Keywords
Physiological changes of teeth, Age estimation, Root translucency.
Introduction
Examination of teeth in many ways form a unique part of human body as they are most durable
and resilient part of the skeleton. The science dealing with establishing identity of a person by
teeth is popularly known as Forensic Odontology or Forensic Dentistry [1]. Many variables have
been used as age determinants and even dental histological techniques can contribute to age
estimation. [2]. The choice to use teeth for age determination is well accepted due to their
longevity ability of being resilient to change[3] There are various physiological changes which
are related to age such as Attrition, Periodontal bone loss, Root resorption, Root translucency,
Cementum apposition and Secondary dentin deposition.[4] Thoma[5] in 1944 described the age
changes occurring in the dental tissue and notes attrition of enamel, sclerosis of dentin, denticles
in the pulp, deposition of cementum, continuous eruption of the teeth and alteration in the
periodontal structures.Gustafson[6] in 1950 suggested the use of six retrogressive changes and
ranked them on arbitrary scale, allotting 0-3 points according to degree of the change. Dalitz [7]
re– examined Gustafson method and suggested a five point system from 0 – 4 instead of the four point system that was previously used. This change was proposed in order to give a slightly
greater efficacy. Bang and Ramm[8]suggested a totally new approach in age estimation. They
found that the root dentine appears to become transparent during the third decade starting at the
tip of the root and advancing coronally with age. This alteration is believed to be caused by
increasing intratubular calcification in dentinal tubules. [9] Johanson [10] in1971 in his research
used same six criterions but different ranking scale and then estimated the age of an individual.
Solheim [11] used in situ teeth and eight variables which included two of color estimate, two for
periodontosis, and two for attrition, crown length and sex. None of the changes took singly
proved more accurate than when these were studied together. [12]
Materials and Methods
The research project was carried out in the department of oral Pathology of Jaipur Dental
College; Jaipur Cases received for extraction by Department of Oral & Maxillofacial Surgery
Jaipur Dental College 20 cases were studied (age group of 20 to 60 years). The following dental
parameters were studied in each case; Attrition, Periodontal disease, Cementum apposition,
Secondary dentine deposition, Root translucency and Root resorption. The armentarium used in
the study are Electric lathe, Carborundum stone (rough and smooth), Alcohol and Xylene,
Formalin, Microscope and slides. The extent of periodontal disease was recorded before the
extraction of the tooth. Ground section was prepared by hand grinding which was done first with
lathe and then with rough Carborundum stone until a section of 1 mm was obtained and at this
thickness, the root translucency was noted. Grinding was further done using fine stone until the
section of 0.25-mm thickness is left. Finally, cleaned and dried section was mounted on slide and
viewed under microscope for secondary dentine, cementum apposition and root resorption.
Normal healthy teeth with class 1 occlusion were included in this study. The order of preference
was Premolar – Canines – Incisors. While Third molar, patients with medical & drug history,
trauma from occlusion, abnormal oral habits, congenital anomalies of teeth, pathologies affecting
teeth were excluded. The scores obtained were tabulated. By plotting actual age on one side and
the calculated score on the other side then the regression formula obtained [13] then age
estimation was done, deviation of estimated age from actual age noted and results subjected for
statistical analysis.
Four point allotment system as per Gustafson’s method [14]
Attrition (A):
A0- No Attrition,
A1- Attrition limited to enamel level,
A2- Attrition limited to dentine level,
A3- Attrition up to pulp cavity.
Periodontal disease (P):
P0-No obvious periodontal disease,
P1-Beginning of periodontal disease but no bone loss,
P2-Peridontal disease more than 1/3rd of the root,
P3-Peridontal disease more than 2/3rd of the root.
Secondary dentine (S):
S0-No secondary dentine formation,
S1-Secondary dentine up to upper part of pulp cavity,
S2-Secondary dentin up to 2/3rd of the pulp cavity,
S3-Diffuse calcification of entire pulp cavity.
Root translucency (T):
T0- No translucency,
T1- Beginning of translucency,
T2- Translucency more than 1/3rd of the apical root,
T3- Translucency more than 2/3rd of the apical root.
Cementum apposition (C):
C0- Normal cementum,
C1- Thickness of cementum more normal,
C2- Abnormal thickness of cementum near the
apex of the root,
C3- Generalized abnormal thickness of cementum throughout the apex of the root.
Formula used = Y= 4.07x + 10.35 (Y = Age in years, X = Total score)
Table. 1 shows age wise distribution of the patients
Table 2 shows the difference between actual age and estimated age
Results
Four groups of the patients were made (20 -29, 30 -39, 40-49 and > 50) 5 patients from each
groups were selected.
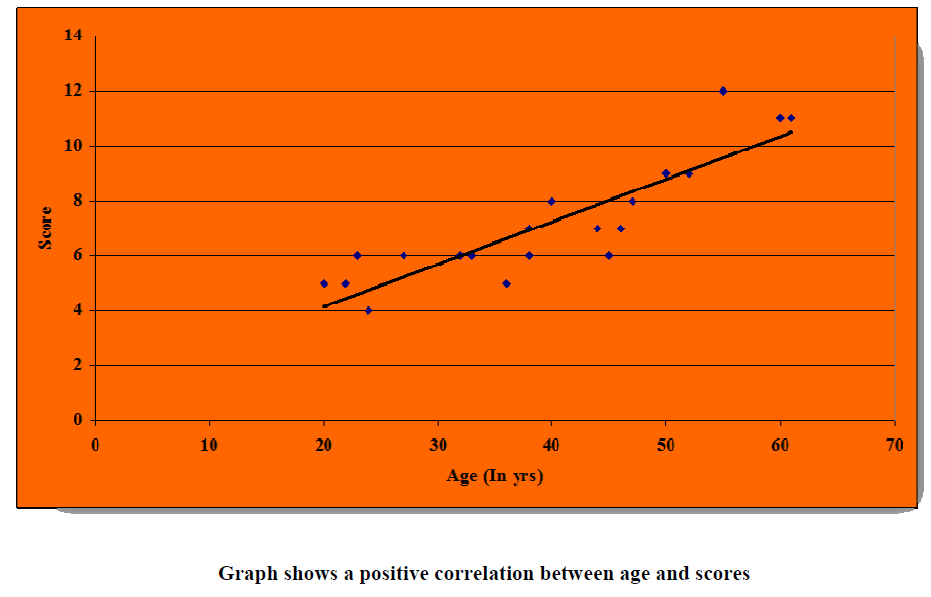
Table 3 shows Correlation and the significance of age groups with estimated age
Discussion
Total of 20 cases taken in this study and 6 physiological changes were recorded. Cases were
divided into 4 different age groups from 20 – 60 yrs of age 41% males & 59% females 55% nonvegetarian
& 45% vegetarian.
The mean age difference of the calculated age was ± 4.86 years which was contrary to the
findings of Gustafson who found the age difference of ± 3.63 years and also differs with the
findings of Singh. A et al.[15] Who found the mean age difference of ± 2.16 years. It was
observed that the total score increased with the increasing age & the increase was statistically
analyzed and was found to be significant (Pillai & Bhaskar 1974) [14] on comparing the means
of both the calculated age and the actual age, it was observed that the difference between them was statistically significant except in the age group of 40-50 years group. On calculating the
maximum and minimum difference between actual age and the calculated age, least difference in
actual age and calculated age on basis of 6 physiological criteria's in all 4 age groups. In our
study we got the mean age difference of ± 4.86 which was greater then some previous studies in
our opinion it was most likely due to the small sample size.
Conclusion
Age estimation from human teeth is well established. Different techniques and numerous studies
have been published for age estimation, each one shows different accuracy and reliability. Error
is present in every approach; to minimize the error one should perform repetitive measurements
and calculations in order to reach a reliable conclusion. Physiological changes like attrition,
periodontal disease, secondary dentin formation, root translucency, cementum apposition & root
resorption noted in this study that could help in the age estimation. It was also observed that the
total score increased with the increasing age
References
- Parikh CK: Parikh Text Book of Medical Jurisprudence and Toxicology. Identification in Mass Disasters: CBS Publishers and Distribution. Bombay: 5th edition: 1990: p. 76
- Sengupta. A., D.K. Whittaker and R.P Shellis 1999 Arch. Oral. Biol., 44(11): 889 – 899.
- Prince,.D.A , L.W Konigsberg ; J. Forensic. Sci., 53(3): 578 – 587.
- Gustafson G; Journal of American Dental Association: 1950.
- Thoma. K.H, 1, Oral Pathology. St. Louis: C.V Mosby company.
- Gustafson. G; 1. Microscopic examination of the teeth as a means of identification in Forensic medicine J.A.D.A, 35: 720.
- Dalitz, G.D., 1962. J. Forensic. Sci. Int., 153: 208 – 212.
- Bang. G, E. Ramm, Acta. Odontol. Scand; 28
- Vasiliadis, L., 1981. Root dentine translucency. Ph.D Bristol University UK.
- Lucy D, Aykroyd RG, Pollard AM, Solheim T: Journal of Forensic Science: 1996: 41 (2): 189-194.
- Solheim T., Sundnes PK.: Forensic Sci Int 1980; 16(1) : 7 – 18.
- Stavrianos, C., Mastagans, D., Karaisko, O., 2008 Research Journal of Medical Sciences. 2(5): 258 – 268.
- Vij K: Textbook of Forensic Medicine and Toxicology. Identification: B.I.Churchill Livingstone: Second Edition: 2002: 4: 71- 72.
- Pillai PS, Bhaskar G: Journal of Forensic Science: 1974: 3: 135-141.
- Pillai VV: Text Book of Forensic Medicine and Toxicology. Identification. Paras Publishers. Bangalore. 14th edition; 2004: p. 68