Allan Fernando Delcid Morazan1*, Sendy Janneth Vides Torres1, Moran E Barcan Batchvaroff1, Delmy Soraya Barahona Andrade2, Wendy Patricia Barahona Zelaya2 and Ronald Emilio Mayorga Izaguirre2
1Doctor of Medicine and Surgery, National Autonomous University of Honduras, Honduras
2Medico en Servicio Social, National Autonomous University of Honduras, Honduras
*Corresponding Author:
Allan Fernando Delcid Morazan
Doctor of Medicine and Surgery
National Autonomous University of Honduras, Honduras
E-mail: allanferdelcid@hotmail.com
Received Date: March 22, 2017; Accepted Date: March 24, 2017; Published Date: April 02, 2017
Citation: Morazan AFD, Torres SJV, Batchvaroff MEB, et al. Collodion Baby: Case Report. J Healthc Commun. 2017, 2:2. doi: 10.4172/2472-1654.100056
Keywords
Collodion baby; Honduras; Ichthyosis; Newborn
Introduction
Ichthyosis is an uncommon clinical condition, with a worldwide occurrence of 1: 300,000 births, the incidence of newborns with the clinical phenotype of ichthyosis in Latin America is unknown, but it is estimated to be present in approximately 1: 250,000 newborns; being an uncommon dermatosis. Since the introduction of the term baby collodion, approximately 270 cases have been reported in medical literature. Alterations in cornification (ichthyosis) are a prominent group of hereditary diseases, which are characterized clinically by desquamation patterns and histopathologically by hyperkeratosis. In most cases, there is a family history of the disease or consanguinity. In turn, it may present with acquired disorders. They are distinguished by their mode of inheritance, clinical characteristics, associated defects and histological findings [1-6]. Several classifications of this pathology are known, Traupe proposed to divide them into vulgar, when the clinic is incipient at birth and congenital when they are marked at the time of birth [2]. As for neonatal presentations, we find that the collodion are normally born premature, wrapped in a layer that resembles cellophane, usually in association with ectropion and eclabium accompanied by trichothiodystrophy. The collodion membrane breaks off between the 1st and 4th week of life, evidencing the definitive phenotype. 60% of the cases correspond to the initial expression of Congenital Ichthyosiform Erythroderma or Lamellar Ichthyosis, however, 10% will have normal skin after resolution of the collodion membrane [3,4]. Other presentations include Ichthyosis Harlequin, Linked to Chromosome X, Erythroderma Ichthyosiform congenital blister and Nethertan Syndrome.
The main manifestations include ectropion (eversion of the eyelids), eclabium (everted lips) and hypoplasia of nasal bones, auricular pavilions, fingers and toes. Skin manifestations often worsen in cold or dry environments. They usually present at birth with severe erythroderma, slight desquamation and bulla or large erosions that are distributed mainly in the trunk and limbs, which evolve to extensive denuded, moist, painful and ill smelling areas [5].
Prenatal diagnosis is possible and should be evaluated, if the mother wishes, when there is a family history with a genetic pattern that makes transmission possible. The techniques to be used may include amniocentesis, villus biopsy, fetal skin biopsy, blood and urine analytical studies, both enzymatic and genetic diagnostic techniques and prenatal diagnosis are subject to continuous improvement and should be indicated and evaluated by experts. The diagnosis of a case of ichthyosis should be followed by genetic counselling, reporting on the possibility of recurrence of the disease in successive pregnancies of the mother and the risk of transmission of the disease by the patient, siblings and other relatives [2].
Among the main complications that can lead to the death of a newborn with ichthyosis, pyoderma, sepsis from respiratory origin or due to an interventional approach, uncontrollable hypothermia, hypernatremia dehydration due to excessive evaporation and transepidermal loss of water are known, although the two leading causes of death in these babies are due to prematurity and absence of protective skin function as a barrier [6]. In addition, these patients are associated with atopic dermatitis, asthma and allergic rhinitis, since the alteration of the skin barrier predisposes them to a greater allergic sensitization [4].
The early treatment consists of maintaining the body temperature by placing the newborn in an incubator with humidifier, skin care and above all pain treatment. Patients suffering from severe forms of Ichthyosis benefit from a humid environment and electrolyte balance control [7]. Intravascular hydration through the peripheral pathway is not recommended due to the characteristic lesions of these patients, it is usually recommended by umbilical vascular catheterization, which is less related to infections [3]. Topical treatments such as urea, alpha hydroxy acids, mainly lactic acid and propylene glycol, vegetable oils such as petroleum jelly and topical retinoid are used [2]. The solutions that are contraindicated in these patients are silver sulfate which is related to agranulocytosis and baths with chlorhexidine because of its toxic potential [3].
Clinical Case
A preterm female newborn, daughter of a 23-year-old mother who attended 4 prenatal check-ups at the health center, which were started until the third trimester of pregnancy, all attentions were given by a nurse, and an obstetrical ultrasound was not performed nor indicated during the pregnancy. According to the prenatal card adequate weight growth is reported, as far as the personal history of the parents they did not report exposure to toxic substances or X-rays, it is only said that the mother had an untreated urinary tract infection during the sixth month of pregnancy and a generalized dermatitis in the eighth month. Both parents deny a history of ichthyosis in the family tree and deny consanguinity. This is the mother´s second pregnancy; the first was an abortion of which details are unknown. She began with active labour at the 35 weeks of gestation according to the date of last menstruation, moment in which she was admitted to labour and delivery room, proceeding to a dystocic delivery due to pelvic presentation. The newborn had an Apgar score of 6 and 8 at the first and fifth minutes, weight 2200 g, cephalic perimeter 32 cm, length 46 cm, chest perimeter 30 cm and 28 cm abdominal perimeter, heart rate 157 beats per minute, respiratory rate 70 breaths per minute, Silverman Anderson score 1 (barely visible intercostal retractions).
On physical examination, a constrictive, tense membrane resembling an oily parchment or collodion covering the whole body surface was found at birth (Figure 1). Eyelid ectropion, biomorphic appearance of the ears and nose by flattening of these and O-shaped configuration of the lips (Figure 2). Skin of neck and trunk with fissures (Figure 3), anterior fontanelle without any compromise, lungs with symmetrical air inlet without presence of pathological sounds, heart sounds with good tone and intensity, without murmurs. Abdomen soft not distended, without presence of visceromegaly. Genitals in accordance to age and sex, symmetrical and complete limbs, joints with preserved mobility, with gestational age of 35 weeks by Capurro Test.
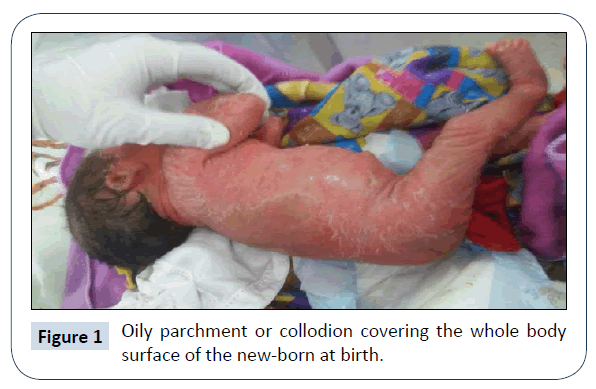
Figure 1: Oily parchment or collodion covering the whole body surface of the new-born at birth.
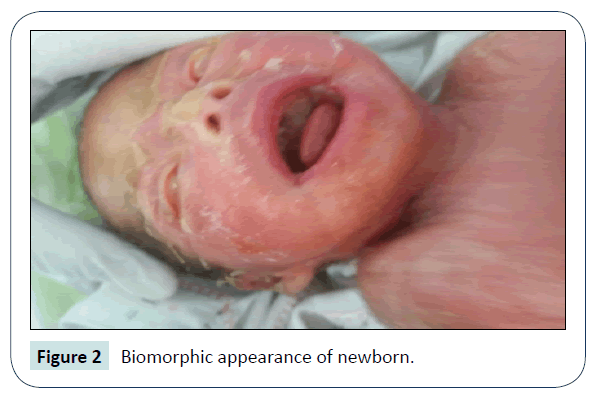
Figure 2: Biomorphic appearance of newborn.
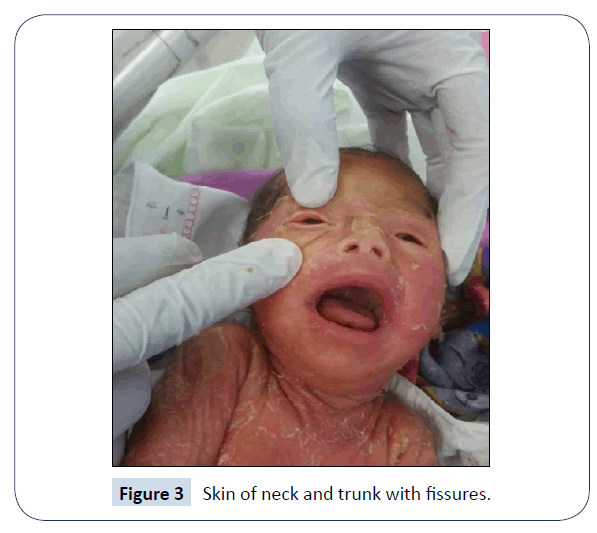
Figure 3: Skin of neck and trunk with fissures.
The patient is admitted to the neonatal intensive care unit, where several laboratory studies are performed, including blood, urine and umbilical secretions with normal results. Complete blood count reported leukocytes 163 × 109/L, neutrophils 54.3% and lymphocytes 37.5%, haemoglobin 11.9 mg/dl, haematocrit 34.5% and platelets 262,000, glucose level and PCR within normal ranges; according to these results it was decided to manage the patient with ampicillin and amikacin, the skin lesions were covered with cream based on vitamin E, panthenol and hyaluronic acid. Intravenous hydration was administered via peripheral route and the newborn was maintained in radiantheat cradle at a suitable temperature to avoid hypothermia and in a sterile environment to avoid infections.
Due to the suspicion of ichthyosis and the need for optimal neonatal care and given the high likelihood of complications it was decided to transfer the patient to a hospital with a higher level of care; where services in the areas of paediatric dermatology, neonatology and genetics were available.
Discussion
The first description of Ichthyosis was made by Rev. Oliver Hart in Charleston, South Carolina in 1750. It owes its name to the appearance of the skin presented by newborns [7]. It is known that they are a group of congenital disorders with cutaneous manifestations, which may or may not be associated with other genetic defects, and where their characteristics are the alterations of the skin, which are relevant for the recognition of the pathology and its adequate approach. Sepsis is its most severe manifestation, concomitantly severe dehydration secondary to transepidermal water loss, which leads the patient to an electrolyte imbalance can be found [8].
In Honduras this is the second case reported at national level between 2011 and 2017 and the first in the southern region of the country to be known of. A recently emerged group of Spanish dermatologists with an important interest in this pathology have conducted an epidemiological study on the prevalence of Ichthyosis; according to the results of their study, it is believed that the prevalence of Ichthyosis in Spain ranges between 7.2 and 16.2 cases per million children born. It is also estimated that 71% of patients are not followed up in specialized consultations, 92% of them are without genetic diagnosis, and 78% are not members of the Spanish Association of Ichthyosis, which currently has about 80 members registered among all types of Ichthyosis [9].
The findings during the physical examination of our case are consistent with other cases of baby collodion, in the literature it is described that it is frequent to find these patients wrapped in a layer that resembles cellophane accompanied by ectropion, eclabium and hypoplasia of nasal bones, ears, fingers and toes [4]. Data on the importance of an ultrasound during pregnancy are unknown for the diagnosis or treatment of this condition, which in this case could not be assessed due to the patient's lack of resources to perform this study during pregnancy. No other study was performed due to poor prenatal control and the lack of suspicion during the pregnancy. In the present case, it was possible to establish the clinical diagnosis, however, due to the condition, which represented a potential risk of infection and because there was no specialist in the area of pediatric dermatology, neonatology and genetics, the patient was referred to a hospital of higher level. Although it is known that this is not a curable disease, it is possible to perform a proper medical intervention and also approach in the psychological and genetic component involving both the patient and the parents to face the disease in the best possible way [7].
Quality of life should be a fundamental part in the treatment of these patients, because the marginalization they suffer from society and even doctors, may cause depression, anxiety and in some cases suicidal ideation, if they do not have people by their side to help them understand the disease or belong to a self-help group, evolution may be unsatisfactory [10].
Ethics
The authorization of publishing this article was granted through the informed consent, signed and approved by the patient legal guardians. The authors declare no conflicts of interest with the publication of this article.
References
- Morelli JG (2013) Trastornos de la Queratinización. In: Robert Kþ Kliegman Robert M, Behrman Richard E, Behrman Richard E (eds.) Nelson Tratado de Pediatria(2) 19a edn. España: Elsevier pp: 2344-2350
- https://www.aeped.es/sites/default/files/documentos/ictiosis.pdf
- Craiglow BG (2014) Ichthyosis in the new-born. NIH 37: 26-31.
- Nadia VA (2016) Aranibar Duranb Ligia. Ictiosis hereditaria: desafío diagnóstico y terapéutico. Rev Chil Pediatr 87: 213-223.
- Olmos Jiménez MJ, González Fernández A, Valverde-Molina J, Díez Lorenzo MP (2014) Ictiosis arlequín. Pediatr 80: 263.
- Antonio PE, Gladys DPR (2017) Severe ichthyosis of the newborn: An Uncommon. Pathology 2: 56-59.
- Gustavo AAM, del Carmen MM, Carolina BM, Aracely CD, César RM, et al. (2017) Ichthyosis harlequin: report of a case in Honduras and review of the literature. Rev Med Hondur 79: 199-202.
- Joaquin SD, Maria Jose SS, Cristian SD, Vanesa RC, Francisco CC (2017) Ictiosis congénita laminar, reporte de un caso.
- https://www.ictiosis.org/sobre_asic/info_asic/files/ictiosis_8.pdf
- https://piel-l.org/libreria/item/645

