Joaquin Cagliani1, Garry Ritter1, Chris Nelson1, Denis Knobel1, Kristen Hopkins1, Ernesto P Molmenti2, Jeffrey Nicastro1, Gene Coppa1and Rafael Barrera1
1Department of Surgery, Long Island Jewish Medical Center, Northwell Health System, New Hyde Park, NY, 11040, USA
2Department of Surgery, North Shore University Hospital, Northwell Health System, Man-hasset, NY, 11030, USA
*Corresponding Author:
Joaquin Cagliani
MD, Department of Surgery and Critical Care Medicine
Northwell Health System, Manhasset, USA
. Tel: +17184707210
Fax:+17184707210
E-mail: jcagliani@northwell.edu
Received date: February 22, 2017; Accepted date: February 26, 2017; Published date: February 28, 2017
Citation: Cagliani J, Ritter G, Nelson C, et al. Bleeding Risk and Thromboprophylaxis in Neurosurgical Patients after Emergency Procedures. J Intensive & Crit Care 2017, 3:1.
Keywords
Low molecular weight heparin; Subcutaneous unfractionated heparin; Thromboprophylaxis; Anticoagulation; Dosing; Neurosurgery.
Introduction
Venous thromboembolism (VTE), including pulmonary embolism (PE) and deep venous thrombosis (DVT), is a well-described process that can cause significant morbidity and mortality. This is especially true in the patient population of a critical care unit [1]. The true incidence of thromboembolic disease in the critically-ill neurosurgical population admitted to a critical care setting has not been well described in the literature. In the absence of VTE thrombo-prophylaxis, the incidence of DVT has been observed between 10-40% in the general surgery population and as high as 40-60% in the major orthopedic surgery population [2].
In addition to VTE risk, mortality rates have also been stratified with VTE prophylaxis in mind, and institution of DVT prophylaxis results in decreased mortality risk [3-5]. Multiple case reports and series on postoperative thromboembolic prophylaxis have been published, however clear guidelines for a “Best Practice” have yet to be described [6-8]. Many investigators and even whole institutions have taken to stratifying the risk for developing VTE and treating the calculated risk accordingly. Treatment modalities range from encouraging early ambulation in the hospitalized patient to the use of compression stockings and/or therapeutic medical management [9].
Despite these ideas and methods, there is a hesitation and a paucity of data in its use the critically-ill neurosurgical population. The neurosurgery community has not developed a unified approach for the prevention of VTE thrombo-prophylaxis in this population [10]. While there is no doubt that stockings and ambulation are effective modalities, these are of-ten not feasible options for a critically-ill neurosurgical patient. The fear behind chemoprophylaxis is the risk of causing or worsening a cerebral or spinal hemorrhage, yet these fears must be balanced with the morbidity and mortality behind DVT propagation and subsequent embolic events related to immobility.
Our institution previously published a study examining the administration of subcutaneous unfractionated heparin (SCUFH) in 522 neurosurgery patients to determine the risk of post-operative hemorrhage [11]. We found no embolic events associated with the use of SCUFH, suggesting that there was no increased risk of bleeding in the general neurosurgical population. However, in the emergency neurosurgery setting, where patients are at high risk of developing VTE, the likelihood of receiving SCUFH or other forms of prophylaxis are significantly reduced compared to non-emergency cases [12] possibly related to the potential bleeding complications. This study is a retrospective analysis of prospectively-collected data evaluating the efficacy and safety of SCUFH in patients who underwent emergency neurosurgical procedures.
Methods
This is a retrospective review of prospectively-acquired data at a single institution at Long Island Jewish Medical Center. All patients in this study were admitted to the surgical intensive care unit and cared for by a dedicated surgical critical care team. We documented whether patients subcutaneous unfractionated heparin or not for venous thromboembolism (VTE) prophylaxis. Stratification of SCUFH was based upon the admitting and/or operating attending preference after discussion with the SICU attending. Of the patients receiving SCUFH, we delineated if patients received SCUFH within 24 h of surgery or greater than 24 h after surgery. All SCUFH patients received 5000 units of SCUFH every eight h until discharge, and no study patients were stopped prematurely or changed to low-molecular weight heparin (LMWH) products. All patients routinely received lower extremity compression boots; compliance was monitored by the nursing staff as per hospital policy. The patients were followed until date of discharge from SICU or death.
Inclusion criteria consisted of all neurosurgical and head trauma patients who required surgical intervention in the emergency setting. None of these patients had a history of heparin induced thrombocytopenia (HIT), PE or DVT. General patient characteristics were collected, including but not limited to: Age, gender, height, weight, body mass index and the amount of day under mechanical ventilation. Other factors taken into consideration included patient condition on admission to the intensive care unit; the ICU length of stay (LOS); units of blood transfused; ICU severity score including the Acute Physiology and Chronic Health Evaluation (APACHE) II score [13,14], APACHE III [13,15], Simplified Acute Physiology Score (SAPS) [16], Multiple Organ Dysfunction score (MODS) [17]; survival outcomes; and complications (heparin induced thrombocytopenia [HIT], deep vein thrombosis [18], and pulmonary embolism [PE], postoperative bleeding, and vasospasm). Postoperative bleeding, PE and vasospasm were evaluated clinically and/or with computed axial tomographic scan (CT scan). Studies were only ordered after a neurosurgical evaluation was performed and if there was a high index of suspicion for intracranial bleeding or an acute change in mental status. As per institution policy, DVT screening ultrasounds were not routinely performed, and evaluation of DVT was performed in setting of high clinical suspicion. Data was compiled, reviewed, and verified for accuracy by multiple independent reviewers.
Associations between categorical factors were examined using the chi-square test or Fisher’s exact test, or Pearson correlation coefficients. Associations between continuous factors (BMI, Age, APACHE score, APACHE III score, SAPS, MODS) were examined using the Mann-Whitney U test. LOS in the SICU was calculated using the product-limit method. Mortality was described using the Kaplan-Meier method. For all study measures, a p-value <0.05 indicated statistical significance. Data was collected and subsequently submitted to the biostatistics department for analysis. This study was approved by the Northwell Health System Institutional Review Board.
Results
We identified 1,152 neurosurgical patients, of which 223 emergency neurosurgical patients were included in this study. 100 (44.84%) received no anticoagulation, 123 (55.16%) patients received SCUFH, of which 88 (71.54%) within 24 h and 35 (28.46%) after 24 h. The mean number of days on SCUFH was 4 ± 5.4. Demographic data are detailed in Table 1. We found no statistically significant differences in age, ethnicity, sex, and patient condition upon discharge from SICU between the patients who did not receive heparin, those who received SCUFH within 24 h, and those who received SCUFH after 24 h.
Table 2 demonstrates the perioperative clinical characteristics. A statistically significant difference was noted with the admission MODS score (p-value=0.0009), and APACHE II (p-value=0.045), of patients receiving SCUFH to those not receiving heparin, but APACHE III and SAPS on admission were shown to have no difference in predicting DVT in this study. A statistical difference was also noted in the median SICU length of stay (LOS) across the different groups, 4 (2-7) days in patients without DVT prophylaxis, 5 (3-11) (SCUFH within 24 h) and 7 (3-13) (SCUFH after 24 h) (Table 2).
Figure 1 shows overall survival of the three groups. No instances of PE or HIT were observed during the study period. No postoperative hemorrhages (confirmed by CT scan of the brain) were observed in any of the neurosurgical patients with pre-operative diagnoses of subarachnoid hemorrhages (SAH), intracerebral hemorrhages, or subdural or epidural hemorrhage (Table 3).
A total of 52 neurologic complications and 123 total complications were identified (Table 4). We found no statistically significant difference in the incidence of these complications by group. Vasospasm (n=9 in no heparin group, n=9 in SCUFH ≤ 24 h, n=8 in SCUFH>24 h, p=0.091) and cerebrovascular accident (n=5, n=6, n=5, respectively, p=0.242) were the most common neurologic adverse events. Within the cerebrovascular accident subgroup, 1 patient was diagnosed in the group that receives heparin within 24 h with intracerebral hemorrhage upon admission to the SICU. Postoperative bleeding was observed in only one patient who received SCUFH within 24 h, and no cases of HIT or VTE were identified. Among non-neurologic complications, respiratory complications including ventilator associated pneumonia and technical issues related to intubation/extubation were most frequently encountered, occurring in 13 cases of patients without heparin, 14 in SCUFH ≤ 24 h and 8 in SCUFH>24 h (p=0.394). Cardiac complications were encountered in 9 patients (n=1, n=4, n=3, respectively, p=0.07), including cardiac arrhythmias, myocardial infarction and pulmonary edema. The main contributors of infectious complications were catheter-related complications.
| Parameter |
No heparin
n=100 |
SCUFH £ 24h
n=88 |
SCUFH>24h
n=35 |
(p) |
Total Patients
n=223 |
| Sex |
Sex, Female
n (%) |
58 (58.00) |
54 (61.36) |
23 (65.71) |
NS |
88 (39.46) |
| Age, (years) |
18-45, year/
n (%) 46-55, years
n (%) 56-65, years
n (%) >65, years
n (%) Total, years
Mean (SD) |
26 (26.00)
14 (14.00)
27 (27.00)
33 (33.00)
57.37 (6.46) |
19 (21.59)
15 (17.05)
18 (20.45)
36 (40.91)
59.35(17.20) |
8 (22.86)
7 (20.00)
9 (25.71)
11 (31.43)
57.51(15.21) |
NS |
53 (23.77)
36 (16.14)
54 (24.22)
80 (35.87)
58.17(16.52)
|
| Ethnicity |
Caucasian, n (%)
African American, n (%)
Asian, n (%)
Hispanic, n (%)
Other, n (%) |
54 (54.00)
7 (7.00)
10 (10.00)
28 (28.00)
1 (1.00)
|
58 (65.91)
5 (5.68)
9 (10.23)
14 (15.91)
2 (2.27) |
21 (60.00)
2 (5.72)
4 (11.43)
6 (17.14)
2 (5.71) |
NS |
133 (59.64)
14 (6.28)
23 (10.31)
48 (21.52)
5 (2.24) |
| BMI, kg/m2 |
Underweight (<19),
n (%) Ideal, (19-24.9)
n (%) Overweight, (25-29.9
)
n (%) Obese, (30-34.9)
n (%) Morbidly Obese, (>35)
n (%) Total, mean (SD) |
4 (8.33)
18 (37.50)
18 (37.50)
2 (4.17)
6 (12.50)
26.03 (5.64) |
6 (10.00)
30 (50.00)
18 (30.00)
6 (10.00)
0 (0.00)
24.32 (4.61) |
1 (4.55)
11 (50.00)
5 (22.72)
4 (18.18)
1 (4.55)
26.01 (5.48) |
NS |
11 (8.46)
59 (45.38)
41 (31.54)
12 (9.24)
7 (5.38)
25.24 (5.19) |
SCUFH: Subcutaneous Unfractionated Heparin; BMI: Body Mass Index; SD: Standard Deviation; NS: Non-Significant
Table 1: Demographic data of critically ill neurosurgical patients admitted to the SICU.
| Parameter |
No heparin n=100 |
SCUFH £ 24h n=88 |
SCUFH>24h n=35 |
(p) |
Total Patients n=223 |
| APACHE II, median (Q1-Q3) |
8 (4-14) |
9 (6.5-14) |
7 (3-13) |
0.045* |
9.95 (7.07) |
| APACHE III, median (Q1-Q3) |
31 (21-53) |
34 (23-52) |
7 (5-11) |
NS |
38.45 (25.76) |
| MODS |
Total, median (Q1-Q3) |
1 (0-2) |
0 (0-2) |
0 (0-0) |
0.0009* |
1.22 (1.84) |
| Score 0, % |
43.21 |
51.14 |
81.82 |
| Score 1-4, % |
49.38 |
43.18 |
12.12 |
| Score>4, % |
7.4 |
5.69 |
6.06 |
| SICU LOS, days median (Q1-Q3) |
4 (2-7) |
5 (3-11) |
7 (3-13) |
0.016* |
5.67 (5.08) |
| Ventilator, days median (Q1-Q3) |
|
0 (0-2) |
2 (0-3) |
2 (0-3) |
0.00005* |
3.60 (6.36) |
| Admitting acuity |
Emergency Surgery, n (%) |
49 (49.00) |
50 (56.82) |
22 (62.86) |
NS |
121 (54.26) |
| Emergency Room, n (%) |
51 (51.00) |
38 (43.18) |
13 (37.14) |
NS |
102 (45.74) |
| Mortality, n (%) |
Hospital Mortality |
14 (14.00) |
15 (17.05) |
2 (5.71) |
NS |
31 (13.90) |
| 30 Days-Mortality |
14 (14.00) |
15 (17.05) |
2 (5.71) |
NS |
31 (13.90) |
| SICU Mortality |
12 (12.00) |
14 (15.91) |
2 (5.71) |
NS |
28 (12.02) |
SCUFH: Subcutaneous Unfractionated Heparin; APACHE II: Acute Physiology and Chronic Health Evaluation II; APACHE: Acute Physiology and Chronic Health Evaluation; SAPS: Simplified Acute Physiology Score; MODS: Multiple Organ Dysfunction Score; SICU: Surgical Intensive Care Unit; LOS: Length of Stay; Q1: Lower Quartile; Q2: Upper Quartile; SD: Standard Deviation; *: Statistically Significant; NS: Non-Significant.
Table 2 Peri-operative characteristics of the use of SCUFH.
Discussion
This study aimed to evaluate the efficacy and safety of SCUFH in high-risk neurosurgical patients undergoing emergency surgery. We recently found that the use of SCUFH in the general neurosurgical population was safe, however, the potential adverse effects of SCUFH in the high-risk neurosurgery patients undergoing emergency surgery was largely unknown.
By collecting data on 1,152 patients-days at a single center, this large retrospective study identified several correlations between the patient demographics and perioperative characteristics with the risk of developing bleeding complications.
This trend may be related to the increased comorbidities and longer LOS seen in the heparin group, as these patients were selected to receive SCUFH whereas the less complex patients did not.
| Parameter |
No heparin
n=100 |
SCUFH £ 24h
n=88 |
SCUFH>24h
n=35 |
(p) |
Total Patients
n=223 |
| Adrenal crisis |
1 (1) |
0 |
0 |
NS |
1 |
| Berry aneurysm |
0 |
1 (1.14) |
0 |
NS |
1 |
| Brain abscess |
0 |
0 |
1 (2.86) |
NS |
1 |
| Brain carcinoma |
5 (5) |
2 (2.27) |
0 |
NS |
7 |
| Cervical spinal cord compression |
2 (2) |
1 (1.14) |
0 |
NS |
3 |
| Cervical vertebrae fracture |
0 |
1 (1.14) |
0 |
NS |
1 |
| Epidural abscess |
0 |
1 (1.14) |
0 |
NS |
1 |
| Epidural hematoma |
0 |
1 (1.14) |
0 |
NS |
1 |
| Intracerebral hemorrhage |
14 (14) |
19 (21.59) |
6 (17.14) |
NS |
39 |
| Meningioma |
1 (1) |
0 |
0 |
NS |
1 |
| Obstructive hydrocephalus |
3 (3) |
1 (1.14) |
0 |
NS |
4 |
| Paraplegia |
0 |
1 (1.14) |
0 |
NS |
1 |
| Subarachnoid hemorrhage |
49 (49) |
31 (35.23) |
24 (75) |
0.00046* |
104 |
| Subdural hematoma |
8 (8) |
9 (10.23) |
2 (5.71) |
NS |
19 |
| Others |
17 (17) |
20 (22.73) |
2 (5.71) |
NS |
49 |
(): Values are represented in percentage. SCUFH: Subcutaneous Unfractionated Heparin; *: Statistically Significant.
Table 3 Admitting diagnoses/procedures of critically ill neurological patients.
| Parameter |
No heparinn=100 |
SCUFH £ 24hn=88 |
SCUFH>24hn=35 |
(p) |
Total Patientsn=223 |
| Neurological complication |
Altered mental state |
1 (1) |
1 (1.14) |
0 |
NS |
2 |
| Bleeding |
0 |
1 (1.14) |
0 |
NS |
1 |
| Cerebrovascular accident |
5 (5) |
6 (6.82) |
5 (14.29) |
NS |
16 |
| Disseminated intravascular coagulation |
1 (1) |
1 (1.14) |
0 |
NS |
2 |
| Heparin-induced thrombocytopenia |
0 |
0 |
0 |
NS |
0 |
| Paraplegia |
0 |
1 (1.14) |
0 |
NS |
1 |
| Thrombophlebitis |
0 |
1 (1.14) |
0 |
NS |
1 |
| Vasospasm |
9 (9) |
9 (10.23) |
8 (22.86) |
NS |
26 |
| Ventriculitis |
1 (1) |
1 (1.14) |
1 (2.86) |
NS |
3 |
| Venous thromboembolism |
0 |
0 |
0 |
NS |
0 |
| Total neurological complications |
16 (16) |
21 (23.86) |
14 (40) |
0.017* |
52 |
| System-based complications |
Cardiac |
1 (1) |
4 (4.55) |
3 (8.57) |
NS |
9 |
| Respiratory |
13 (13) |
14 (15.91) |
8 (22.86) |
NS |
35 |
| Endocrine |
1 (1) |
4 (4.55) |
1 (2.86) |
NS |
6 |
| Infectious |
3 (3) |
6 (6.82) |
3 (8.57) |
NS |
12 |
| Gastrointestinal |
1 (1) |
1 (1.14) |
2 (5.71) |
NS |
4 |
| Renal |
2 (2) |
2 (2.27) |
1 (2.86) |
NS |
5 |
| Total Complications |
37 (37) |
52 (59.09) |
32 (91.43) |
2.12x10-8* |
123 |
(): Values are represented in percentage. SCUFH: Subcutaneous Unfractionated Heparin; *: Statistically Significant.
Table 4: Post-neurosurgical complications in patients.
Evaluation of the data and the Kaplan Meyer curve (Figure 1) demonstrated a significant p value when comparing no SCUFH to either arm of the heparin group. Since the non-heparin group had the worst survival and the heparin groups both had improved outcomes it could be inferred that the heparin improved survival. However, clinically is not significant as the data may be confounded. Patients may have been sicker or transfers from the SICU to the floor delayed. While our cohort was not randomized into the different treatment regimens, Table 1 shows that these groups were well matched.
Significant statistical association was noted with the multiple organ dysfunction score (Table 2). The MODS represents an attempt to develop reliable, reproducible measure of the severity of organ dysfunction at the time of ICU admission as well as quantify subsequent deterioration over the course of the ICU stay [17]. The MODS was constructed using simple measures of dysfunction in six organ systems and, therefore, may not be applicable to the emergency neurosurgical post-operative population.
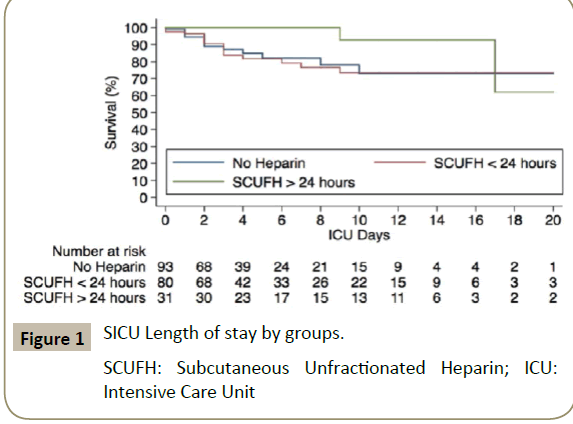
Figure 1: SICU Length of stay by groups.
SCUFH: Subcutaneous Unfractionated Heparin; ICU: Intensive Care Unit
We hypothesized that a number of other variables may affect the likelihood of post-operative VTE, including BMI, advanced age, anticoagulation medication (Table 1) and admitting diagnoses and procedures (Table 3). However, none of these hypotheses were statistically significant. It is possible that this study may be underpowered to detect these differences.
Abundant data from other meta-analyses and placebo-controlled, blinded, randomized clinical trials have demonstrated the overall safety of anticoagulation, as the marginally increased rates of bleeding with prophylactic doses of low-dose unfractionated heparin (LDUH), low molecular weight heparin (LMWH), or a vitamin K antagonist (VKA) are not of clinical significance [19,20]. Several studies support the usage in the neurosurgical population as well [21-24]. The belief that pharmacologic VTE prophylaxis should be withheld in any patient at increased risk for bleeding is largely unsupported by literature, it is yet a practice widely performed.
Prospective studies of neurosurgical patients who received perioperative LDUH prophylaxis, has not shown increased risk of intracranial bleeding. Studies show that perioperative administration of heparin does not significantly alter bleeding tendency by any measured parameter [25-30]. This analysis confirms previous conclusions and supports the usage of subcutaneous heparin, even in emergency neurosurgical patients. It is clear that the administration of SCUFH does not directly cause postoperative hemorrhage. Our findings support the above claims that the administration of subcutaneous heparin in the postoperative period is safe, even in patients with SAH.
Our Study has some limitations. First, although data were prospectively entered into the eICU database, our evaluation was retrospective. Thus, vulnerable to residual cofounding which could have explained the lack of association between both SCUFH groups and mortality. However, those uncaptured factors would need to have an overwhelming effect in order to hide that association, which we believe is highly unlikely. Second, given the lack of post-operative VTE or bleeding events we observed in Table 4, our study may not have sufficient power to show a significance association. Our failure to enroll and analyse a larger number of patients could have led to a type-II error. Because of limitations in our dataset, we were not able to measure the median time to the Operating Room since admission. Information that could have been helpful to better support the emergency nature from our cohort. Nonetheless, our cohort includes only the patients who receive neurosurgical intervention within the first 24 h post-admission. Finally, it should be noted that the years from 2008 to 2010 reflect a period of changing practice as regards corticosteroid usage in septic shock.
In spite of this limitation, our findings highlight the importance of the on-going controversies and discussions about the use of SCUFH in neurosurgical patients after emergency procedures. In addition, to our knowledge, this study is one of the largest single center studies on bleeding complications in emergency neurosurgical patients.
Conclusion
Based on the above analysis, the administration of SCUFH in emergency neurosurgical patient at 24 h, dosed accordingly to guidelines for thromboembolism, does not appear to be associated with increase post operatively bleeding and continues to be a safe and effective chemoprophylaxis against DVT. Our study suggests that for post-operative bleeding neurosurgical patients, the administration of SCUFH should be routinely used as a VTE prophylactic agent and that it is not an independent risk factor. Further studies are warranted in a controlled, multicenter, randomized way to confirm the safety and effectiveness use of SCUFH in the treatment and prevention against DVT.
Acknowledgement
We would like to thank the nurses and ancillary personnel in the MICU and SICU for their help in this study.
References
- Muscedere JG, Heyland DK, Cook D (2007) Venous thromboembolism in critical illness in a community intensive care unit. J Crit Care 22: 285-289.
- Anderson FA, Wheeler HB, Goldberg RJ, Hosmer DW, Patwardhan NA, et al. (1991) A population-based perspective of the hospital incidence and case-fatality rates of deep vein thrombosis and pulmonary embolism: The Worcester DVT Study. Arch Int Med 51: 933-938.
- Giorgi PM, Donadini MP, Dentali F, Ageno W, Marazzi M, et al. (2013) The short-and long-term risk of venous thromboembolism in patients with acute spinal cord injury: A prospective cohort study. Thrombosis and haemostasis 109: 34-38.
- Ho KM, Chavan S, Pilcher D (2011) Omission of early thromboprophylaxis and mortality in critically ill patients: a multicenter registry study. CHEST Journal 140: 1436-1446.
- Patel AP, Koltz MT, Sansur CA, Gulati M, Hamilton DK (2013) An analysis of deep vein thrombosis in 1277 consecutive neurosurgical patients undergoing routine weekly ultrasonography: Clinical article. J neurosurg 118: 505-509.
- Glotzbecker MP, Bono CM, Harris MB, Brick G, Heary RF, et al. (2008) Surgeon practices regarding postoperative thromboembolic prophylaxis after high-risk spinal surgery. Spine 33: 2915-2921.
- Schneck M (2013) Venous thromboembolism in neurologic disease. Handbook of clinical neurology 119: 289-304.
- Smith TR, Nanney AD, Lall RR, Graham RB, McClendon J, et al. (2015) Development of venous thromboembolism (VTE) in patients undergoing surgery for brain tumors: Results from a single center over a 10year period. J Clin Neurosci 22: 519-525.
- Sobieraj-Teague M, Hirsh J, Yip G, Gastaldo F, Stokes T, et al. (2012) Randomized controlled trial of a new portable calf compression device (Venowave) for prevention of venous thrombosis in high-risk neurosurgical patients. J Thromb Haemost 10: 229-235.
- Brambilla S, Ruosi C, La Maida G, Caserta S (2004) Prevention of venous thromboembolism in spinal surgery. Eur Spine J 13: 1-8.
- Hacker RI, Ritter G, Nelson C, Knobel D, Gupta R, et al. (2012) Subcutaneous heparin does not increase postoperative complications in neurosurgical patients: An institutional experience. J Crit Care 27: 250-254.
- Iorio A, Agnelli G (2000) Low-molecular-weight and unfractionated heparin for prevention of venous thromboembolism in neurosurgery: A meta-analysis. Arch Int Med 160: 2327-2332.
- Beck DH, Taylor BL, Millar B, Smith GB (1997) Prediction of outcome from intensive care: a prospective cohort study comparing Acute Physiology and Chronic Health Evaluation II and III prognostic systems in a United Kingdom intensive care unit. Crit Care Med 25: 9-15.
- Knaus WA, Draper EA, Wagner DP, Zimmerman JE (1985) APACHE II: A severity of disease classification system. Crit Care Med 13: 818-829.
- Knaus WA, Wagner DP, Draper EA, Zimmerman JE, Bergner M, et al. (1991) The APACHE III prognostic system. Risk prediction of hospital mortality for critically ill hospitalized adults. Chest Journal 100: 1619-1636.
- Le Gall J-R, Lemeshow S, Saulnier F (1993) A new simplified acute physiology score (SAPS II) based on a European/North American multicenter study. Jama 270: 2957-2963.
- Marshall JC, Cook DJ, Christou NV, Bernard GR, Sprung CL, et al. (1995) Multiple organ dysfunction score: a reliable descriptor of a complex clinical outcome. Crit Care Med 23: 1638-1652.
- Goldhaber SZ, Tapson VF, Committee DFS (2004) A prospective registry of 5,451 patients with ultrasound-confirmed deep vein thrombosis. Amer J Cardiol 93: 259-262.
- Clagett GP, Reisch JS (1988) Prevention of venous thromboembolism in general surgical patients. Results of meta-analysis. Ann Surg 208: 227.
- Nurmohamed M, Buller H, Dekker E, Hommes D, Rosendaal F, et al. (1992) Low-molecular-weight heparin versus standard heparin in general and orthopaedic surgery: A meta-analysis. The Lancet 340: 152-156.
- Bauman JA, Church E, Halpern CH, Danish SF, Zaghloul KA, et al. (2009) Subcutaneous heparin for prophylaxis of venous thromboembolism in deep brain stimulation surgery: Evidence from a decision analysis. Neurosurgery 65: 276-280.
- Gonda DD, Fridley J, Ryan SL, Briceño V, Lam SK, et al. (2015) The safety and efficacy of use of low-molecular-weight heparin in pediatric neurosurgical patients. J Neurosurg: Pediatr 16: 329-334.
- Kwiatt ME, Patel MS, Ross SE, Lachant MT, MacNew HG, et al. (2012) Is low-molecular-weight heparin safe for venous thromboembolism prophylaxis in patients with traumatic brain injury? A Western trauma association multicenter study. J Trauma Acute Care Surg 73: 625-628.
- Macdonald RL, Amidei C, Lin G, Munshi I, Baron J, et al. (1999) Safety of perioperative subcutaneous heparin for prophylaxis of venous thromboembolism in patients undergoing craniotomy. Neurosurgery 45: 245.
- Bauer KA, Rosendaal FR, Heit JA (2002) Hypercoagulability: Too many tests, too much conflicting data. ASH Education Program Book 2002: 353-368.
- Constantini S, Kanner A, Friedman A, Shoshan Y, Israel Z, et al. (2001) Safety of perioperative minidose heparin in patients undergoing brain tumor surgery: A prospective, randomized, double-blind study. J Neurosurg 94: 918-921.
- Geerts W, Cook D, Selby R, Etchells E (2002) Venous thromboembolism and its prevention in critical care. J Crit Care 17: 95-104.
- Kakkos SK, Caprini JA, Geroulakos G, Nicolaides AN, Stansby G, et al. (2016) Combined intermittent pneumatic leg compression and pharmacological prophylaxis for prevention of venous thromboembolism. The Cochrane Library.
- Stein PD, Beemath A, Olson RE (2005) Trends in the incidence of pulmonary embolism and deep venous thrombosis in hospitalized patients. Amer J Cardiol 95: 1525-1526.
- Wen DY, Hall WA (1998) Complications of subcutaneous low-dose heparin therapy in neurosurgical patients. Surg Neurol 50: 521-525.

