Keywords
Breast cancer; Health promotion; African American women; Public health; Communication; Health crises; Mammography
Introduction
Breast cancer prevention and spiritual wellbeing among African American Women
Breast cancer is the most common cause of cancer and second leading cause of cancer death in the United States (US) among women. The American Cancer Society (ACS) estimated that 231,840 women in the US would be diagnosed with invasive breast cancer and that 40,290 would die from the disease in 2015 [1].
Breast cancer morbidity and mortality are disproportionate among African American women when compared to White women and other racial groups [2,3]. The incidence of breast cancer increased between 2008 and 2012 among African American women (0.4%) but was stable among White, Hispanic and American Indian and Alaska Native women [1]. Although White women overall are more likely to develop breast cancer, African American women are more likely to have breast cancer before age 45 and die from it at any age [1]. Persistent cancer morbidity and mortality rates among this population have challenged health promoters and medical providers to address a long-standing health disparity. Culturally appropriate health promotion programs designed for African American women are needed to complement existing programs. These programs include cultural components that may be appealing to African American women but they are often cursory and deficient of elements that will bolster appeal of health promotion materials and messaging.
Spirituality, a multi-dimensional construct that is defined as the intrinsic value of connecting with a higher power and involving a transcendent force [4-6], is considered a critical component of health promotion by many public health organizations both nationally and globally [7,8] and has received increased attention over the past four decades [9-11]. Spirituality in healthcare (e.g. prevention to palliative care) has spurred an evolution of a culture that attempts to provide linkages to understanding, explaining and predicting spiritual coping and well-being along the continuum of care among various populations [12].
Spirituality has also shown to be effective in health promotion among African American women [13,14]. Health promotion efforts that include a framework for spiritual well-being increase effectiveness and also have potential to positively impact health behavior when compared to cursory strategies. The multidimensional aspects of spirituality provide a platform for diverse and in-depth promotion that appeal on multiple levels. The elements of spirituality in breast cancer screening promotion among African American women become an integrative measure of health and well-being that captures both religious and existential well-being [15]; strengthens cultural appropriateness [16] and also emphasizes the importance of socio-cultural values [17].
Project joy, a cardiovascular health promotion intervention, included a sample of 579 African American women 40 and older who were randomized to spiritual and non-spiritual groups. Women randomized to the spiritual intervention groups had significantly better cardiovascular outcomes when compared to those who were randomized to the non-spiritual group. Participants in the spiritual groups had significantly reduced blood pressure, dietary fat and sodium intake [18]. This and other public health promotion programs are only a few examples of incorporating socio-cultural factors into a health promotion program for African American women [19].
The value of including and infusing culturally appropriate factors into multiple levels of health promotion also has potential to strengthen and broaden reach and impact. There is scant research that investigates the effectiveness of spiritual well-being in mass mediated communication to address cancer disparities among African American women. Emerging studies show that popular mass media (i.e., internet, magazines, television, and radio) among African American women are avenues to complement and broaden the reach and depth of health promotion efforts [20-22]. Strategic placement of spiritual well-being into public health promotion efforts, much like the strategic placement of health promotion components into individual, group and organizationallevel health promotion, may re-emphasize the importance of cancer screening among the target audience. The health promoter utilizes the media as an avenue or channel to strategically position cancer communication and disseminate specific messaging that is culturally appealing to African American women about breast cancer risk and prevention on a mass societal level [23].
Currently, there are few studies that have investigated the utility and incorporation of spiritual well-being in mass-mediated health promotion targeting minority populations. Many African American women consume health messages through the mass media [25]; self-report spirituality as impactful to their health and well-being; and are receptive to spiritual well-being components in health promotion for health crises, prevention of cancer and other health conditions [14,24-26]. It is plausible that the inclusion of spiritual well-being in public health promotion via the mass media would have a positive impact on the efficacy of breast cancer screening initiatives among African American women. The following exploratory research questions and hypotheses were advanced to investigate African American women’s spiritual well-being and its associations with media exposure to breast cancer screening information and attitudes toward breast cancer screening:
RQ1: Are there significant predictive relationships among African American women’s spiritual well-being, media exposure to breast cancer screening information, and attitudes toward breast cancer screening?
H2a: African American women who have higher levels of spiritual well-being pay more attention to breast cancer screening information in the media.
H2b: African American women who have higher levels of spiritual well-being are more knowledgeable about breast cancer and have more positive attitudes toward breast cancer screening (i.e., more perceived benefits and less perceived barriers of mammography).
H2c: African American women who are more exposed to breast cancer screening information via the mass media are more knowledgeable about breast cancer and have more positive attitudes toward breast cancer screening.
H2d: The influences of spiritual well-being on knowledge about breast cancer and attitudes toward breast cancer screening are mediated via breast cancer screening media exposure among African American women.
Method
Participants and procedures
This survey data were collected from a convenience sample of African-American women residing in the Midwest. Eligible individuals were recruited through advertisements at church services and events, referrals from pastors and church leaders, and a flyer disseminated at several churches and community centers in Kansas and Missouri. The recruitment occurred at two time points. Sixty-five individuals were recruited in 2006, as a part of a larger study that investigated the impact of spirituality and religion in processing messages in breast cancer screening advertisements and can be found elsewhere [27]. An additional 33 individuals were recruited in 2008 to yield a larger sample size (and thus greater power) for the current study. The participants were African American women (N=98) between 18 and 78 years of age and were given a $30 incentive for their participation in the study. The research protocol was approved by the Institutional Review Board at the University of Missouri and the University of Kansas.
Measures
Spiritual well-being
The Spiritual Well-Being Scale (SWBS) [15], one of the most widely recognized spirituality scales, was utilized to assess respondents’ perceptions on spirituality quality of life. Paloutzian and Ellison [28] argued that it is important to address one’s well-being with respect to his/her subjective experience and relationships with a transcendent being and others. This 20-item scale originally has two subscales: Religious Well-Being (RWB) that examines one’s relationship with the Christian God, and Existential Well- Being (EWB) that explores his/her connection to others as well as general satisfaction and meaning in life. Example items include “I believe that God loves me and cares about me,” “I feel very fulfilled and satisfied with life,” and “I don’t find much satisfaction in private prayer with God.” Responses are recorded on a Likert scale ranging from 1 (strongly disagree) to 6 (strongly agree). The reliability and internal consistency of the SWBS have been supported—test-retest reliability of 0.93 (SWB), 0.96 (RWB), and 0.86 (EWB) [29], and Cronbach α of 0.76 to 0.93 (SWB), 0.87 to 0.91 (RWB), and 0.78 to 0.91 (EWB) [30-32]. It should be noted that the participants recruited in 2006 responded on a 5-point Likert scale instead of the original 6-point scale. Their responses were recoded/weighted to have a metric as close as possible to the responses from other participants who used the original scale. Cronbach α in the current study was 0.98 for the SWB, and 0.95 for the RWB and 0.98 for the EWB.
Knowledge, attitudes and beliefs about breast cancer
Measures also included in the study were knowledge about breast cancer screening and beliefs toward breast cancer screening. Knowledge about breast cancer screening was included to gauge how involved participants were with breast cancer screening. Breast cancer screening belief measures [32], and breast cancer screening attitudinal measures were modified and expanded to measure a specific set of respondent beliefs about breast cancer screening a priori. The measures included 8 items that measured four dimensions (factors) of breast cancer screening knowledge and beliefs: perceived benefit of mammography, perceived benefit of breast self-exams and perceived barriers to mammography. Example items include “Having a mammogram will help me find breast lumps early” and “I am afraid to find out something is wrong when I have the mammogram.” Participants responded on a Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). Champion and Scott [32] investigated the psychometric properties of breast cancer beliefs in a large sample of African-American women and found adequate reliability and internal consistency (test-retest reliability = 0.40–0.68, Cronbach α = 0.65–0.90) and construct validity.
Breast cancer screening media
Exposure Respondents also indicated their exposure to breast cancer screening information through the media, by answering to a single item “Indicate how often [you] pay attention to breast cancer information in the media” with five response options (1: Never; 2: Seldom; 3: Occasionally; 4: Often; 5: A lot).
Analytic Procedures
Data were analyzed in two steps. First, confirmatory factor analysis (CFA) was conducted for the SWBS to confirm that the measurement model fits well and to explore factor and correlation structures to ensure the necessary preconditions for parceling [33,34]. Parceling is the mean aggregation of two or more items for the purpose of creating more parsimonious CFA models [34]. Parceling also provides psychometric benefits, such as improved reliability and internal consistency as well as closer approximation to normality [35]. We constructed six parcels from the 20 SWBS items (3 parcels per subscale) by counterbalancing the factor loadings derived from an initial model. The parceled model was tested for use in all subsequent analyses.
Second, structural equation modeling (SEM) was conducted to evaluate the predictive relationships and potential mediations among the study variables. More specifically, an SEM model was hypothesized that African American women’s exposure to breast cancer screening information through the media (mediator) would mediate the influences of spiritual well-being (predictor) onto their knowledge about breast cancer and perceived benefits and barriers of mammography (outcomes). As depicted in Figure 1, this model included all direct effects of the predictor on the mediator (denoted by a; Hypothesis 2a) and outcomes (c′’s; Hypothesis 2b) as well as all direct effects of the mediator on the outcomes (b’s; Hypothesis 2c). Also included were all possible indirect effects of the predictor on the outcomes through the mediator (ab’s; Hypothesis 2d) [36]. The outcomes were allowed to correlate each other in the model.
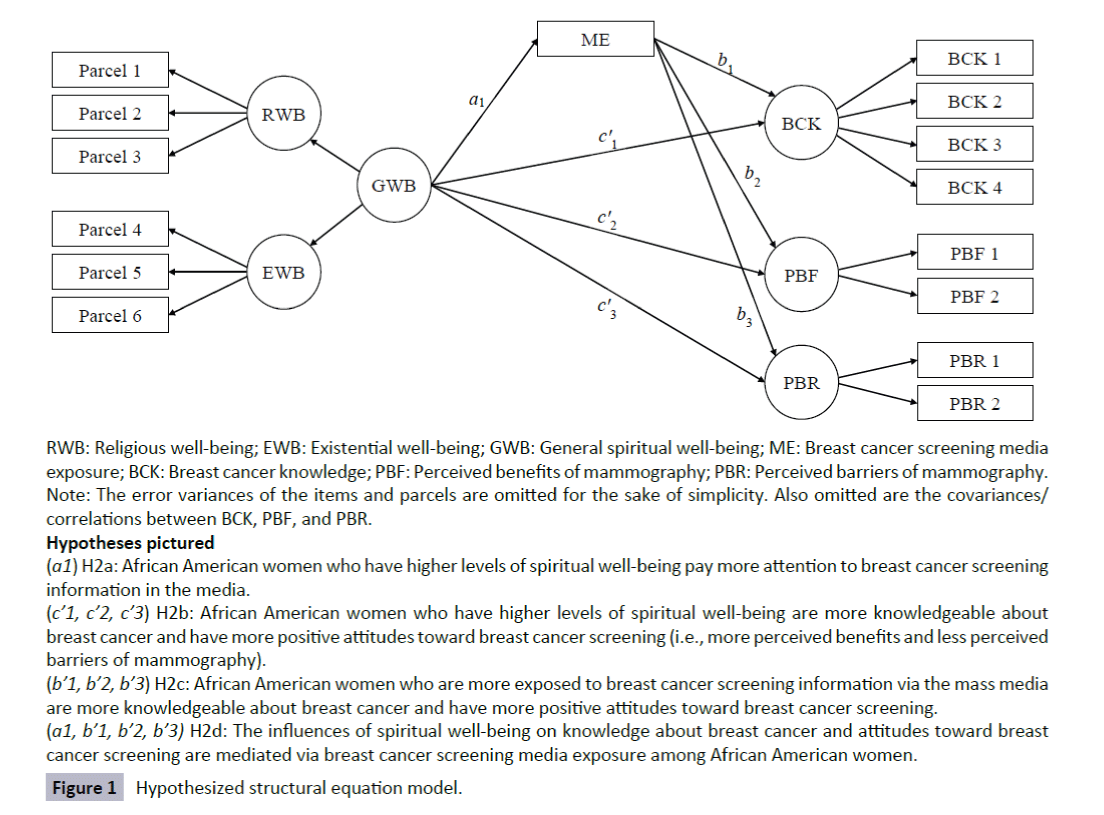
RWB: Religious well-being; EWB: Existential well-being; GWB: General spiritual well-being; ME: Breast cancer screening media exposure; BCK: Breast cancer knowledge; PBF: Perceived benefits of mammography; PBR: Perceived barriers of mammography. Note: The error variances of the items and parcels are omitted for the sake of simplicity. Also omitted are the covariances/ correlations between BCK, PBF, and PBR.
Hypotheses pictured
(a1) H2a: African American women who have higher levels of spiritual well-being pay more attention to breast cancer screening information in the media.
(c’1, c’2, c’3) H2b: African American women who have higher levels of spiritual well-being are more knowledgeable about breast cancer and have more positive attitudes toward breast cancer screening (i.e., more perceived benefits and less perceived barriers of mammography).
(b’1, b’2, b’3) H2c: African American women who are more exposed to breast cancer screening information via the mass media are more knowledgeable about breast cancer and have more positive attitudes toward breast cancer screening.
(a1, b’1, b’2, b’3) H2d: The influences of spiritual well-being on knowledge about breast cancer and attitudes toward breast cancer screening are mediated via breast cancer screening media exposure among African American women.
Figure 1: Hypothesized structural equation model.
The fit of the CFA and SEM models was evaluated with regard to both incremental and absolute fit using multiple indices: comparative fit index [37] and Tucker-Lewis index [38]; and root mean square error of approximation [39] (RMSEA), standardized root mean square error (SRMR), and weighted root mean square residual [40] (WRMR). CFI and TLI quantify the benefit of the hypothesized model over the null model of uncorrelated latent variables. A CFI or TLI value greater than 0.95 indicates a well-fitting model; and a value greater than 0.90 is considered an adequate fit [41]. RMSEA, SRMR, and WRMR examine the discrepancy between the observed and fitted covariance matrices. Unlike SRMR and WRMR, RMSEA also considers model complexity (i.e., sample size and degrees of freedom [df] of the model). In general, an RMSEA value less than 0.06 [41] or 0.07 [42] indicates good fit (< 0.08 = fair fit, < 0.10 = mediocre fit; [43]. An SRMR value less than 0.08 is generally considered a good fit [41]. WRMR is useful especially when the variables are in different scales (e.g., a mix of binary items and ordinal items as in our SEM model). A WRMR value less than 1.00 is considered as acceptable [44].
Missing data due to nonresponses (≤ 2% on individual items) were handled by an iterative Monte Carlo Markov Chain (MCMC) multiple imputation [45]. More specifically, the expectationmaximization (EM) algorithm provided prior estimates of missing values for a subsequent MCMC procedure which produced 200 imputed datasets. Then, modeling results from each of 200 imputed datasets were combined to make statistical inference [46]. All analyses were conducted using Mplus 7.0 [47].
Results
Sample demographics
The participants’ age was well distributed over the range of 18 to 69 years, and the majority was between 30 to 59 years old (67%). While 21% of the participants had less than or equal to high school education, 56% had some college or were college graduates; 23% had a post or advanced college degree. The majority of the participants had an income greater than $35,000 (54%); and 20% earned below $10,000 and 12% between $25,000 to $34,999.
Confirmatory factor analysis
The CFA results supported the psychometric properties of the SWBS, all standardized factor loadings were statistically significant (p < 0.001) and substantially large (> 0.90). The RWB items (parcels) produced relatively higher standardized loadings (> 0.96) and thus greater predictability, compared to the EWB items (range = 0.91–0.96). Given a high correlation between the religious well-being and existential well-being factors, they were re-parameterized in the final model as latent indicators of a higher-order factor, general spiritual well-being. The model fit values were satisfactory (CFI = 0.98, TLI = 0.97, SRMR = 0.01), except for RMSEA (0.15 [90% confidence interval = 0.08; 0.22]). Thus, the hierarchical SWBS model was reasonably accepted, and then incorporated into the SEM model to test our research hypotheses—i.e., predictions and mediations among spiritual well-being, breast cancer screening media exposure, perceived benefits and barriers of mammography.
Structural equation modeling
The hypothesized SEM model (Figure 1) provided an excellent fit (CFI = 0.97. TLI = 0.96, RMSEA = 0.03, WRMR = 0.55). The general spiritual well-being factor significantly predicted the breast cancer screening media exposure factor. The standardized estimate of this direct effect was negative (a1 = –0.23, SE = 0.10, p < 0.05), indicating that the participants who had higher levels of spiritual well-being were exposed to less information about breast cancer screening through the media (Hypothesis 2a). After controlling for media exposure, the general spiritual well-being factor was also related negatively to the breast cancer knowledge factor (c1′ = –0.46, SE = 0.25, p = 0.07; significant at 0.10 α level), and positively to the perceived benefits of mammography factor (c2′ = 0.85, SE = 0.06, p < 0.001). These results suggested that the participants with higher levels of spiritual well-being were less knowledgeable about breast cancer but have more positive attitudes toward breast cancer screening (see Hypothesis 2b). However, the participants’ spiritual well-being was not predictive of their perception about mammography barriers (c3′ = –0.02, SE = 0.21, p = 0.91).
The breast cancer screening media exposure factor was not a significant predictor of the outcomes—b1 = 0.34, SE = 1.49, p = 0.82 for the breast cancer knowledge factor; b2 = –0.05, SE = 0.14, p = 0.72 for the perceived benefits of mammography factor; and b3 = 0.01, SE = 0.21, p = 0.91 for the perceived barriers of mammography factor. Consequently, the influences of the general spiritual well-being factor could not be mediated or delivered through the breast cancer screening media exposure factor to those outcome factors (i.e., no mediations)—ab1 = –0.08, SE = 0.36, p = 0.83; ab2 = 0.01, SE = 0.03, p = 0.72; and ab3 = –0.001, SE = 0.05, p = 0.98, respectively.
Discussion, Implications and Conclusion
The purpose of the present study was to explore the utility of the Spiritual Well-Being Scale and its role in health promotion of breast cancer screening among African American women. The empirical, theoretical and practical implications and findings provide a framework for how SWBS fares among a pilot sample of African American women in faith-based (and affiliated) communities in the Midwest.
The SWBS did not show in this study to have predictive strength in health promotion among African American women but may provide a guide for how to use this measure with those women who are highly spiritual. Given that the integration of health and spirituality is prevalent among many documented research samples of African American women [48], it is reasonable that testing this measure in individual and group-level health promotion among African American women prior to masssocietal levels would be warranted. A limitation of the study included sample size; there was a relatively small sample (N = 98). Nevertheless, a post-hoc power calculation using the MacCallum, Browne, and Cai’s [44] procedure revealed that this study was adequately powered with the current sample size— the hypothesized SEM model with 81 df produced 0.82 power to reject the null hypothesis of acceptable fit (i.e., RMSEA of 0.08).
The analysis began with exploring the domains of the SWBS, a popular scale known for its reliability and validity but also questioned for its fit with minority groups [49]. The scale was confirmed as a two-factor solution scale with this pilot sample and CFA results supported the psychometric properties of the SWBS. There are also existing scales that measure spirituality among African Americans [50] however these scales do not necessarily include dimensions related to spiritual well-being – a component that is critical to health promoting behavior. The domains of the SWBS that include the RWB or Religious Well Being dimension that examines a vertical relationship or an individual’s relationship with the Christian God; and the horizontal relationship or Existential Well Being (EWB) dimension help explain the connection between an individual and others as well as general satisfaction and meaning in life [29]. Previous studies conducted with African American samples found that the structure of the SWBS did not adequately measure subjective well-being in regards to a spiritual domain of human functioning and called into question the validity of the scale among African Americans [49] and determined that a five-factor rather than a two-factor solution was an appropriate measure of spiritual wellbeing among this population [51].
Hypotheses that predicted spiritual well-being would predict breast cancer screening media exposure were not supported (Figure 1); participants who had higher levels of spiritual wellbeing were exposed to less information about breast cancer screening through the media. Consequently, the influences of the general spiritual well-being factor could not be mediated or delivered through the breast cancer screening media exposure factor to those outcome factors (i.e., no mediations) After controlling for media exposure, the general spiritual well-being factor was also related negatively to breast cancer knowledge, and to outcome measures (breast cancer knowledge, perceived benefits of mammography, perceived barriers of mammography). These results suggested that the participants with higher levels of spiritual well-being were less knowledgeable about breast cancer but had more positive attitudes toward breast cancer screening. However, the participants’ spiritual well-being was not predictive of their perception about mammography barriers. Given that the outcome variables included in the study of perceived barriers and perceived benefits of mammography were measured by two items each, this might provide only limited information or a partial picture about the constructs of our interest. Hence, it would be beneficial for future studies to develop and utilize more psychometrically validated measures of the variables.
Given the sample size, type (convenience) and also the time points in which data collection was made, additional studies must be conducted with a more representative sample to test validity and reliability and its impact on breast cancer screening among African American women. Qualitative studies may yield more contextual information from women about the type of breast health promotion that they are willing to pay attention to through the mass media. Quantitative studies may help to confirm these strategies and also identify direct and indirect impact on knowledge and attitudes toward breast cancer screening.
For public health researchers and health promotion practitioners, these empirical findings may guide future research and health promotion programming among African American women concerning breast cancer screening. African American women in this sample and other empirical research report that they are spiritual [52]. Spirituality, a construct that encompasses both existential and religious well-being, has shown to be an important factor in framing messages in breast cancer screening health communication [53] and also health education among African American women [53]. Spiritual well-being as a strategically embedded component into breast cancer screening health promotion has potential to reduce negative barriers to screening and enhance cancer prevention approaches among disproportionately impacted populations. Although hypotheses pertaining to spiritual well-being as a predictor of breast cancer media exposure were not supported in the present study, there is some evidence that these practices have potential to impact attitudes and beliefs among African American women based on current media practices [25]. Certain media outlets (e.g. magazines, targeted newspapers, newsletters) are positioned to cover relevant health issues such as breast cancer screening and also reach niche audiences through strategic selection of topics and appealing promotions writing. Spiritual well-being as a component of these health promotion strategies may have far reaching impact on delivery of health programs because of domains that align with spiritual experiences of African American women and African American culture and way of life. Other practical implications include opportunities health promotions personnel have to include community partners in the process of developing health promotions materials. These strategies at best will resonate with the target audience and serve as either the first step to awareness or a linkage to positive behavior outcome. Incorporating spiritual well-being into existing health promotion programs or using this factor as the framework for health promotion programming can serve as a tool to diversify health promotion programming for vulnerable persons on population, group and individual levels.
This investigation is only a starting point where health promotions and public health scholars may delve to see how spiritual wellbeing is conceptualized among minority populations and how it can be utilized to strategically place and frame health messages in the mass media. The strategic use of spiritual well-being is warranted in cancer screening promotion to influence this and other proactive health behaviors. This also provides health promotions professionals with an avenue to strengthen health promotion materials, public health interventions and programs that target African American women concerning breast cancer risk and prevention.
Acknowledgements
Candice Coffey and Pavel Panko
The project was conducted through the Frontiers: The Heartland Institute for Clinical and Translational Research at the University of Kansas.
References
- American Cancer Society (2015-2016) Breast Cancer Facts & Figures. Atlanta.
- CDC Cancer among women (2013) Centers for Disease Control and Prevention.
- Siegal R, Naishadham D, Jemal A (2013) Cancer Statistics. CA Cancer J Clin 63: 11-30.
- Koenig HG, Larson DB, McCullough ME (2001) Handbook of Religion and Mental Health. San Diego: Academic.
- Miller WR, Thoresen CE (2003) Spirituality, religion & health: An emerging research field. Am Psychol 58: 24-35.
- Zinnbauer BJ, Pargament K, Scott AB (1999)The emerging meaningness of religiousness andspirituality: Problems and prospects. J Pers 67: 889-919.
- Dhar N, Chaturvedi SK, Nandan D (2013) Spiritual health, the fourth dimension: a public health perspective. WHO South-East. Asia J Public Health 2:3-5.
- Eagan R (2010) Health promotion and spirituality: Making the implicit explicit. Health Promotion Forum 34: 1-4.
- Chatters LM (2000) Religion and health: Public health research and practice. Annu Rev of Public Health 21: 335-367.
- Giger J N, Appel SJ, Davidhizar R, Davis C (2008) Church and spirituality in the lives of the African American community. J TranscultNurs19: 375-383.
- Musgrave C, Allen C, Allen G (2002) Spirituality and health for women of color. Am J of Public Health92: 557-561.
- Koenig HG (2004) Spirituality, wellness and quality of life. Sex Reprod Menopause2: 76-82.
- Lincoln E (1974)The black church since Frazier. Schocken Books, New York.
- Millon Underwood S, Powell RL (2006) Religion and spirituality: Influence on health/risk behavior and cancer screening behavior of African Americans. ABNF J 17: 20-31.
- Ellison CW, Smith J (1991)Toward an integrative measure of health and well-being. JPsycholTheol 19: 35-48.
- Kreuter M, Lukwago SW, Bucholtz DC, Clark EM, Sanders Thompson V (2003) Achieving cultural appropriateness in health promotions programs: Targeted and tailored approaches. Health EducBehav30: 133-146.
- Kreuter M, McClure S (2004)The role of culture in health communication. Annu Rev of Public Health 25: 439-455.
- Yanek LR, Becker DM, Moy TF, Gittlelsohn J, Koffman DM (2001) Project Joy: Faith based cardiovascular health promotion for African American women. Public Health Reports,pp: 69-81.
- Holt (2003) Development of a Spiritually Based Breast Cancer Educational Booklet for African American women. Cancer Control 10: 37-43.
- Hoffman-Goetz L (1999) Cancer experiences of African American women as portrayed in popular mass magazines. Psychooncology 8: 36-45.
- Godbold Kean L, Prividera LC, Boyce A, Curry T (2012) Media use, media literacy, and African American females’ food consumption patterns. Howard Journal of Communication 23: 197-214.
- Frisby C (2002) Messages of hope: Health communication strategies that address barriers preventing Black women from screening for breast cancer. J Black Studies 32: 489-505.
- Lumpkins C, Bae J, Cameron G (2009) Generating Conflict for Greater Good: Contingency Theory as a Strategic Tool to Impact Health Disparities in African American Communities, Public Relations Review 36: 73-77.
- Lumpkins CY, Cameron GT, Frisby C (2012) Spreading the gospel of good health: Assessing ethnic and mass women’s magazines as communication vehicles to combat health disparities among African Americans. J Media and Religion 11: 78-90.
- Dailey DE, Steart AL (2007) Psychometric characteristics of the spiritual perspective scale in pregnant African-American women. Research in Nursing & Health30: 61-71.
- Dessio W, Wade C, Chao M, Kronenberg F, Cushman L, et al. (2004) spirituality and healthcare choices of African American women: Results of a national survey. Ethn Dis 14: 189-197.
- LumpkinsCY (2010) Sacred symbols as a peripheral cue in health advertisements: an assessment of using religion to appeal to African American women about breast cancer screening. J Media and Religion 9:181-201.
- Paloutzian RF, Ellison CW (1982) Loneliness, spiritual well-being and the quality of life. In Peplau LA, Perlman D (eds.), Loneliness: A sourcebook of current theory, research and therapy, John Wiley & Sons,New York, pp: 224-236.
- Ellison CW (1983) Spiritual well-being: Conceptualization and measurement. J PsycholTheol11: 330-340.
- Fernander A, Wilson J, Stanton M, Leukefeld C (2004) An exploratory examination of the Spiritual Well Being Scale among incarcerated black and white male drug users. International journal of Offender Therapy and Comparative Criminology 48: 403-413.
- Genia V (2001) Evaluation of the Spiritual Well-Being Scale in a sample of college students. International Journal for the Psychology of Religion 11: 25-33.
- Champion VL, Scott CR (1997) Reliability and validity of breast cancer screening belief scales in African American women. Nursing Research 46:331-337.
- Cheung GW, Rensvold RB (2002) Evaluating goodness-of-fit indexes for testing measurement invariance. Structural Equation Modeling 9: 233-255.
- Little TD, Gunningham WA, Sbahar G, Widaman KE (2002) To parcel or not to parcel: Exploring the question, weighing the merits. Structural Equation Modeling 9: 151-173.
- Brown TA (2006) Confirmatory factor analysis for applied research. Guilford Press, New York.
- Little TD, Card NA, Bovaird JA, Preacher KJ, Crandall CS (2007) Structural equation modeling of mediation and moderation with contextual factors. In:Little TD, Bovaird JA, Card NA (eds.), Modeling contextual effects in longitudinal Mahwah, NJ: Lawrence Erlbaum Associates, pp: 207-230.
- Bentler PM (1990) Comparative fit indexes in structural models. Psychol Bulletin107: 238-246.
- Tucker LR, Lewis CA (1973) Reliability coefficient for maximum likelihood factor analysis. Psychometric 38: 1-10.
- Steiger JH, Lind LC (1980)Statistically based tests for the number of factors. Paper presented at the annual spring meeting of the Psychometric Society, Iowa City, IA.
- Muthén L, Muthén B (2007) M Plus user’s guide: Statistical Analysis With Latent Variables.Los Angeles, CA
- Hu LT, Bentler PM (1999) Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal 6: 1-55.
- Steiger JH (2007) Understanding the limitations of global fit assessment in structural equation modeling. Personality and Individual Differences 42: 893-898.
- MacCallumRC, Browne MW, Cai L (2006) Testing differences between nested covariance structure models: Power analysis and null hypotheses. Psychol Methods 11: 19-35.
- Muthén LK, Muthén BO (1998-2012)Mplus user’s guide.
- Enders CK (2010) Applied missing data analysis. The Guildford Press, New York.
- Rubin DB (1987) Multiple imputations in nonresponse in survey. Wiley & Sons, New York.
- Mattis J (2002) African American women’s definitions of spirituality and religiosity. J Black Psychol 26: 101-122.
- Utsey S, Lee A, Bolden MA, Lanier YA (2005) Confirmatory test of the factor validity of scores on the spiritual well-being scale in a community sample of African Americans. J PsycholTheol33: 251-257.
- Jegers R, Smith P (1996) Further Examination of the spirituality scale. J Black Psychol22: 429-442.
- Miller G, Fleming W, Brown-Anderson F (1998) Spiritual well-being scale ethnic differences between Caucasians and African-Americans. J Psychol and Theol126: 358-364.
- Greg G (2011) I’m a Jesus girl: Coping stories of Black American women diagnosed with breast cancer. J Religion and Health 50: 1040-1053.
- Best AL, Spencer SM, Hall I, Friedman D, Billings D (2015) Developing spiritually framed breast cancer screening messages in consultation with African American women. Health Communication 30: 290-300.
- Kline KN (2007) Cultural sensitivity and health promotion: Assessing breast cancer education pamphlets designed for African American women. Health Communication21:85-96.

