Keywords
Nosocomial infections; Hand washing; Glove utilization
Abbreviations
CDC: Center for Disease Control; HCW: Health Care Workers; UP: Universal Precautions; HICPAC: Hospital Infection Control Practice Advisory Committee; HLD: High Level Disinfection; OSHA: Occupational Safety and Health Administration; OPIM: Other Potentially Infectious Materials; WHO: World Health Organization; AIDS: Acquired Immune Deficiency Syndrome; HIV: Human Immune Virus; IUD: Intra Uterine Device
Introduction
One of the most recurrent themes with regards to the prevention of nosocomial infections in hospital has been the issue of hand washing and glove utilization among medical personnel. Knowledge and practice of hand washing and aseptic technique are very important in preventing the transfer of pathogen micro-organisms by nurses to their patients in the course of rendering care. It is considered as one or the most infection control measures. Nurses may harbor micro-organisms that are harmless to them but potentially harmful to patients if they find a route of entry. It is important that nurses wash their hands and maintain aseptic technique when carrying out health procedures because they are directly involved in providing a biologically safe environment for the patients. Micro-organism exists everywhere, in water, soil, air, body surface like the skin, intestinal tract, vagina, respiratory tract and urinary tract. Some micro-organisms are normal resident flora, while others invade the body and cause infection and disease that could either be asymptomatic, subclinical or clinical. These features make them vary in their virulence, pathogenesity and sepsis [1].
Nosocomial or hospital acquired infections- is infection that is neither present nor incubating at the time the patient come to the health care facility (hospital).Nosocomial refers to the association between care and the subsequent onset of infection and nosocomial infections are a significant problem throughout the world and are increasing [2].
In 1987, the Centers for disease Control and Prevention (CDC) developed universal precautions (UP) to help protect both health care workers (HCWs) and patients from infection with bloodborne pathogens in health care settings. The recommendations stress that blood is the most important source of HIV, HBV and other blood –borne pathogens, and that infection control efforts should be focused on the prevention of exposures to blood as well as the receipt of HBV immunizations. In 1996, however, the CDC’s Hospital Infection Control Practices Advisory Committee (HICPAC) introduced the concept of standard precautions, which states that a single set of precautions be used for the care of all patients in hospital regardless of their presumed infection status [3]. Standard precautions integrate and expand the elements of universal precautions into a standard of care designed to protect health care practitioners and patients from pathogens that can be spread by blood or by any other body fluid, excretion or secretion [4].
Study revealed that at any time over 1.4 million patients worldwide will have infectious complications acquired in the hospital. Hospital acquired infection poses a very real and serious threat to all who are admitted to hospital. Hand hygiene means either washing the hands with soap and water or hand antiseptics with an alcohol-based hand-rub. The efficacy of hand washing for the prevention of hospital acquired infections has been clearly demonstrated. To make hand washing easier and safer, new detergents and methods have been developed, tested, and were successful, integrated into many infections control guidelines [5-7].
However, under routine hospital conditions the compliance with hand washing by health care workers including nurses, Physicians, and others (e.g. physical therapists and radiologic technicians) is still unacceptably low.As the rate of compliance with hand hygiene in medical practitioners is low, and the US centers for Disease Control and Prevention (CDC) published a guide line for hand hygiene in health care settings in an effort to promote it [8].
A study conducted in Jimma university hospital in, south west Ethiopia, also showed that hand washing practice by the nursing staff will be inadequate. This study demonstrated that only 43.2% of the nursing staff practices adequate hand washing while 56.8% of them practice inadequate hand washing [9].
Despite the magnitude of Hospital acquired infections problems and the importance of adherence to infection control policies, hand hygiene practice has remained unacceptably low. Hand hygiene compliance rates in different developed countries rarely exceed 50%. For instance, figures show that in the USA it is 50%, in Switzerland 42% and in the UK 32%. Hence, poor compliance has resulted in high morbidity and mortality. In the USA, there are between 1.7 and 2 million people who contract hospital acquired infections and 88 to 99 thousand deaths are attributed to it annually. Furthermore, hospital acquired infections affect nearly 10% of hospitalized patients and presents major challenges in healthcare facilities. Consequently, annual medical expenses have increased in the USA to approximately $4.5 billion [10].
One of the most important infection control measures is hand hygiene. In Turkey, the compliance of health-care workers is generally poor (<33%). The major reasons for non-compliance are heavy workload, inadequate structure (lack of sinks, difficult access to hygiene products), and behavioral aspects [11].
As proper glove utilization and appropriate hand washing practice has of paramount importance to reduce and prevent hospital acquired infections, it is important that all health care workers must have adequate knowledge and practice and compliance with proper hand washing and glove utilization. In Agaro health center and hospital there is no formal research conducted on this subject matter, and therefore it is necessary to conduct a baseline study to determine the knowledge and practice of hand washing practice and glove utilization with the standard, so that compliance with the standard will be recommended.
Materials and Methods
An institutional based cross- sectional study design was conducted at Agaro health center and hospital from February 1-3, 2015. Agaro health center and hospital contain 17 and 63 health care providers respectively. The sample size was determined by using census method (Since the number of study participants were less than one hundred (N =73) and all health care providers were included in the study (n=73) except pharmacists. Pharmacists were excluded from the study because their frequency of contact with the patient is not as much significant.
Data was collected using pre-tested structured and semi structured questionnaire that developed after a thorough review of literature on the subject matter. The tool contained three parts, part I-Socio-demographic information with 8items, part II-Practice questions with 12 items and Part-III-Knowledge questions with 16 items.
The data was analyzed and processed using SPSS for windows version 20 so that percentages and frequencies of the findings were identified and presented in texts, tables and figures.
Ethical clearance letter was obtained from ethical review board of Jimma University College of health sciences and the school sent a one page letter of permission to Agaro health center and hospital administrators. The administrators read the purposes of the study and gave their letter of permission. Explanation about the objective, method as well as the benefit of the study was given to the study population for their full-co-operation.
Result
Socio demographic distributions of the study participants
From all respondents 83.6% of respondents’ age lie between 20 – 29 age group. Moreover, 61.9% of the study participants had 1 – 5 years of service (Table 1).
| Category |
Frequency |
Percentage |
| Age |
20-29 |
61 |
83.6 |
| 30-39 |
10 |
13.7 |
| 40 and above |
2 |
2.7 |
| Total |
73 |
100 |
| Ethnicity |
Oromo |
54 |
73.9 |
| Amhara |
16 |
21.9 |
| Tigre |
3 |
4.2 |
| Total |
73 |
100 |
| Religion |
Orthodox |
28 |
38.4 |
| Muslim |
27 |
36.9 |
| Protestant |
17 |
23.3 |
| Others (wakefeta) |
1 |
1.4 |
| Total |
73 |
100 |
| Marital status |
Single |
45 |
61.7 |
| Married |
27 |
36.9 |
| Others (engaged) |
1 |
1.4 |
| Total |
73 |
100 |
| Years of service |
Less than 1 year |
6 |
8.3 |
| 1 - 5 years |
45 |
61.6 |
| More than 5 years |
22 |
30.1 |
| Total |
73 |
100 |
Table 1: Socio demographic distributions of respondents in Agaro health center and hospital, 2015.
Frequency and percentage distribution of study population by occupation and sex
Most of the study participants, 45.2% were nurses from that 32.8% of them were males followed by midwives accounting 21.8% from whom only 5.4% of them were females and the least in numbers were Health officers with 2.7%. Generally, from all health care providers males were the predominant (77%) (Table 2).
| Category of staffs |
Male |
Female |
Total |
| No |
% |
No |
% |
No |
% |
| Physicians |
6 |
8.2 |
2 |
2.7 |
8 |
10.9 |
| Nurses |
24 |
32.8 |
9 |
12.3 |
33 |
45.2 |
| Dentists |
3 |
4.1 |
- |
- |
3 |
4.1 |
| Midwives |
12 |
16.4 |
4 |
5.4 |
16 |
21.8 |
| Lab Technologists |
7 |
9.5 |
- |
- |
7 |
9.5 |
| Anesthetists |
3 |
4.1 |
1 |
1.3 |
4 |
5.4 |
| Health officers |
1 |
1.3 |
1 |
1.3 |
2 |
2.7 |
| Total |
56 |
77 |
17 |
23 |
73 |
100 |
Table 2: Frequency and percentage distribution of study population by occupation and sex among HCWs of Agaro health center and hospital, 2015.
Knowledge of hand washing and glove utilization
All study participants have knowledge of hand washing and glove utilization.
Practice of hand washing and glove utilization
Almost all 72 (98.6%) of the study participants practiced hand washing before and after individual patient contact and after contact with body secretions, but only 1 (1.4%) of the study participant didn’t practice hand washing and raised unavailability of sink for not practicing it. The study participants also reported that the frequency of hand washing practice depends on the patient flow and varies from day to day. All of the study participants wet their hands under running water before applying soap and 64 (88%) of them always used soap or other antiseptic solutions during hand washing. Majority, 52 (71.2%) of the study participants applied soap and alcohol for total duration of 15 seconds and the rest for less than 15 seconds. Majority, 70 (95.8%) of the study participants had adequate practice of glove utilization.
Frequency and percentage distribution of antiseptic solutions used by health care providers
59%, 16.4% and 24.6% of health care providers used Soap, Alcohol and Soap with Alcohol respectively for hand hygiene (Figure 1).
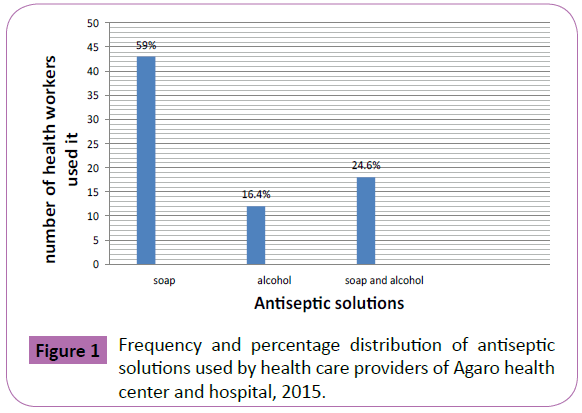
Figure 1: Frequency and percentage distribution of antiseptic solutions used by health care providers of Agaro health center and hospital, 2015.
Frequency distribution of methods of hand drying after hand washing by health care providers
Most of the study participants (70%) use air for hand drying and only 21% of the participants used towel for hand drying after washing their hands (Figure 2).
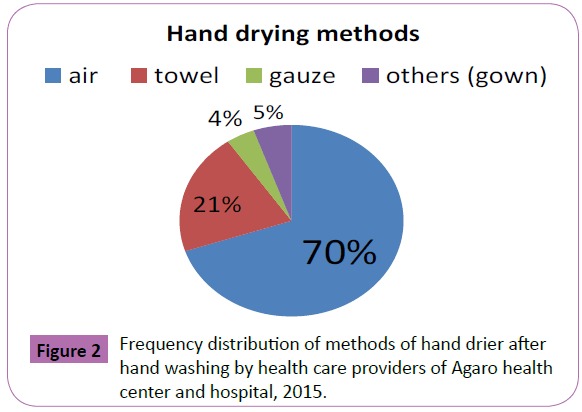
Figure 2: Frequency distribution of methods of hand drier after and washing by health care providers of Agaro health center and hospital, 2015.
Discussion
Over all in this study almost all, 70 (96%), of the study participants believed that hand washing is the single most effective mechanism to prevent the spread of infection even before and after gloving. A survey of approximately 200 health care workers noticed that 89% recognized hand washing as an important means of preventing infections [12]. The discrepancy might be because of sample size and study area difference.
Majority, 59 (80.9%), of the respondents said that many infections in the health care facilities are preventable with proper and consistent hand washing. Other study puts the importance of proper hand washing is to perform correctly the various procedures in reducing transmission of infections and therefore decreasing the frequency of nosocomial infection in patients, by using antiseptic solutions to inhibit growth or kill microorganisms on the hands [13].
Out of 73 study groups 63 (86.3%) of them agreed that hands should be washed by applying soap for at least 15 seconds. All of the study participants agreed that effective hand washing consists of wetting, soaping, applying friction, rinsing and drying adequately. All of the study participants agreed that medical personnel should always wash their hands before and after contact with a client and immediately after contact with blood, secretions or excretions. But other evidence shows that health care provider always needs to moisten and apply soap at least for 10 seconds or antiseptic solution and wash their hands before individual patient contact and after contact with blood, body secretions or execrations. Effective hand washing includes wetting, soaping, and applying friction, rinsing and drying adequately [14] which are consistent to each other.
In this study, 43 (59%), of the study participants used soap followed by soap and alcohol, 18 (24.6%), for washing their hands. Of those who practiced hand washing, 51 (70%), of them dried their hands by air followed by towel, 15 (21%). But Since 2005 research by creed on S.A indicate that alcohol based hand rub or 70% isopropanol (99-99.9%) kills bacteria most effectively but that antimicrobial soap or chlorhexadine (88-90) continues to destroy them for some time after the initial application. Soap (<60%) appears least effective [15]. Even if soap is the least effective in destroying microorganisms, majority of the health care workers used it. This discrepancy may be due to economical difference of the study area.
All of the study participants reported that examination gloves should be changed as soon as possible when visibly soiled, torn or punctured. All of the study participants thought that sterile glove should be used for blood drawing, IV insertion and removal, pelvic examination, IUD insertion and removal and for procedures involving contact with tissue deep under the skin (e.g. cesarean section). All of the study participants agreed that utility glove should be used for handling and cleaning instruments, handling contaminated wastes and cleaning blood or body fluid spills. It is consistent with reference pointing: Surgical staffs are required wearing sterile or high level disinfected gloves and when needed examination gloves are used but in case of like blood pressure check, temperature check and injection glove is not required. Exam gloves and HLD surgical glove is preferred and acceptable for blood drawing, IV insertion and removal, pelvic examination, IUD insertion and removal (with no -touch technique).Sterile/ high level disinfectant surgical, HLD Surgical glove is preferred and acceptable for the health worker to use for procedures involving contact with tissue deep under the skin (e.g. cesarean section). Utility or heavy-duty household glove, a health worker should use for handling and cleaning instruments, handling contaminated wastes and cleaning blood or body fluid spills [16].
Conclusion
Based on the finding it was concluded that the knowledge and practice of the study participants regarding hand washing and glove utilization was adequate.
According to this study, almost all, 72 (98.6%)of the study participants practiced hand washing before and after individual patient contact and after contact with body secretions, but only 1 (1.4%) of the study participant didn’t practice hand washing and raised unavailability of sink for not practicing it.
Majority, 43 (59%), of the study participants used soap for hand washing.
Almost all 70 (96%) of the study participants believed that hand washing is the single most effective mechanism to prevent the spread of infection.
Authors’ contributions
Both TL and BF participated in the design and analysis of the study. TL searched the databases, and wrote the first and second draft of the article. BF reviewed proposal development activities and each drafts of the result article. Finally, both authors revised the manuscript and approved the final version.
Acknowledgement
First and foremost we would like to greatly thank the almighty God, the foundation of knowledge and wisdom for enabling us to achieve this task.
We would like to extend our acknowledgement to Jimma University Department of Nursing and Midwifery for their support in different ways for conducting this research.
Moreover, we would like to express our respect to Agaro Health center and Hospital administrators and health care providers for their permission to carry out this study in their facility and we extend our thanks for all our associates involved in this research work.
References
- Alvarado CJ (2000) The Science of Hand Hygiene a Self Study Monograph. University of Wisconsin Medical School and SCI –health Communication 21: 231-233.
- Akyol AD (2007) Hand hygiene among nurses in Turkey: opinions and practices.J ClinNurs 16: 431-437.
- Bagg J, Jenkins S, Barker GR (1990) A laboratory assessment of the antimicrobial effectiveness of glove washing and re-use in dental practice.J Hosp Infect 15: 73-82.
- Alemu BS, Bezune AD,Joseph J,Gebru AA, Ayene YY , et al. (2015) Knowledge and Practices of Hand Washing and Glove Utilization Among the Health Care Providers of Shenen Gibe Hospital, South West Ethiopia. Science Journal of Public Health 3: 391-397.
- Centers for Disease control (2015) Community-associated MRSA Information Clinicians.
- Creedon SA (2005) Healthcare workers' hand decontamination practices: compliance with recommended guidelines.J AdvNurs 51: 208-216.
- Conley JM, Hill S, Ross J, lertzman J, Louie T (1989) Hand washing practices I an intensive care unit. The effects of an educational program and its relationship to infection rates. Is J infecting control. 17:330-339.
- Aragon D, Sole ML, Brown S (2005) Outcomes of an infection prevention project focusing on hand hygiene and isolation practices.AACN Clin Issues 16: 121-132.
- Takahashi I, Osaki Y, Okamoto M, Tahara A, Kishimoto T,et al. (2009) The Japanese Society for Hygiene 2: 643-654.
- Kristy Ménage Bernie (2002) Clinician’s Corner If the Glove Fits, Wear It. The Journal of Practical Hygiene 53-54.
- WHO guidelines on hand hygiene in health care (2009) First global patient safety challenge-clean care is safer care. Geneva, WHO.
- Korniewicz DM, Laughon BE, Cyr WH, Lytle CD, Larson E (1990) Leakage of virus through used vinyl and latex examination gloves.J ClinMicrobiol 28: 787-788.
- N Hawkes, D Kovach, M Al-Shehri, R Wray, R Freeman, et al. (2005) Perspective Assessment of Hand Hygiene Practices at a Tertiary Care Pediatric Hospital 54.
- Motamed N, BabaMahmoodi F, Khalilian A, Peykanheirati M, Nozari M (2006) Knowledge and practices of health care workers and medical students towards universal precautions in hospitals in Mazandaran Province.East Mediterr Health J 12: 653-661.
- Zegeyewondie (2003) Knowledge and practice of hand washing among the nursing staff of Jimma university hospitalpp: 1-25.
- Uti OG, Agbelusi GA, Jeboda SO, Ogunbodede E (2009) Infection control knowledge and practices related to HIV among Nigerian dentists.J Infect DevCtries 3: 604-610.

