Keywords
Atrial fibrillation; Left atrial or left atrial appendage thrombus; Transesophageal echocardiography; CHADS2 score; CHA2DS2VASC score
Introduction
Atrial fibrillation (AF) is the most common cardiac arrhythmia with a growing prevalence due to an aging population. One of the major issues for AF is stroke and systemic embolism in patients at high risk that are associated with significant morbidity and mortality as well as social and financial burdens [1]. Stroke and other thromboembolic events are closely related to left atrial (LA) or left atrial appendage (LAA) thrombus. Transesophageal echocardiography (TEE) is considered the gold standard for detecting LA/LAA thrombus, with 97% sensitivity and 100% specificity [2,3]. Expert consensus recommends routine anticoagulation and exclusion of LA/LAA thrombus using TEE prior to AF ablation or cardio version [4]. However, TEE is an invasive and expensive procedure that is associated with discomfort to the patients and potential serious complications like esophageal injuries, and may lead to decreased level of willingness to follow the recommendations [5,6]. Clinically, LA/LAA thrombus has been identified only in a small portion of the AF patients with TEE. However, it is critical to rule out LA/LAA thrombus prior to AF ablation or cardio version to minimize the risk of stroke and other thromboembolic events. Therefore, there is a need to establish a system to predict the risk of LA/LAA thrombus in AF patients.
Currently, the risk for stroke for non-valvular AF patients has been determined with a scoring system (CHADS2 or CHA2DS2- VASc) based on the number of risk factors like age, sex, hypertension , diabetes, cardiac function, and previous stroke. These two scoring systems have been widely used clinically to guide the selection of AF patients for systematic anticoagulation therapy for stroke prevention [7,8]. The clinical data have shown that CHA2DS2VASC is as good as, and possibly better than CHADS2 in identifying patients at risk for stroke and other thromboembolism [9,10]. The clinical value of these scoring systems especially based on the recently recommended CHA2DS2VASC score in the AHA/ACC/HRS guidelines to evaluate the risk of thromboembolism in AF patients has been validated in multiple clinical studies [11]. However, there are little data on CHA2DS2VASC and CHADS2 scores to predict LA/LAA thrombus prior to AF ablation or cardio version. In the present study, we demonstrated that CHADS2 or CHA2DS2VASC scores could be used to predict the risk for LA/LAA thrombus in AF patients with or without adequate systematic anticoagulation therapy, and to identify the high risk patients who could really benefit from TEE prior to AF ablation or cardio version.
Methods
Patient population
The study protocol was reviewed and approved by the ethic committee of Chong-qing Medical University. An informed consent was obtained from every patient in the study. All the patients (both male and female with age 18 and above) with drug-refractory symptomatic non-valvular AF (including paroxysmal, persistent, and chronic AF) who were scheduled for AF ablation at the First and Second Affiliated Hospitals of Chongqing Medical University between January 2010 to June 2012 were included in the study. The AF patients who underwent repeat AF ablation were excluded. Diagnosis of AF in all patients was confirmed with a 12-lead surface ECG or Holter monitoring. Paroxysmal AF was defined as self-terminating episodes of AF lasting for less than 7 days. Persistent AF was defined as AF sustained for more than 7 days, and requiring electrical or pharmacological cardio version [11]. Clinical risk factors including age, sex, types of AF, hypertension, diabetes mellitus, stroke or TIA, vascular disease, cardiac function, and other clinical data were collected from all the patients.
Anticoagulation
Based on the level of anticoagulation therapy, patients were divided into two groups for further analysis: with and without adequate anticoagulation. The patients were classified into the group of adequate anticoagulation therapy if they were in coumadin with INR 2.0 or above for at least 4 weeks or aspirin following the expert consensus strictly [4].Otherwise, the patients were considered to be of without adequate anticoagulation, although all the patients were advised to be treated with anticoagulation therapy recommended by expert consensus. In brief, patients with two or more risk factors were strongly encouraged to take coumadin for at least 4 weeks prior to the ablation procedure. Patients with one risk factor were recommended to receive coumadin or aspirin. Patients without risk factors would stay on aspirin. Patients on coumadin were asked to have an INR check every week for 4 weeks to maintain their INR of 2.0-3.0 prior to ablation. Patients with LA/LAA thrombus identified with TEE were advised to receive anticoagulation treatment for at least 4 weeks before undergoing another TEE. After LA/LAA thrombus was excluded using TEE, the patients underwent AF ablation. All patients were placed on an adequate systemic anticoagulation therapy as recommended by expert consensus during and after ablation [4].
LA/LAA thrombus risk assessment
The CHADS2 [cardiac failure, hypertension, age, diabetes, and stroke (doubled)] scoring system was adopted from the AF Investigators and Stroke Prevention in Atrial Fibrillation (SPAF): 2 points for a history of stroke or TIA, and 1 point each for age >75 years, a history of hypertension, diabetes, or cardiac failure. Similar to atrial fibrillation, the patients with a CHADS2 score of 0, 1, and 2 or above were considered at low, intermediate, and high risk for LA/LAA thrombus, respectively [12]. CHA2DS2VASC score was also calculated prior to TEE for each patient: 2 points for a history of stroke or TIA, or age ≥ 75, and 1 point each for age 65–74 years, a history of hypertension, diabetes, heart failure, vascular disease [(myocardial infarction, complex aortic plaque, and peripheral vascular disease (PAD) including prior revascularization, amputation due to PAD, or angiographic evidence of PAD)] and female sex. Based on the score, the patients were divided into low (CHA2DS2VASC score of 0), intermediate (score of 1), and high risk group (score ≥ 2) [12]. Other risk factors including enlarged LA (LA ≥ 40mm), type of AF (persistent or chronic), and AF at the time of TEE were also taken into consideration in the present study [1].
Transesophageal echocardiography
After obtaining a written informed consent, TEE was performed within 24 hours prior to ablation. At first, the heart chamber size and left ventricular ejection fraction were assessed with transthoracic echocardiography (TTE). Then, the presence of potential LA/LAA thrombus was carefully evaluated with TEE using a 6-MHz multiplane probe of the GEViVid7.0 color doppler ultrasonic diagnostic apparatus. All patients were examined with the use of 10% lidocaine gel for posterior pharyngeal anesthesia after fasting for at least six hours. No sedation or atropine was administered. The TEE probe was inserted with the subject lying on the left lateral position. Cine loops of the LAA were acquired during a continuous sweep from 0° to 180°. A thrombus was defined as an echo-dense mass with a uniform texture different from that of the LA/LAA endocardial wall [13,14]. All TEEs were performed and interpreted by experienced cardiologists without knowledge on the patients’ risk scores.
Follow-up assessment for stroke during the ablation and 7 days after the procedure
In addition to regular monitoring, additional efforts were made to evaluate all the patients to determine if the patients developed any new abnormal neurological symptoms and signs over their baseline during the procedure and 7 days after the procedure. Brain CT or MRI examinations were performed to establish the diagnosis if clinically indicated.
Statistical analysis
The data with continuous variables were expressed as mean ± standard deviation and categorical variables as frequencies and percentages. Statistical analyses were performed using the SPSS software (version 17.0 Chicago: SPSS Inc.). Unpaired student ttest (two-sided) was used for two group comparison for continuous variables. The categorical variables were analyzed using chi-square or Fisher’s exact test. Multivariate logistic regression analysis was performed on variables found to be significant by univariate analysis. ROC curve analysis was performed to determine the sensitivity and specificity of the two risk stratification systems (CHADS2 and CHA2DS2VASC scores) predicting the LA/LAA thrombus. All statistical tests were twosided, and a p value of <0.05 was considered statistically significant.
Results
Patients’ characteristics
A total of 397 patients were enrolled in the present study during the 2.5 years period. The baseline characteristics of patients were shown in Table 1. Over 80% of the patients had paroxysmal AF, and the most common associated medical condition was hypertension (38.5%). The majority of the patients were at low or intermediate risk as defined by either CHADS2 score or CHADS2VAC scores.
| Number |
397 |
|
|
| Age (years) |
59 ± 13 |
Chads2=0 |
206 (51.9%) |
| Male gender |
263 (66%) |
Chads2=1 |
135 (34%) |
| LA size (mm) |
35 ± 8 |
Chads2 ≥ 2 |
56 (14.1%) |
| LVEF (%) |
60 ± 7 |
CHA2DS2VASC= 0 |
112 (28.2%) |
| AF at the time of TEE |
123 (31%) |
CHA2DS2VASC= 1 |
121 (30.5%) |
| AF history (months) |
16 ± 6 |
CHA2DS2VASC ≥ 2 |
164 (41.3%) |
| Paroxysmal AF |
325 (82%) |
Coumadin therapy |
158 (39.8%) |
| Hypertension |
153 (38.5%) |
INR of 2.0-3.0 |
144 (36.3%) |
| Diabetes mellitus |
40 (10%) |
LA/LAA thrombus |
38 (9.6%) |
| CAD |
55 (13.9%) |
PVI |
330 (83%) |
| Previous stroke or TIA |
13 (3.3%) |
PVI+line ablation |
67 (17%) |
| PVD |
8 (2%? |
|
|
| Aspirin therapy |
81 (20%) |
|
|
AF=Atrial fibrillation; CAD=Coronary artery disease; INR=International normalized ratio; LA/LAA= Left atrial or left atrial appendage; LVEF=Left ventricular ejection fraction; PVD=Peripheral vascular diseases; PVI=Pulmonary vein isolation; TIA=Transitory ischemic attack.
Table 1: Patient characteristics.
To determine if adequate anticoagulation therapy could affect the predictive value of CHADS2 and CHA2DS2VASC scores for LA/LAA thrombus, the patients were divided into two groups: 1) patients without adequate anticoagulation (202 patients), and 2) patients with adequate anticoagulation with coumadin or aspirin (195 patients). The patients’ characteristics were summarized in Table 2. Between the two groups, age, gender, AF at the time of TEE, type of AF, hypertension, diabetes mellitus, coronary artery disease, previous stroke or TIA, were not significantly different. In both groups, there were no significant differences between the low, intermediate and high risk patients classified by CHADS2 and CHADS2VAC scores.
| Variables |
Without OAC |
With adequate OAC |
P-Value |
| Number |
202 |
195 |
0.472 |
| Age (years) |
60.09 ± 11.07 |
58.71 ± 12.821 |
0.435 |
| Male gender |
147 (73%) |
126 (65%) |
0.817 |
| LA ≥ 40mm |
36 (18%) |
32 (16%) |
0.14 |
| LVEF<50% |
18 (9%) |
21 (11%) |
0.339 |
| AF at the time of TEE |
66 (33%) |
57 (29%) |
0.945 |
| Paroxysmal AF |
175 (87%) |
150 (77%) |
0.705 |
| Hypertension |
78 (39%) |
75 (38%) |
0.444 |
| Diabetes mellitus |
22 (11%) |
18 (9%) |
0.831 |
| CAD |
25 (12%) |
30 (15%) |
0.203 |
| Previous stroke or TIA |
6 (3%) |
7 (3.6%) |
0.594 |
| PVD |
4?2%? |
4?2.1%? |
0.804 |
| Chads2=0 |
104 (51%) |
102 (52%) |
0.476 |
| Chads2=1 |
67 (33%) |
68 (35%) |
0.865 |
| Chads2 ≥ 2 |
31 (16%) |
25 (13%) |
0.925 |
| CHA2DS2VASC=0 |
57 (28%) |
55 (28%) |
0.377 |
| CHA2DS2VASC=1 |
61 (30%) |
60 (31%) |
0.44 |
| CHA2DS2VASC ≥ 2 |
84 (42%) |
80 (41%) |
0.678 |
| Aspirin therapy |
14 (6.9%) |
67 (34.4%) |
<0.001 |
| Coumadin therapy |
33 (16.3%) |
125 (63.5%) |
<0.001 |
| INR of 2.0-3.0 |
23 (11.4%) |
121 (62.1%) |
<0.001 |
| LA/LAA thrombus |
29 (14.4%) |
9 (4.6%) |
0.002 |
AF=Atrial fibrillation; CAD=Coronary artery disease; INR=International normalized ratio; LA/LAA=Left atrial or left atrial appendage; LVEF=Left ventricular ejection fraction; OAC=Oral anticoagulation (coumadin or aspirin); PVD=Peripheral vascular diseases; TIA=Transitory ischemic attack; TEE=Transesophageal echocardiography.
Table 2: Clinical characteristics for the patients in the two groups.
The incidence of LA/LAA thrombus and thromboembolism
As shown in (Table 1), a significant number of patients (9.6%) with AF were found to have LA/LAA thrombus on TEE. As expected, the incidence of LA/LAA thrombus was significantly higher in the patients without adequate anticoagulation (14.4%) than that in the patients with adequate anticoagulation therapy (4.6%) (p=0.002) (Table 2). No thrombus was found in patients in both groups during the procedure and 7 days after AF ablation.
CHADS2 and CHADS2VAC scores were associated with LA/LAA thrombus
We then evaluate the relationship between CHADS2 and CHA2DS2VASC scores and LA/LAA thrombus in AF patients. In both groups, a significant portion of patients who were classified as low and intermediate risks using CHADS2 score fell into the group of high risk individuals when CHADS2VAC score system was used (Figure 1). As expected, the higher CHADS2 and CHA2DS2VASC scores, the higher prevalence for LA/LAA thrombus in AF patients in the two groups as shown in Figure 2.
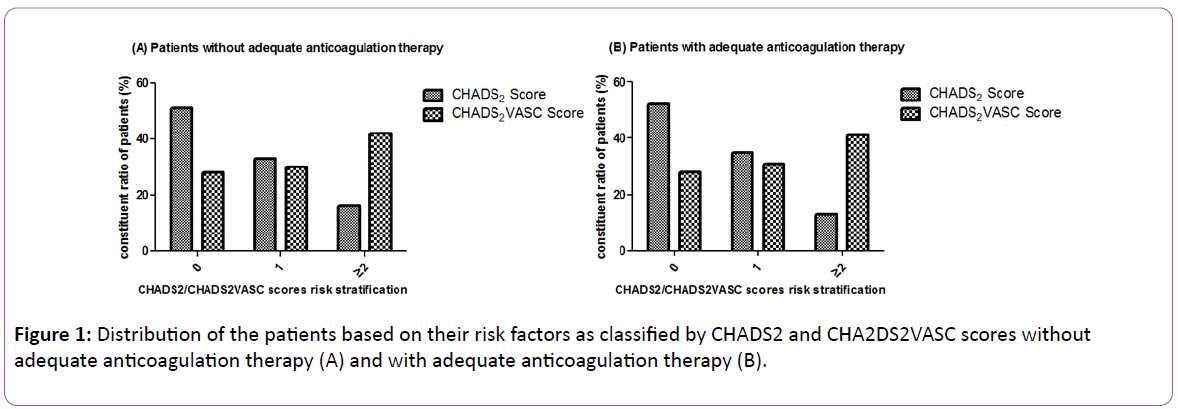
Figure 1: Distribution of the patients based on their risk factors as classified by CHADS2 and CHA2DS2VASC scores without adequate anticoagulation therapy (A) and with adequate anticoagulation therapy (B).
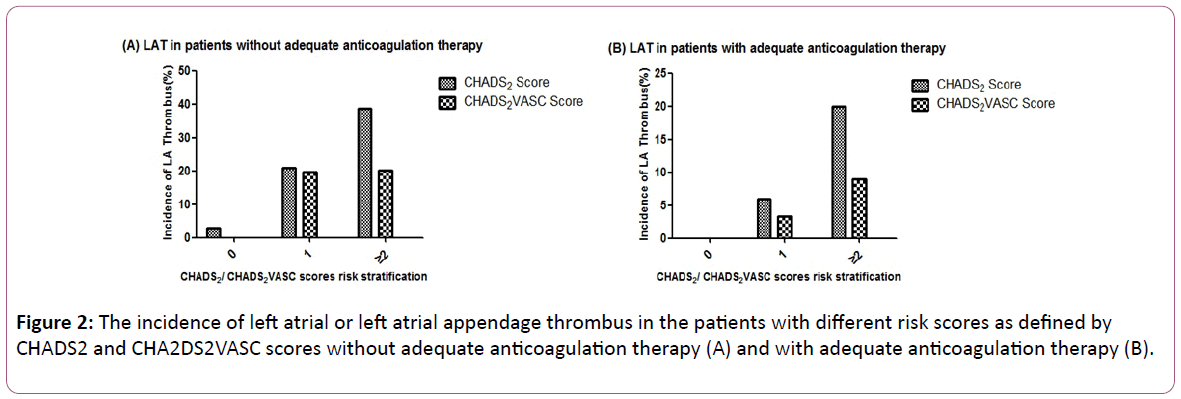
Figure 2: The incidence of left atrial or left atrial appendage thrombus in the patients with different risk scores as defined by CHADS2 and CHA2DS2VASC scores without adequate anticoagulation therapy (A) and with adequate anticoagulation therapy (B).
Although 9.6% of all AF patients had LA/LAA thrombus, no LA/LAA thrombus was identified in patients with CHA2DS2VASC score of 0 regardless the status on their anticoagulation (with or without adequate anticoagulation treatment).
However, LA/LAA thrombus was detected in a small number of patients (2.9%) with CHADS2 score of 0 who were not adequately treated with anticoagulation therapy, while no LA/LAA thrombus was observed in those with CHADS2 score of 0 with adequate anticoagulation therapy (Figure 2).
Univariate analysis showed that heart failure (LVEF50%), diabetes mellitus, previous stroke or TIA, hypertension, inadequate coumadin or aspirin therapy, CHADS2 score of ≥ 2 and CHA2DS2VASC score of ≥ 2 were significantly associated with LA/LAA thrombus (Table 3).
| Variables |
No LA/LAAT N=359 (%) |
LA/LAAT
N=38 (%) |
Odds Ratio (95% CI) |
P Value |
| Hypertension |
122 (34%) |
31 (81.6%) |
1.187 (1.090 -1.293) |
<0.001 |
| Diabetes mellitus |
26 (7.2%) |
14 (36.8%) |
1.409 (1.120-1.773) |
<0.001 |
| No OAC therapy |
127 (35.4%) |
31 (81.6%) |
1.175 (1.054-1.309) |
=0.002 |
| Stroke or TIA |
7 (1.95%) |
6 (15.8%) |
1.673 (1.011-2.771) |
<0.001 |
| CAD |
44 (12.3%) |
11 (28.9%) |
1.129 (0.985-1.294) |
=0.656 |
| LA ≥ 40 mm |
53 (14.8%) |
15 (39.5%) |
1.018 (0.943-1.100) |
=0.784 |
| LVEF<50% |
13 (3.6%) |
26 (68.4%) |
1.173 (1.099-1.252) |
<0.001 |
| Chads2 ≥ 2 |
33 (9.2%) |
23 (60.5%) |
1.700 (1.319-2.192) |
<0.001 |
| CHA2DS2VASC ≥ 2 |
129 (35.9%) |
35 (92.1%) |
1.316 (1.203-1.440) |
<0.001 |
CAD=Coronary artery disease; CI=Confidence interval; LA= Left atrium; LA/LAAT=Left atrial or left atrial appendage thrombus; LVEF=Left ventricular ejection fraction; OAC=Oral anticoagulation (coumadin or aspirin);TIA=Transitory ischemic attack
Table 3: Prevalence of risk factors in patients with and without LA/LAAT.
Multivariable logistic regression analysis demonstrated that CHA2DS2VASC score of ≥ 2 (p=0.02), CHADS2 score of ≥ 2 (p=0.046) and previous stroke or TIA (p=0.038) were the factors independently associated with LA/LAA thrombus in the patients regardless of their anticoagulation status (Table 4).
| Variables |
Odds Ratio (95% CI) |
P-Value |
| Hypertension |
1.693 (0.662-4.329) |
0.272 |
| Diabetes mellitus |
1.001 (0.945-1.060) |
0.676 |
| No OAC therapy |
1.805 (0.426-7.638) |
0.423 |
| Previous stroke or TIA |
3.507 (1.104-6.476) |
0.038 |
| LVEF<50% |
2.026 (0.782-5.251) |
0.146 |
| Chads2 ≥ 2 |
2.389 (1.09-4.792) |
0.046 |
| CHA2DS2VASC ≥ 2 |
5.964 (1.627-8.970) |
0.02 |
CAD=Coronary artery disease; CI=Confidence interval; LA=Left atrium; LA/LAA=Left atrial or left atrial appendage; LVEF=Left ventricular ejection fraction; OAC=Oral anticoagulation (coumadin or aspirin);TIA=Transitory ischemic attack
Table 4: Multivariate analysis of clinical variables on predicting LA/LAA Thrombus.
Using ROC curve analysis for the patients with or without adequate anticoagulation, we found that a CHADS2 score and CHA2DS2VASC score could be used to predict the presence of LA thrombus compared with reference. The areas under the curve (AUC) of CHADS2 score and CHA2DS2VASC score were 0.681 (SE=0.028, 95% CI: [0.623, 0.737]) and 0.691 (SE=0.031, 95% CI: [0.630, 0.752]) respectively. CHA2DS2VASC score was only slightly better than CHADS2 score, but there was no significant difference (Figure 3).
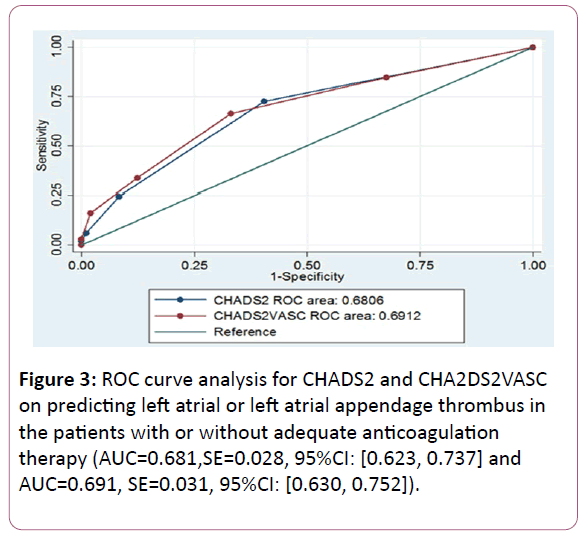
Figure 3: ROC curve analysis for CHADS2 and CHA2DS2VASC on predicting left atrial or left atrial appendage thrombus in the patients with or without adequate anticoagulation therapy (AUC=0.681,SE=0.028, 95%CI: [0.623, 0.737] and AUC=0.691, SE=0.031, 95%CI: [0.630, 0.752]).
Discussion
Study main findings
In the present study, we found that LA/LAA thrombus was present in 9.6% of all the AF patients regardless of their anticoagulation status. Adequate anticoagulation significantly reduced the prevalence of LA/LAA thrombus in AF patients (from 14.4% to 4.6%).No thrombus was identified in patients with CHA2DS2VASC score of 0 regardless of their status on anticoagulation therapy. However, LA/LAA thrombus was present in some patients (2.9%) with CHADS2 score of 0 who were not adequately treated with anticoagulation. Compared to the CHADS2 score, CHA2DS2VASC score could not be more valuable to predict LA/LAA thrombus in the patients regardless of their anticoagulation status.
Adequate anticoagulation therapy reduces the incidence of LA/LAA thrombus
The data from the present study confirmed that adequate anti-coagulation therapy significantly reduced the incidence of LA/LAA thrombus as expected. A wide range of LA/LAA thrombus prevalence (from 0.5% up to 13.8%) in patients with AF has been reported [15,16]. Previous studies showed that the incidence of LA/LAA thrombus identified by TEE was estimated to be about 2% despite adequate anticoagulation [17,18]. The incidence for LA/LAA thrombus in AF patients in our study was significantly higher than that reported. The reasons for the big difference in LA/LAA thrombus prevalence were unclear at this point. However, it might be due to the differences in the risk factors in the study patient populations, and different ethnic background. Indeed, it was reported that the incidence of stroke in Chinese population was significantly higher than those in western countries [19]. It is well known that AF is strongly associated with stroke. Further studies are needed to determine the role of ethnic background in the development of LA/LAA thrombus in AF patients.
The value of CHADS2 score and CHA2DS2VASC score on predicting LA/LAA thrombus
There are several methods to assess the risk for stroke and thrombo-embolism in non-valular AF patients [7]. Currently, the widely used and validated methods for risk stratification for stroke were CHADS2 score and CHA2DS2-VASC score. Clinical data have shown that CHA2DS2VASC score is more accurate for screening the low risk patients for future stroke events than CHADS2 score [10]. Strokes in AF patients are associated with hypercoagulability, LA enlargement, atrial endothelial dysfunction and fibrosis and other risk factors. It is believed that about 75% of the sources for stroke in AF patients are originated from the LA/LAA thrombus [20]. Therefore, it could be beneficial and important to predict the LA/LAA thrombus using the CHADS2 and CHA2DS2VASC scores.
In the present study, we observed that higher CHADS2 and CHA2DS2VASC scores were associated with increased prevalence of LA/LAA thrombus in the patients with and without adequate anticoagulation, indicating that CHADS2 score and CHA2DS2VASC score are both associated with LA/LAA thrombus in patients regardless of their anticoagulation status. The multivariate logistic regression analysis showed that previous stroke or TIA, CHA2DS2VASC score of ≥ 2 and CHADS2 score of ≥ 2 were the independent factors predicting the presence of LA/LAA thrombus. In a previous study, hypertension, age >75, and cardiomyopathy were found to be independently associated with LA/LAA thrombus by TEE in 635 patients treated with coumadin for at least 4 weeks prior to AF ablation [2]. Other clinical factors including diabetes, valve disease, and prior stroke or TIA, did not predict LA/LAA thrombus. Recently, it was shown that diabetes mellitus, CHADS2 score ≥ 3 and CHA2DS2VASC score ≥ 4 were independent predictor for LA/LAA thrombus [18]. Under similar clinical circumstance, Jeffrey and colleagues demonstrated a strong association between CHADS2 score and LA/LAA thrombus. Among the risk factors for CHADS2 score, CHF was identified as the only independent risk factor correlated with LA/LAA thrombus [21]. Clearly, there were significant differences in the outcomes from different studies. The discrepancy in the study results was likely due to the differences of the enrolled patient populations in each study. Our present study showed that diabetes or heart failure were not independent predictors for LA/LAA thrombus , which maybe the majority of patients were low and intermediate risk individuals.
Although the CHADS2 score was developed to identify AF patients at high risk for stroke, the goal of the CHA2DS2VASc score was to identify the truly low-risk patients who might not require oral anticoagulation therapy [22]. Indeed, no LA/LAA thrombus was identified in patients with a CHA2DS2VASC score of 0 regardless of their systemic anticoagulation therapy, whereas there was LA/LAA thrombus in some patients with a CHADS2 score of 0 without adequate therapy. Of note, many patients with low and intermediate risk based on CHADS2 scoring system could be re-classified into high risk categories using the CHA2DS2VASC score system. Our data suggested that although CHA2DS2VASC scores were not more valuable to predict LA/LAA thrombus than CHADS2 scores, CHA2DS2VASc score was better to identify the truly low-risk patients with LA/LAA thrombus than CHADS2 score.
Clinical implication
LA thrombus is a major source for stroke in AF patients, and a contraindication for AF ablation or cardio version. To avoid stroke related to LA/LAA thrombus, the expert consensus recommended an adequate anticoagulation therapy and TEE prior to AF ablation or cardio version [1]. With the increasing prevalence of AF, healthcare expenditures related to LA/LAA thrombus identification, anticoagulation therapy and associated potential bleeding complications could be certainly increased. Clinical studies showed the absolute risk for major bleeding in AF patients on coumadin was about 2% per year, with approximately one quarter of the bleeding complications involving intracranial hemorrhages [23]. On the other hand, oral anticoagulation therapy presents a major challenge to both physicians and patients with many patients either over-treated or under-treated as reported in clinical studies [24]. Compared with western countries, underuse of coumadin is more common in China due to decreased tolerance to coumadin and increased tendency of bleeding. Therefore, it is very useful to create a reliable method to identify the patients with high risk of LA/LAA thrombus for optimal anticoagulation therapy for the right patient populations.
There is wide variation among the Task Force Members on the use of TEE prior to AF ablation or cardio version. Approximately 50% of Task Force Members could perform a TEE in all patients undergoing AF ablation regardless of their presenting rhythm and CHADS2 or CHA2DS2VASc score, while the others could not agree with the recommendation [4]. The data from the present study suggested that it might be not mandatory for the patients with low risk identified by CHA2DS2VASC scores to perform a routine TEE and/or start anticoagulation therapy prior to AF procedure or cardio version, and it could be necessary for high risk patients classified by CHA2DS2VASC or CHADS2 scores. Our follow-up data showed no patient with a CHA2DS2VASC score of 0 had a stroke during and after ablation no matter with or without adequate anticoagulation therapy, indicating that it could be safe for low risk patients without anticoagulation therapy to undergo AF ablation or cardio version without TEE.
Study limitations
In the present study, LA/LAA thrombus was identified by experienced cardiologists. However, the study was not a randomized trial. The majority of the patients were young low risk patients with paroxysmal AF. Therefore, patient selection bias might be present.
Conclusion
The present study showed that both CHA2DS2VASC and CHADS2 scores were associated with LA/LAA thrombus on TEE in non-valvular AF patients. Although CHA2DS2VASC score did not appear to be more valuable to predict the presence of LA/LAA thrombus in the patients without adequate anticoagulation than CHADS2 score, CHA2DS2VASc score seemed better to identify the truly low-risk patients with LA/LAA thrombus than CHADS2 score. It seemed safe to perform AF ablation or cardio version in AF patients with a CHA2DS2VASC of 0 without TEE or anticoagulation therapy.
Acknowledgement
None
Conflict of Interest
None
References
- Camm AJ, Kirchhof P, Lip GY, et al. (2010) European Heart Rhythm Association; European Association for Cardio-Thoracic Surgery, Guidelines for the management of atrial fibrillation: the Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC). Eur Heart J 31: 2369-2429.
- McCready JW, Nunn L, Lambiase PD, Ahsan SY, Segal OR, et al. (2010) Incidence of left atrial thrombus prior to atrial fibrillation ablation: is pre-procedural transoesophageal echocardiography mandatory? Europace 12: 927-932.
- Koca V, Bozat T, Akkaya V, Sarikamis C, Turk T, et al. (1999) Left atrial thrombus detection with multiplane transesophageal echocardiography: an echocardiographic study with surgical verification. J Heart Valve Dis 8: 63-66.
- Calkins H, Kuck KH, Cappato R, Brugada J, Camm AJ, et al. (2012) 2012 HRS/EHRA/ECAS Expert Consensus Statement on Catheter and Surgical Ablation of Atrial Fibrillation: recommendations for patient selection, procedural techniques, patient management and follow-up, definitions, endpoints, and research trial design. Europace 14: 528-606.
- Arbelo E, Brugada J, Hindricks G, Maggioni A, Tavazzi L, et al. (2012) Esc-Eurobservational research programme:the atrial fibrillation ablation pilot study,conducted by the European heart rhythm association. Europace 14: 1094-1104.
- Bhargava M, Di Biase L, Mohanty P, Prasad S, Martin DO, et al. (2009) Impact of type of atrial fibrillation and repeat catheter ablation on long-term freedom from atrial fibrillation: results from a multicenter study. Heart Rhythm 6: 1403-1412.
- Fang MC, Go AS, Chang Y, Borowsky L, Pomernacki NK, et al. (2008) Comparison of risk stratification schemes to predict thromboembolism in people with nonvalvular atrial fibrillation, J Am Coll Cardiol 51: 810-815.
- Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, et al. (2001) Validation of clinical classification schemes for predicting stroke: results from the National Registry of Atrial Fibrillation. JAMA 285: 2864-2870.
- Uehara M, Funabashi N, Takaoka H, Ozawa K, Kushida S, et al. (2014) CHA2DS2-VASc score is a useful-predictor of not prognosis but coronary-arteriosclerosis in chronic atrial-fibrillation compared with CHADS2 score: A two-center study of 320-slice CT, part 2. Int J Cardiol (2014)177: 368-373.
- Pieri A, Lopes TO, Gabbai AA (2011) Stratification with CHA2DS2-VASc score is better than CHADS2 score in reducing ischemic stroke risk in patients with atrial fibrillation. Int J Stroke 6: 466.
- January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, et al. (2014) 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. Circulation 130: 1524-4539.
- Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ (2010) Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation. Chest 137: 263-272.
- Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, et al. (2005) Recommendations for chamber quantification: a report from the American Society of Echocardiography's Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr 18: 1440-1463.
- Schneider B, Stöllberger C, Schneider B (2007) Diagnosis of left atrial appendage thrombi by multiplane transesophageal echocardiography: interlaboratory comparative study Circ J 71: 122-125.
- Thambidorai SK, Murray RD, Parakh K, Shah TK, Black IW, et al. (2005) Utility of transesophageal echocardiography in identification of thrombogenic milieu in patients with atrial fibrillation (an ACUTE ancillary study). Am J Cardiol 96: 935-941.
- Khan MN, Usmani A, Noor S, Elayi S, Ching CK, et al. (2008) Low incidence of left atrial or left atrial appendage thrombus in patients with paroxysmal atrial fibrillation and normal EF who present for pulmonary vein antrum isolation procedure. J Cardiovasc Electrophysiol 19: 356-358.
- Scherr D, Dalal D, Chilukuri K, Dong J, Spragg D, et al. (2009) Incidence and predictors of left atrial thrombus prior to catheter ablation of atrial fibrillation. J Cardiovasc Electrophysiol 20: 379-384.
- Dorenkamp M, Sohns C, Vollmann D, Lüthje L, Seegers J, et al. (2013) Detection of left atrial thrombus during routine diagnostic work-up prior to pulmonary vein isolation for atrialfibrillation: role of transesophageal echocardiography and multidetector computed tomography. Int J Cardiol 163: 26-33.
- Mukherjee D, Patil CG (2011) Epidemiology and the global burden of stroke. World Neurosurg 76: S85-S90.
- Lubitz SA, Rosen AB, Ellinor PT, Benjamin EJ (2010) Stroke risk in AF: do AF patterns matter? Eur Heart J 31: 908-910.
- Decker JM, Madder RD, Hickman L, Marinescu V, Marandici A, et al. (2011) CHADS2 score is predictive of left atrial thrombus on precardioversion transesophageal chocardiography in atrial fibrillation. Am J Cardiovasc Dis 1: 159-165.
- Mason PK, Lake DE, DiMarco JP, Ferguson JD, Mangrum JM, et al. (2012) Impact of the CHA2DS2-VASc Score on Anticoagulation Recommendations for Atrial Fibrillation. Am J Med 125: 603.e1-603.e6.
- Weir NU (2008) An Update on Cardioembolic Stroke.Postgrad Med J 84: 133-142.
- Zimetbaum PJ, Thosani A, Yu HT, Xiong Y, Lin J, et al. (2010) Are atrial fibrillation patients receiving warfarin in accordance with stroke risk? Am J Med 123: 446-453.