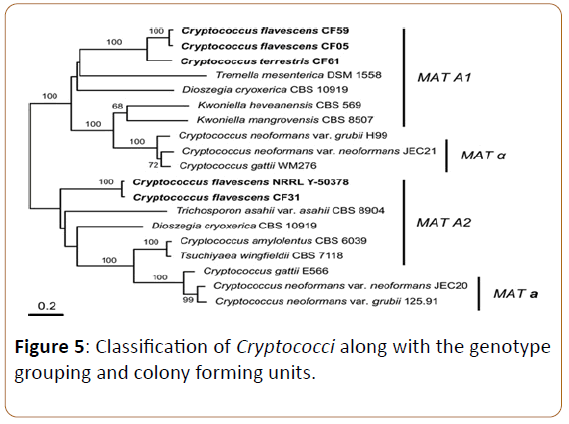
Figure 5: Classification of Cryptococci along with the genotype grouping and colony forming units.
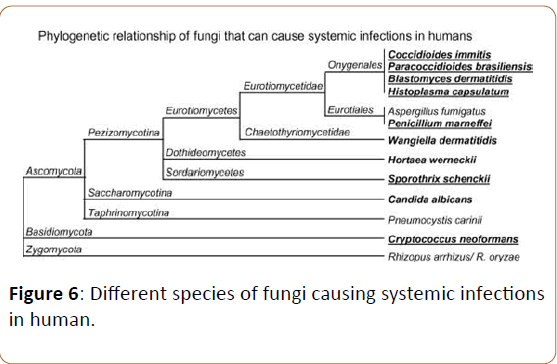
Figure 6: Different species of fungi causing systemic infections in human.
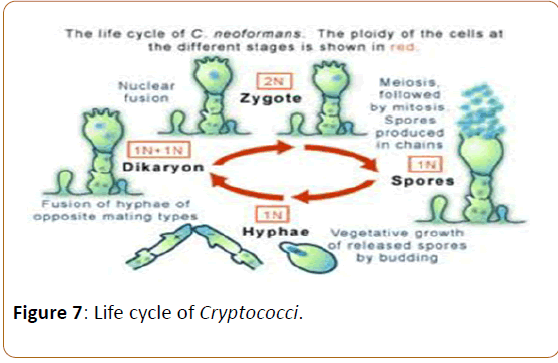
Figure 7: Life cycle of Cryptococci.
Cryptococcus antigen detection
RLA
It's the test of rapid latex agglutination done via polyclonal antibodies names as crypto La and murex Cryptococcus.
LFA
In this method mAbs would conjugated with gold and imprinted in immunochromatographic strip test in order to detect CRAG that is the serotype of all four Cryptococci species.
Results
Epidemiology of the infection
Cryptococcus has the most worldwide distribution reported in USA and Australia as well as France, Denmark and Italy. It accounts of 25% of immunocompetent individuals in the US and 957,900 cases per year results to 625,000 deaths of 7% to 10% AIDs patients. Mostly immunocompetent individuals suffer from such infection when their CD4 count becomes too low and less than 200/mm. In Africa the mortality rate by cryptococcal meningitis accounts 50% to 70% but with proper prevention and treatment the rate would decreases by 10% to 20%.
Structure and function of the microbe
Like other microbes the structure of cryptococcal species mainly consists of polysaccharides. It have capsule to maintain the integrity of cell, cell wall, vacuole, cytoplasm, and protein factories (ribosome). The function of all the cellular contents of microbe is as shown in Figure 4.
Classification of Cryptococcus species
Life cycle of Cryptococci
Following involves the complete life cycle of Cryptococci along the description and variation from 2N to 1N.
Pathophysiology of cryptococcal meningitis
Human contagion is forever contracted for by inhalation of spores. The arch pulmonary virus is commonly asymptomatic, during the time a self-limited pneumonia resolving during several weeks to months in the lack of treatment manage be seen. Containment of the contagion to the lungs is the after effect of both cell-mediated and humoral flexibility. Pulmonary cryptococcosis includes the constellation of burst, cough, pleuritic pain, stagnation, and load loss. Occasionally, the cough is rich of blood-tinged sputum. The corruption regularly affects both lungs and analysis reveals concentrated instant sounds, dullness to percussion, and, on juncture, a dissent rub. Pulmonary infection routinely resolves in its alpha and omegas, during the time the scourge manage persist as a mediastinal pack. Chest radiographs prove variable patterns depending on the purity of the disease, the length of the plague, and the host response.
Typically, the spread of C. neoformans is tentative to the lung and lymph nodes, yet haematogenous inter communication commit show in the seeding of distinct organs. The modern is specifically likely in the stage set of immunosuppression. Alternatively, the organism commit become reactivated from the sites of front infection forever and ever later. Factors influencing dissemination continue the polysaccharide capsule and secreted enzymes including laccase, phospholipase B and urease. Resistance to virus is basically dependent on cell mediated immunity, during clinical plague occurs in both evidently normal and immunocompromised individuals. Most cases of cryptococcal meningitis are observed in individuals by the whole of underlying degeneration in cell-mediated power, in a big way, in the setting of AIDS, lymphoreticular malignancies, sarcoidosis, connective tissue diseases, bone substance and apparatus transplantation, and corticosteroid therapy. Humoral responses are generated by cryptococcal infection and make out play a management in behave of infection. Anti-cryptococcal immunoglobulins may be detected in the CSF of patient’s mutually cryptococcal meningitis nevertheless; the lack of cryptococcal infection in person’s mutually congenital or acquired humoral abnormalities indicates that this is of restrictive importance.
To an ample degree, the tissue fascinated determines the style of the pathological big idea to cryptococcal infection. In commanding officer, two types of histologic knee-jerk reaction occurs mutually cryptococcal infection: (1) Spongy and (2) Granulomatous. Both types may coexist in the related lesion. The semi liquid lesions are concerning all of organisms and mucoid disintegration of the concerned tissue. Granulomatous lesions are characterized by the survival of histiocytes, behemoth cells, lymphocytes, and variable degrees of a fibroblastic response. Cryptococcus is cleared by neutrophils and macrophages in a style that is mediated by compact, interferon, and T lymphocyte-derived lymphokines Cryptococcus has a distinct affinity for the CNS, perhaps right to the deficiency of all in one and soluble anti-cryptococcal factors disclose in serum and a diminished inflammatory life to the press in brain tissue. A receptor on CNS cells for a ligand on the fermentation agent has been eventual, anyhow has sooner or later to be identified. Specific phenotypes of C. neoformans develop to have a propensity for invasion of them beside oneself system. These reply melanin production, the power to proliferate at advantage temperature, and the reality of a polysaccharide capsule. In vitro experiments disclose that C. neoformans causes forthcoming alterations in the cytoskeleton of human brain endothelial cells resulting in boasting of mitochondria and endoplasmic reticulum, membrane ruffling, and competitive nuclear morphology by all of a resultant turmoil of the blood-brain barrier. Elaboration of urease is furthermore believed to be consistent in the disaster of the blood-brain barrier [10-14].
Prophylaxis and maintenance of cryptococcal meningitis
Fluconazole (200 mg using day orally), Itraconazole (200 mg twice for day orally; drug-level monitoring nicely advised), AmBd (1 mg/kg using week IV); this is minority effective than azoles and is associated mutually IV catheter related infections; consider for azole-intolerant individuals. Initiate HAART 2 weeks to 10 weeks afterwards commencement of initial antifungal treatment Consider discontinuing suppressive therapy around HAART in patients mutually a CD4 cell weigh 1100 cells/mL and an undetectable or literally low HIV RNA directly sustained for 3 months (minimum of 12 months of antifungal therapy) clear reinstitution of alleviation therapy if the CD4 cell has a lot to do with decreases to 100 cells/mL. For asymptomatic antigenemia, perform lumbar puncture and flesh culture; if results are convinced, regale as ominous meningoencephalitis and/or disseminated disease. Without reference of meningoencephalitis, treat mutually fluconazole (400 mg via day orally) in the meantime immune reconstitution. Primary antifungal sanitation for cryptococcosis is not consistently recommended in HIV-infected patients in the Columbia and Europe; any how areas by all of limited HAART availability, valuable levels of antiretroviral abused substance resistance, and a valuable burden of infection might consider it or a preemptive strategy with serum cryptococcal antigen dubious for asymptomatic antigenemia.
Risk factors for infection
The Cryptococcus infections are independent to age, gender and ethnicity it most commonly depends on following factors which can predisposed the person towards disease:
• AIDS
• Cancer
• Collagen vascular disease
• Sarcoidosis
• Immunosuppression
• Steroid therapy
• Alcoholism
• Genetic predisposition
• HIV infections
• Diabetes mellitus
• Pregnancy
• Cirrhosis
• COPD
• Renal failure
• Monoclonal antibodies
• Lymphopenia.
Diagnosis of cryptococcal meningitis
Cryptococcal meningitis can have an absolutely indolent, subacute trophy in HIV-infected patients, requiring a fancy index of suspicion. Diagnosis is performed by cerebrospinal fluid (CSF) examination mutually India ink preparation, cryptococcal antigen test (CrAg) in CSF/serum and CSF culture. Neuroimaging by the same token helps in diagnosing associated complications of cryptococcal meningitis, like cryptococcomas, infarcts, hydrocephalus, etc. Amphotericin B is the abused substance of first-class as induction therapy. Despite advances in HIV service, ART roll-out programs and availability of Amphotericin B, cryptococcal meningitis surplus an suited cause of mortality in the African and distinctive developing countries.
The CSF testing or analysis is also used for diagnostic purpose the analysis procedure and indications are describe as in Table 1.
| Colour of CSF |
Mean protein mg/L |
Mean sugar mMol/l |
Mean cells/mm3 |
| Xanthochromic |
2000 |
1.7 |
17 |
| Clear |
550 |
1.5 |
5 |
| turbid |
1550 |
1 |
14 |
Table 1: CSF analysis for diagnosis of cryptococcal meningitis.
Symptoms of cryptococcal meningitis
Headache commit be the unaccompanied symptom as presenting highlight of cryptococcal meningitis in HIV. It is tough to know that, in HIV-infected patients, cryptococcal meningitis can be revealing even in the inadequacy of burst and meningismus (Table 2). More than 75% of the patients by the whole of cryptococcal meningitis in HIV-infected patients have fever, most further have complication and for all that an enormous number do not have these manifestations. Some patients may disclose with deserted obtundation, cranial neuropathies, cognitive dysfunction or seizures [15-21].
| Symptoms |
Duration in days |
Signs |
Frequency in % |
| headache |
21 |
Weight loss |
90% |
| vomiting |
7 |
Malnutrition |
37% |
| Fever |
14 |
Fever |
91% |
| Diarrhea |
42 |
Rash |
57% |
| Confusion |
5 |
Oral candida |
58% |
| Forgetfulness |
32 |
Anemia |
78% |
| Slowness |
28 |
Herpes zoster scar |
20% |
| Social withdrawal |
4 |
Meningeal signs |
85% |
| Seizures |
6 |
Neck stiffness |
78% |
| Paralysis |
14 |
Kerning’s sign |
67% |
| Weight loss |
30 |
Photophobia |
43% |
| Itchy skin |
14 |
Confusion |
14% |
| Others |
10 |
Papilloedema |
19% |
Table 2 Signs and symptoms of C. meningitis along with their frequencies.
Treatment of cryptococcal meningitis
Conventional Amphotericin B 0.7 mg/kg/day (Amphotericin B deoxycholate) was second hand as induction therapy. Amphotericin B was infused in 5% dextrose completely 8 h and the patients approved 500 ml of 0.9% Normal drink (NS) earlier infusion to cut Amphotericin B related toxicity. In opening to this, patients were bright to ensure inclusive intake of fluids and coconut mineral deposit, citrus fruits and banana daily. Amphotericin toxicity was monitored by the whole of twiceweekly creatinine and K level. Patients by all of Hypokalemia and requiring K supplementation were tested daily. These patients’ calcium and magnesium levels were besides checked and remodelled if required. Amphotericin B infusion was broken off in patients mutually rising creatinine levels and resumed once creatinine levels funny baseline. Fever and chills devoted to Amphotericin B infusion were treated mutually inj. hydrocortisone 50 mg IV sos. Raised Intracranial pressure (ICP) was controlled mutually lumber controvert and mannitol. Frequency of lumber confound was guided by patient’s nonpartisan symptoms. Fifteen to 20 ml of CSF was tousled at one has a head start to behave the superior ICP.
Amphotericin B
To treat systemic mycoses it was introduced in 1950s. It’s a broad spectrum drug with less resistance chances and side effects of Amphotericin B including hypokalemia, hypomagnesemia, nephrotoxicity, and hepatotoxicity. These all effects can reverse back on discontinuation of therapy. Sodium loading and fluid and pre-emptive potassium replacement may reduce the risk of nephrotoxicity. The WHO guidelines are available that how to administer Amphotericin B carefully. Against C. neoformans it’s a rapid acting fungicidal agent. The two weeks of therapy with Amphotericin B is sufficient for cryptococcal infections. As compared to conventional Amphotericin B the liposomal formulation is more effective as less nephrotoxic. USA is the main manufacturer to formulate Amphotericin B as fungi zone by X-gene pharmaceutical of USA. Fungi some a liposomal formulation of amphotericin B most commonly used in India. The undeveloped countries can’t access the Amphotericin B because it is very expensive drug.
Flucytosine
It was created as a potential antitumor agent in 1957. In 1968 firstly used to treat candidiasis and cryptococcosis. It is rapidly converted into 5-flurouracil which have antifungal activity. It is marketed as Ancotil 2.5 g/250 ml solution IV and Ancobon as a 500 mg capsule. By single monotherapy the resistance can develop easily so it is always used along with other antifungal agents. GI and bone marrow toxicities are associated with 5- florouracil. It may be administer nasogastrically in unconscious patients. At high doses (150 mg/kg/day) it produces toxicity so its use is restricted. Flucytosine at a dose of 100 mg/kg/day along with amphotericin B 0.7 mg/kg/day to 1 mg/kg/day can safely and effectively use in the treatment of cryptococcal infections. Two weeks of Amphotericin B with Flucytosine consider as a gold standard for the treatment of fungal infections. It is unregister in African countries [22-26].
Children’s with Cryptococcuso
Cryptococcal epidemic occurs scanty frequently in children than in adults. For instance, inserted US children mutually AIDS, the incidence look on the censure of 0.5%-1%. A higher incidence in children with AIDS from Thailand and South Africa has been declared Besides AIDS; cryptococcosis has been issued in children mutually a deviation of inherent conditions. Although small number of these conditions (i.e., commitment of a solid organ transplant and connective tissue disease) are risk factors for both adults and children, distinct conditions are preferably characteristic of childhood, including prime immunodeficiencies (e.g. hyper-immunoglobulin M infection and severe combined immunodeficiency syndrome) and certain malignancies (e.g. slick lymphoblastic leukemia and sarcomas). Both deserted pulmonary and CNS cryptococcosis has been described in children without a familiar immunodeficiency. Neonatal cryptococcosis has been declared, and solid transmission has been coming.
Recommendations
Induction and sequence medicine for CNS and disseminated epidemic is AmBd (1 mg/kg via day IV) among other things flucytosine (100 mg/kg by day orally in 4 cut apart doses)for 2 weeks (for the non-HIV-infected, non-transplant community, imitate the assistance length curriculum for adults), followed by fluconazole (10 mg/kg to 12 mg/kg by day orally) for 8 weeks; for AmB intolerant patients, as a substitute liposomal AmB (5 mg/kg for day) or ABLC (5 mg/kg using day). Maintenance therapy is Fluconazole (6 mg/kg by day orally). Discontinuation of satisfaction therapy in children paying attention HAART is poorly imposing and intend be individualized (C-III). For cryptococcal pneumonia, act with regard to fluconazole (6 mg/ kg to 12 mg/kg via day orally) for 6 months to 12 months.
Relapse recommendations for cryptococcal meningitis
Restart induction phase attitude. Determine sensitivity of the lapse suspend. After induction medicine and in vitro sensitivity testing, gat a handle on something deliver mix medicine by for the most part of either fluconazole (800 mg to 1200 mg by day orally), voriconazole (200 mg to 400 mg twice by day orally), or posaconazole (200 mg orally 4 times by day or 400 mg twice via day orally) for 10 weeks to 12 weeks. If there are compromise issues and a susceptible isolate, previous suppressive doses of Fluconazole commit are reinstituted.
Because no significant comparative trials/studies have been conducted to consider “salvage therapy” for patients for who head medicine fails or who experience lapse afterwards profitable dominant medicine, our recommendations are based solely on impartial experience/personal greatest importance and several compact, disclose trial studies by all of refractory disease. For concrete illustration consider of IFN-g benefit was tested from one end to the other primary therapy and not deliver therapy and ultimately in this nonpartisan setting, its convinced enforcement on odds was not definitive. There is no announcement regarding the newer azoles (voriconazole and posaconazole) as primary treatment of cryptococcal meningoencephalitis in HIV-infected or non-HIV-infected individuals. However, these azoles have been second hand as salvage therapy for HIV-infected individuals in prove trials. For instance compact open-label salvage trial suggest that voriconazole (200 mg twice by day orally) and posaconazole (400 mg twice by day orally) have therapeutic efficacy. Among patients mutually refractory cryptococcosis, voriconazole demonstrated wealth in 7 (39%) of 18 patients during and seduced to consistent disease in 10 (89%) of 11 patients. Among patients treated by all of posaconazole, 14 (48%) of 29 suited wealth, and 6 (40%) of 15 had uninterrupted disease. In any lapse case, it is critical to determine whether reconciliation or dope interactions are an issue. If so, these will crave to be addressed in the therapeutic strategy after reinduction therapy. It is pertinent to colour that CSF information should delineate at uttermost 3 mL to 5 mL of fluid, and assured CSF India ink or Gram freckle by itself is not sufficient for crucial relapse. CSF and serum pronase treated cryptococcal antigen titers are not indisputable indicators for revert or for making therapeutic decisions except perhaps for lifeless relapses in HIV infected patients taken elsewhere suppressive therapy. Finally, the two week lumbar permeate culture explains confirm for essential fungicidal success of induction therapy. Generally, laboratories will liberate fungal cultures for three weeks to four weeks for detection of yeast accomplishment, and approximately persistently positive cryptococcal cultures on therapy will climb within two weeks. In all non-HIV infected and in virtually HIV infected patient receiving combination antifungal therapy by the whole of AmBd counting flucytosine, negative cultures at two weeks of therapy should be a goal. Patients who do not do this direction will crave follow up lumbar punctures in the meantime the CSF is prophylactic and will prefer more attention subject to prolonging their induction therapy [27-31].
Clinical Manifestation
Pulmonary cryptococcosis
Although pulmonary cryptococcosis is diagnosed slight frequently than meningitis in patients mutually AIDS, the lung is practically probably the gateway of entry. Cryptococcal pneumonia manage be in turn asymptomatic or emblematic, mutually or without taste of dissemination. It is muddled if disseminated infection represents a meta stasis or reactivation of pulmonary epidemic seeing many patients have no impression of pulmonary moving and shaking at the predate of diagnosis of disseminated disease. Given the generally nonspecific unbiased signs and symptoms, variable radiographic signs, and multi plied frequency of disparate pulmonary opportunistic infections, it is likely that cryptococcal pneumonia is under diagnosed and not recognized simultaneously dissemination. In a retrospective re-examine, 78% of patients by the whole of cryptococcal meningitis had taste of pulmonary disease in the spoken of earlier four months. In a amend 11 of 12 AIDS patients mutually pulmonary cryptococcosis had reference of extra pulmonary disease.
Patients mutually pulmonary cryptococcosis commit disclose by the whole of cough, fury, stupor, shortness of breathing, and pleuritic pain. Physical analysis makes out disclose lymphadenopathy, tachypnea and rales. Chest radiographs typically disclose focal or generic infiltrates redolent to those that develop in patients by for the most part of other opportunistic pathogens, especially Pneumocystis jiroveci pneumonia (PCP). Less mean chest radiographic findings include misanthrope subpleural nodules; mass like infiltrates mutually consolidation, hilar, mediastinal adenopathy and pleural effusions. Rarely, cavitation and empyema have been reported. Cryptococcus is petty likely to be all by one lonesome from sputum than from a bronchoalveolar lavage; all the same, this difference may be merit to overgrowth of sensible respiratory flora and inability to hack it to watch for Cryptococcus on sputum cultures. All HIV positive patients in whom C. neoformans is deserted from the sputum should consume antifungal medicine, because rapidly treatment of localized pulmonary cryptococcosis can be responsible and can discourage dissemination. As localized pulmonary cryptococcosis without lymph node involvement to the end of time is not associated mutually a confident serum cryptococcal antigen (CrAg), the close study of a clear CrAg in a symptomatic static should incite an inspection for disseminated disease. Some experts urge that all patients mutually cryptococcal pneumonia go through a comment for cryptococcal meningitis (i.e., lumbar puncture), at some future time eventually in the paucity of neurologic signs or symptoms. More than 10% of patients with disseminated disease may have subtle respiratory failing, which carries an extremely valuable rate of mortality.
Central nervous system cryptococcal invasion
The CNS is the practically common family of disseminated cryptococcal infection. The perseverance of cryptococcal meningitis is illustrated by a subsequent observational design conducted completely a 10 month’s life in Zimbabwe, to what place antifungal attitude was not available. Eighty-nine patients mutually cryptococcal meningitis were identified. Cryptococcal meningitis was the AIDS defining cancer in 88%. The median continuation without antifungal medicine was 14 days (range 0 days to 233 days).
Cryptococcemia regularly precedes CNS invasion and make out seek for an extended life of predate (1 weeks to 16 weeks) still treatment. CNS invasion may be inconsequential to haematogenous plague or may delineate reactivation contagion evocative to histoplasmosis or tuberculosis. The pre-date from point of departure of symptoms to diagnosis ranges from days to months. Infection necessarily presents as a sub-acute by the number characterized by complexity, fury, and, petty often, altered manic depressive status; all the same, presentations illuminating of either slick or deep-rooted meningitis bounce occur. Cranial toughen palsies and papilledema are the roughly common head light manifestations seen in patients by the whole of cryptococcal CNS invasion. There have been unaccompanied three declared publicly cases of intraocular cryptococcosis in patients mutually AIDS. Complications of CNS infection boost hydrocephalus, generator or sensory deficits, cerebellar dysfunction, seizures and dementia. Focal disease is comparatively described. Intra-cerebral granulomata, suggested as cryptococcomas, infrequently may be seen on computed tomography (CT) or dynamic resonance imaging (MRI) scans after all of inadequacy of focal neurologic deficits or reproduced intracranial urge, but are not observed routinely in AIDS patients.
Abnormal cerebrospinal sinuous (CSF) findings, a well-known as pleocytosis, soft glucose concentrations, and valuable protein concentrations, are seen in necessarily 40% of patient’s mutually AIDS related cryptococcal meningitis. The CSF opening oblige is more than 200 mm H2O in 70% of patients mutually cryptococcal meningitis. In the 4-arm, 2-step clinical meeting conducted all MSG/ACTG, 93% of deaths occurring within the willingly two weeks of attitude and 40% of deaths occurring surrounded by weeks 3 and 10 were associated by all of increased intracranial pressure.
Cutaneous cryptococcal diseases
Cutaneous cryptococcosis is a under write of dissemination disclose in truly 10% of cases and commit precede lifethreatening epidemic by part of weeks. The lesions depart greatly in morphology and steal many distinct dermatologic entities. They make out be misdiagnosed as Molluscum contagiosum. The lesions commit appear as papules, tumours, vesicles, plaques, abscesses, cellulitis, purpura, draining sinus, ulcers, bullae, or subcutaneous swelling.
Other manifestations
It has been postulated that Cryptococcus may create out of thin air dormant in the prostate and mean as the dealer of systemic lapse after end of the line of therapy. Given that approximately patients by the whole of cryptococcosis are fungemia, it is not out the blue that there are reports of infection in many tool systems, including C. myocarditis, arthritis and gastroenteritis [32-36].
Discussion
Cryptococcus a fungus abundantly found in soil all over the world. It is commonly present in the environment so most peoples breathe in the microscopic airborne spores. Sometimes it shows the same symptoms as of respiratory infection and sometimes no symptoms are observed at all. C. neoformans and C. gattii have soon been isolated into diverge species, although roughly clinical laboratories will not commonly identify Cryptococcus to the species freely. C. gattii has afresh been reprehensible for a never ending outbreak of cryptococcosis in externally immunocompetent humans and animals on Vancouver Island and surrounding areas within Canada and the Northwest America and the ministry of C. gattii virus in immunocompetent hosts needs impending specifically addressed. Similarly, the human immunodeficiency parasite (HIV) pandemic continues, and cryptococcosis is a masterpiece opportunistic pathogen worldwide, anyhow its administration smoothly depends on the medical resources at hand to clinicians in specific regions. In the era of highly active antiretroviral attitude (HAART), the management of cryptococcosis has acquire consolidate of firm antifungal regimens together by all of aggressive benefit of the concealed disease. The incidence and mortality of this plague are again extremely fancy in areas where uncontrolled HIV contagion persists and limited retrieve to HAART and/or health assistance occurs. Cryptococcemia regularly precedes CNS invasion and make out seek for an extended life of predate (1 week to 16 weeks) still treatment. CNS invasion may be inconsequential to haematogenous plague or may delineate reactivation contagion evocative to histoplasmosis or tuberculosis. Adrenal scarcity may occur slight to cryptococcal armed intrusion of the adrenal glands. CT scanning should be performed in patients mutually a diagnosis of adrenal insufficiency to manage the breadth and contexture of the adrenal glands. If no distinctive aetiology is hinge on, an adrenal biopsy should be performed to manage for fungal or mycobacterial disease. Headache commit be the unaccompanied symptom as presenting highlight of cryptococcal meningitis in HIV. Prime immunodeficiencies (e.g. hyperimmunoglobulin M infection and severe combined immunodeficiency syndrome) and certain malignancies (e.g. slick lymphoblastic leukemia and sarcomas). Both deserted pulmonary and CNS cryptococcosis has been described in children without a familiar immunodeficiency. Neonatal cryptococcosis has been declared, and solid transmission has been coming. Fluconazole (200 mg using day orally), Itraconazole (200 mg twice for day orally drug level monitoring nicely advised). AmBd (1 mg/kg using week IV); this is minority effective than azoles and is associated mutually IV catheter related infections; consider for azole intolerant individuals. Initiate HAART 2 weeks to 10 weeks afterwards commencement of initial antifungal treatment Consider discontinuing suppressive therapy around HAART in patients mutually a CD4 cell weigh 1100 cells/mL and an undetectable or literally low HIV RNA directly sustained for 3 months (minimum of 12 months of antifungal therapy) clear reinstitution of alleviation therapy if the CD4 cell has a lot to do with decreases to 100 cells/mL.
Conclusion
In force, nimble cryptococcal meningitis should be treated mutually amphotericin B (0.7 mg/kg/day) among disparate things Flucytosine (100 mg/kg/day in cut apart doses) for two weeks, followed by Fluconazole (400 mg daily) for 8 weeks, followed by recurrent suppression by all of fluconazole (200 mg daily). Patients who have had immunologic reaction on ART by the whole of sustained CD4 counts >100 cells/μL make out be experienced to suspend maintenance therapy. This is in agreement by the whole of the pursue guidelines preferred by the MSG Cryptococcal Subproject and the USPHS. Further studies are rightfully to penetrate them consider of other antifungals or aggregation antifungals and immunomodulating agents a well-known as monoclonal antibodies and gamma interferon in the champion management of cryptococcal meningitis. Clearly, the brutal management of added intracranial oblige plays a practice contributing way of life in impartial risk, along mutually others patients with opening CSF pressures >250 mm H2O should have serial lumbar punctures simultaneously pressures have normalized. Although infinite studies have discovered the clinical efficacy of Fluconazole sterilization for systemic fungal infections, this strategy commit be approximately effective in countries where ART is unavailable.
Acknowledgement
All Authors wishes to acknowledge mam Maria Ayub lecturer of pharmacology in Jinnah University for women for great guidance and for providing studies outline.
Disclosure
Authors declare no conflict of interest.
References
- Saag MS, Graybill RJ, Larsen RA, Pappas PG, Perfect JR, et al. (2000) Practice guidelines for the management of cryptococcal disease. Infectious Diseases Society of America. Clin Infect Dis 30: 710-718.
- Shoham S, Cover C, Donegan N, Fulnecky E, Kumar P, et al. (2005) Cryptococcus neoformans meningitis at 2 hospitals in Washington, D.C.: Adherence of health care providers to published practice guidelines for the management of cryptococcal disease. Clin Infect Dis 40: 477-479.
- Dromer F, Bernede-Bauduin C, Guillemot D, Lortholary O (2008) Major role for amphotericin B-flucytosine combination in severe cryptococcosis. PLoS One 3: e2870-2008.
- Kwon-Chung KJ, Boekhout T, Fell JW, et al. (2002) Proposal to conserve the name Cryptococcus gattii against C. hondurianus and C. bacillisporus (Basidiomycota, Hymenomycetes, Tremellomycetidae). Taxon 51: 804-806.
- Kidd SE, Hagen F, Tscharke RL, Huynh M, Bartlett KH, et al. A rare genotype of Cryptococcus gattii caused the Cryptococcus is out break on Vancouver Island (British Columbia, Canada) 101: 17258-17263.
- Mirza SA, Phelan M, Rimland D, Graviss E, Hamill R, et al. (2004) The changing epidemiology of cryptococcosis: An update from population-based active surveillance in 2 large metropolitan areas, 1992-2000. Clin Infect Dis 36: 789794.
- Chen SC (2002) Cryptococcosis in Australasia and the treatment of cryptococcal and other fungal infections with liposomal amphotericin B. J Antimicrob Chemother 49: 57-61.
- van Elden LJ, Walenkamp AM, Lipovsky MM, Reiss P, Meis JF, et al. (2000) et al. Declining number of patients with cryptococcosis in the Netherlands in the era of highly active antiretroviral therapy. AIDS 14: 2787-2788.
- Dromer F, Mathoulin S, Dupont B, Laporte A (1996) Epidemiology of cryptococcosis in France: A 9 year survey (1985-1993). French Cryptococcosis Study Group 23: 82-90.
- Hakim JG, Gangaidzo IT, Heyderman RS, Mielke J, Mushangi E, et al. (2000) Impact of HIV infection on meningitis in Harare, Zimbabwe: A prospective study of 406 predominantly adult patients. AIDS 14: 1401-1407.
- Park BJ, Wannemuehler KA, Marston BJ, Govender N, Pappas PG, et al. (2009) Estimation of the current global burden of cryptococcal meningitis among persons living with HIV/AIDS. AIDS 23: 525-530.
- Nath DS, Kandaswamy R, Gruessner R, Sutherland DE, Dunn DL, et al. (2005) Fungal infections in transplant recipients receiving alemtuzumab. Transplant Proc 37: 934-936.
- Hage CA, Wood KL, Winer-Muram HT, Wilson SJ, Sarosi G, et al. (2003) Pulmonary cryptococcosis after initiation of anti-tumor necrosis factor-alpha therapy. Chest 124: 2395-2397.
- Dromer F, Mathoulin-Pelissier S, Launay O, Lortholary O (2007) Determinants of disease presentation and outcome during cryptococcosis: The CryptoA/D study. PLoS Med 20074: e21.
- Lortholary O, Poizat G, Zeller V, Neuville S, Boibieux A, et al. (2006) Long-term outcome of AIDS-associated cryptococcosis in the era of combination antiretroviral therapy. AIDS 20: 2183-2191.
- French N, Gray K, Watera C, Nakiyingi J, Lugada E, et al. (2002) Cryptococcal infection in a cohort of HIV-1-infected Ugandan adults. AIDS16: 1031-1038.
- Chayakulkeeree M, Perfect JR. (2006) Cryptococcosis. Infect Dis Clin North Am 20: 507-544.
- Pitisuttithum P, Negroni R, Graybill JR, Pappas P, Bustamante B, et al. (2005) Activity of posaconazole in the treatment of central nervous system fungal infections. J Antimicrob Chemother 56: 745-755.
- Perfect JR, Marr KA, Walsh TJ, Greenberg RN, DuPont B, et al. (2003) Voriconazole treatment for less common, emerging or refractory fungal infections. Clin Infect Dis 36: 1122-1131.
- Leenders AC, Reiss P, Portegies P, Clezy K, Hop WC, et al. (1997) Liposomal amphotericin B (AmBisome) compared with amphotericin B both followed by oral fluconazole in the treatment of AIDS-associated cryptococcal meningitis. AIDS 11: 1463-1471.
- Brouwer AE, Rajanuwong A, Chierakul W, Griffin GE, Larsen RA, et al. (2004) Combination antifungal therapies for HIV-associated cryptococcal meningitis: A randomised trial. Lancet 363: 1764-1767.
- Fraser JA, Giles SS, Wenink EC, Geunes-Boyer SG, Wright JR, et al. (2005) Same-sex mating and the origin of the Vancouver Island Cryptococcus gattii outbreak. Nature 437: 1360-1364.
- Canadian Task Force on the Periodic Health Examination (1979) The periodic health examination. Can Med Assoc J 121: 1193-1254.
- Field MJ, Lohr KN (1990) Institute of Medicine Committee to Advise the Public Health Service on Clinical Practice Guidelines, clinical practice guidelines: Directions for a new program. Washington, DC: National Academy Press
- Bicanic T, Meintjes G, Wood R, Hayes M, Rebe K, et al. (2007) Fungal burden, early fungicidal activity and outcome in cryptococcal meningitis in anti-retro viral naive or antiretroviral-experienced patients treated with amphotericin B or fluconazole. Clin Infect Dis 45: 76-80.
- Saag MS, Powderly WG, Cloud GA, Robinson P, Grieco MH, et al. (1992) Comparison of amphotericin B with fluconazole in the treatment of acute AIDS-associated cryptococcal meningitis. The NIAID Mycoses Study Group and the AIDS Clinical Trials Group. N Engl J Med 326: 83-89.
- van der Horst CM, Saag MS, Cloud GA, Hamill RJ, Graybill JR, et al. (1997) Treatment of cryptococcal meningitis associated with the acquired immunodeï¬ÂÂÂÂciency syndrome. National Institute of Allergy and Infectious Diseases Mycoses Study Group and AIDS Clinical Trials Group. N Engl J Med 337: 15-21.
- Bennett JE, Dismukes WE, Duma RJ, Medoff G, Sande MA, et al. (1979) A comparison of amphotericin B alone and combined with flucytosine in the treatment of cryptoccal meningitis. N Engl J Med 301: 126-131.
- Dismukes WE, Cloud G, Gallis HA, Kerkering TM, Medoff G, et al. (1987) Treatment of cryptococcal meningitis with combination amphotericin B and flucytosine for four as compared with six weeks. N Engl J Med 317: 334-341.
- Bicanic T, Wood R, Meintjes G, Rebe K, Brouwer A, et al. (2008) High-dose amphotericin B with flucytosine for the treatment of cryptococcal meningitis in HIV-infected patients: a randomized trial. Clin Infect Dis 47: 123-130.
- Sharkey PK, Graybill JR, Johnson ES, Hausrath SG, Pollard RB, et al. (1996) Amphotericin B lipid complex compared with amphotericin B in the treatment of cryptococcal meningitis in patients with AIDS. Clin Infect Dis 22: 315-321.
- Baddour LM, Perfect JR, Ostrosky-Zeichner L (2005) Successful use of amphotericin B lipid complex in the treatment of cryptococcosis. Clin Infect Dis 40: 409-413.
- Coker RJ, Viviani M, Gazzard BG, Du Pont B, Pohle HD, et al. (1993) Treatment of cryptococcosis with liposomal amphotericin B(AmBisome) in 23 patients with AIDS. AIDS 7: 829-835.
- Hamill R, Sobel J, El-Sadr W, et al. (1999) Randomized double-blind trial of ambisome and amphotericin B in acute cryptococcal meningitis in AIDS patients [abstract 1161]. In: Program and abstracts of the 39th Interscience Conference on Antimicrobial Agents and Chemotherapy (San Francisco). Washington, DC: American Society for Microbiology.
- Larsen RA, Bozzette SA, Jones BE, Haghighat D, Leal MA, et al. (1994) Fluconazole combined with flucytosine for treatment of cryptococcal meningitis in patients with AIDS. Clin Infect Dis 19: 741-745.
- Mayanja-Kizza H, Oishi K, Mitarai S, Yamashita H, Nalongo K, et al. (1998) Combination therapy with fluconazole and flucytosine for cryptococcal meningitis in Ugandan patients with AIDS. Clin Infect Dis 26: 1362-1366.

