Keywords
Lead; Chelating effects; Food supplement; Aloe vera
Introduction
Lead is a ubiquitous toxic element existing more and more frequently in contaminated environments. Lead toxicity henceforth is becoming an important public health problem. Once consumed, it affects in large quantity the nervous system. Even small quantities would accumulate in the kidneys, liver, bones, cardiovascular, reproductive as well as gastrointestinal systems [1].
Lead contaminated water in a lake by the side of mining industry in US has been alarming international news. The presence of lead in household tap water in Hong Kong has aroused as much deep concerns. According to a report given by the World Health Organization (WHO) in 2010, one of the major sources of children’s exposure to lead is related to the drinking-water systems with lead solders and lead pipes. People become particularly worried when their children are found to have lead in the blood. The blood level could be just below the “level of concern” viz., around 10 ug/dL, yet knowing that there is no perfect understanding about its excretion, it remains a dreadful issue.
For the genuine lead poisoning, presenting with clinical symptoms and signs, there are a number of pharmaceutical chelating agents available for the detoxification of lead accumulated within our bodies: Dimercaptosuccinic acid (DMSA) has been recommended for the treatment of lead poisoning in children by poison control centers around the world [2]. Other common chelating agents include ethylenediamine tetraacetic acid (EDTA), 2,3- dimercaptopropanesulfonic acid (DMPS), thiamine tetrahydrofurfuryl disulfide (TTFD) and alpha lipoic acid (ALA). DMPS and ALA are used in conventional and alternative medicine. EDTA and DMSA, but not DMPS and TTFD, have been approved for the removal of lead by the US Food and Drug Administration. These drugs are bound to the lead molecules in the body thus preventing them from attaching to other tissues, and finally get eliminated through the kidneys and gastrointestinal tract.
However, it is important to note that proper chelating therapy will lead to serious adverse effects, which include dehydration, anemia, low blood calcium, damages to the kidneys and liver, allergic reactions, and nutritional defects [3]. When administered inappropriately, chelation therapy also increases the risks of cancer development and neurodevelopmental disorders, even death [4,5]. Chelating therapy should therefore never be considered unless the blood lead level reaches above 45 ug/dl [3]. For the less severe in toxications, some other safe interventions are very much needed.
Developing a Food Supplement with Chelating Effects
Aloe vera and Pectin have been reported to be able to bind metal ions, in particular, those of lead. They are therefore chosen as key items for the development of the supplement. Many scientific reports on the effects of pectin related to lead removal are already available [6-10]. Pectin is reported to be able to reduce the retention of lead in the blood, and organs (liver, kidney, heart, brain and bones) of animals.
On the other hand, A. vera has not been studied in animals on lead removal. However, in the recent decade, A. vera has been suggested to be a potential “green product” that can be used for lead removal since it was found capable of adsorbing to large amounts of Pb(II) from lead containing solutions [11]. Chemical modification of A. vera with phosphoric acid even increased the adsorption ability of A. vera for Pb(II) from waste water [12]. Scientific literature reporting the in vivo efficacy of A. vera on lead removal has yet to be found.
In the current study, we plan to evaluate the in vivo effects of the extracts of pectin and A. vera on the removal of lead ions in both chronic and acute lead toxications. This study can provide valuable scientific data to demonstrate the in vivo efficacy of pectin and A. vera to remove lead from the blood and internal organs. The outcome might lead to further clinical studies.
Methodology
Preparation of pectin and Aloe vera
The pectin and the aloe extracts were purchased commercially in powder forms (namely Pectin and Aloe Extract in the current study). The pectin was extracted from apples. Fresh aloe was also provided from a local farm. The green skin was peeled off and only the interior pulp was used. The pulp was cut into rectangular strips for tests of direct Lead binding, and alternatively, blended into a paste to feed the rats (Fresh Aloe) for the biological studies. The pulp could also be completely dried and concentrated in an oven and then blended into the powder form (Conc. Aloe Powder). Pectin, the commercial Aloe extracts and the concentrated aloe pulp powder were dissolved in distilled water to make a suspension with the following concentrations:
• Pectin: 100 mg/kg, low dose for the treatment of chronic toxication.
• Pectin: 500 mg/kg, for the treatment of acute toxication.
This was considered as nutritional dose because it corresponded to 35 g of pectin is recommended to be consumed per day by a human [9].
• Commercial aloe extract and concentrated aloe pulp powder: 1 g/kg. It was the maximum amount that could be delivered via the gavage tube.
• Fresh aloe pulp: 7.0 g/kg. This amount was equivalent to the volume of the commercial aloe extract and the concentrated aloe pulp powder suspension to be fed to the rats.
Animal and grouping
A total of 80 male Sprague-Dawley rats (135.4 ± 13.1 g) were obtained from the Laboratory Animal Services Centre of the Chinese University of Hong Kong (CUHK). The animal study had been approved by the Animal Experimental Ethics Committee of CUHK. The rats were divided into 16 groups and the experiment was divided in two parts (Figure 1):
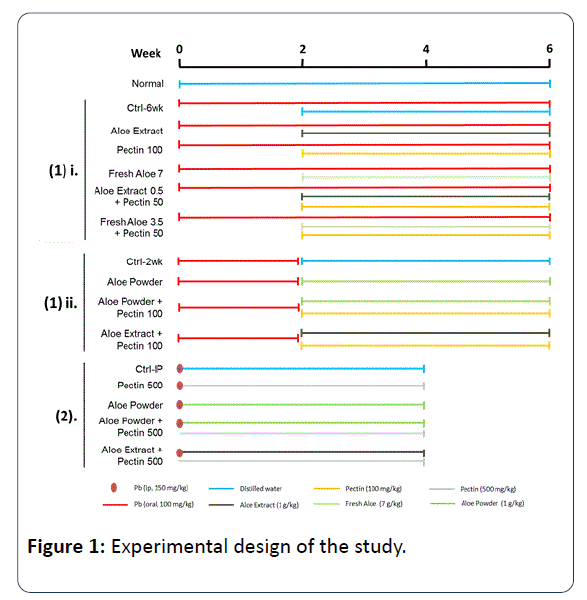
Figure 1: Experimental design of the study.
Prolonged lead toxication: The rats were fed with lead (II) acetate trihydrate solution (100 mg/kg/day) orally using gavage tube daily. This amount was of high lead content suitable to be classified as severe lead toxication and a rapid accumulation of the lead in the blood, organs and bones of the animals was expected [9]. However, it was only 10% of the lethal dose according to Reinholz et al. [13].
Details of the two treatment plans were implemented as follows: To mimic chronic lead toxication, oral lead solution was given daily and continuously for 6 weeks. Starting from the third week, additional daily treatment with different types of forced feeding (2 ml each) were given to the six groups of animals for four weeks:
• Distilled water as control (Ctrl-6 week);
• Commercial aloe extracts (Aloe Extract) (1 g/kg);
• Pectin (100 mg/kg);
• Fresh aloe pulp (Fresh Aloe) (7 g/kg);
• Commercial aloe extract (Aloe Extract) (0.5 g/kg)+Pectin (50 mg/kg);
• Fresh aloe pulp (Fresh Aloe) (3.5 g/kg)+Pectin (50 mg/kg).
To mimic moderate lead toxication, oral lead water was given daily for only 2 weeks and then discontinued, to be followed by the daily oral treatment of four different types of forced feeding (2 ml each) for four weeks:
• Distilled water as control (Ctrl-2 week);
• Fresh aloe pulp powder (Conc. Aloe Powder) (1 g/kg);
• Fresh aloe pulp powder (Conc. Aloe Powder) (1 g/kg) +Pectin (100 mg/kg);
• Commercial aloe extract (Aloe Extract) (1 g/kg)+Pectin (100 mg/kg).
Acute toxication: One single high dose of lead (II) acetate trihydrate solution (150 mg/kg) was injected intraperitoneally into the rats. This concentration was 75% of the LD50 of lead (II) acetate trihydrate [14]. It mimicked the severe acute lead toxication but was non-lethal. The efficacy of chelating agents on the detoxification of lead could be demonstrated clearly using this model. From the next day, the following oral treatments (2 ml in volume) were given to the rats daily, for a total of 4 weeks:
• Distilled water as control (Ctrl-IP);
• Pectin (500 mg/kg);
• Fresh aloe pulp powder (Conc. Aloe Powder) (1 g/kg);
• Fresh aloe pulp powder (Conc. Aloe Powder) (1 g/kg) +Pectin (500 mg/kg);
• Commercial aloe extract (Aloe Extract) (1 g/kg)+Pectin (500 mg/kg);
One additional group of rats did not receive lead toxication and acted as Normal control.
The rats were anaesthetized (cocktail of ketamine and xylazine mixture, 70 mg/kg and 10 mg/kg, respectively, i.p.) for blood collection from the inferior vena cava. The blood samples were kept in EDTA blood collection vials for the measurement of lead concentration in blood. The rats were then euthanized via cervical dislocation immediately after the blood collection. The Kidneys, liver and femur (only the cortical mid-shaft) were harvested for the measurement of tissue lead concentrations. All the tissues collected were washed with deionized water, blotted to dry on Kim wipes tissue and stored in acid-washed plastic containers at -80°C, until they are ready for lead concentration analysis.
The blood samples were prepared by the skilled laboratory operators of the University Pathology Service, CUHK. The lead concentration was analyzed using the inductively coupled plasma mass spectrometry (ICP-MS) and internal quality control was performed for the quality assurance of the measurement. The kidney and liver samples were homogenized separately. About 20 mg of the homogenized tissue was weighed into an acid-washed glass tube and then digested by adding 1ml nitric acid diluted with hydrogen peroxide. The samples were sonicated at 80 kHz in 70°C for 50 min.
All the data were presented as mean ± standard error of mean (SEM). The statistical significant differences between the treatment groups and their corresponding control groups were tested by one-way ANOVA with Uncorrected Fisher's LSD as multiple-comparison post-test using Graph pad Prism 6. All the statistical tests were two-sided, with p<0.05 as considered statistically significant.
Results
Lead contents in blood and tissues of rats
The lead contents in the blood of rats were elevated as expected after the animals consumed lead water (Table 1). Continuous oral administration of the lead water daily from week 2 to week 6 boosted the blood lead concentration from 0.286 to 1.328 umol/L which was significantly higher than that of the Normal (p=0.032). Intraperitoneal injection of lead water yielded the highest blood lead concentration (2.814 umol/L) (p<0.001 vs. Normal).
| Blood (umol/L) |
Liver (umol/g) |
Kidney (umol/g) |
Femur (umol/g) |
| Normal |
0.001 ± 0.000 |
<0.001 |
<0.001 |
<0.001 |
| Ctrl-6wk |
1.328 ± 0.090* |
0.006 ± 0.001 |
0.033 ± 0.004** |
0.600 ± 0.140** |
| Ctrl-2wk |
0.286 ± 0.039 |
<0.001 |
0.005 ± 0.001 |
0.217 ± 0.023 |
| Ctrl-IP |
2.814 ± 0.372*** |
1.044 ± 0.282** |
0.040 ± 0.005*** |
0.538 ± 0.091** |
Table 1: Lead concentration in blood and tissues of rats after lead water administration. *p<0.05, **p<0.01, ***p<0.001 vs. normal.
The lead concentrations in the tissues of normal rats was very low (<0.001 umol/g). Accumulations of lead in the kidney and femur were found after 2 weeks of lead water feeding. After 6 weeks of lead water feeding, the lead concentration in these two tissues became even higher than that of the normal rat (0.033 and 0.600 umol/g, respectively). One high dose of lead water injection intraperitoneally led to dramatically high levels in lead concentrations in all the tissues (1.044, 0.040 and 0.538 umol/g for the liver, kidney and femur, respectively).
Effects of Aloe vera and pectin on lead concentration in Blood: After 6 weeks of continuous consumption of lead water, in spite of treating with A. vera or pectin or combined, starting from the third week, there was no obvious decline in the lead concentration in the blood (Figure 2A). When the rats were fed with lead water for only 2 weeks, followed by treatment using high dose A. vera (Conc. Aloe Powder) for 4 weeks, a trend of decline of lead concentration was observed in the blood. Adding pectin to A. vera gave no additional benefits (Figure 2B).
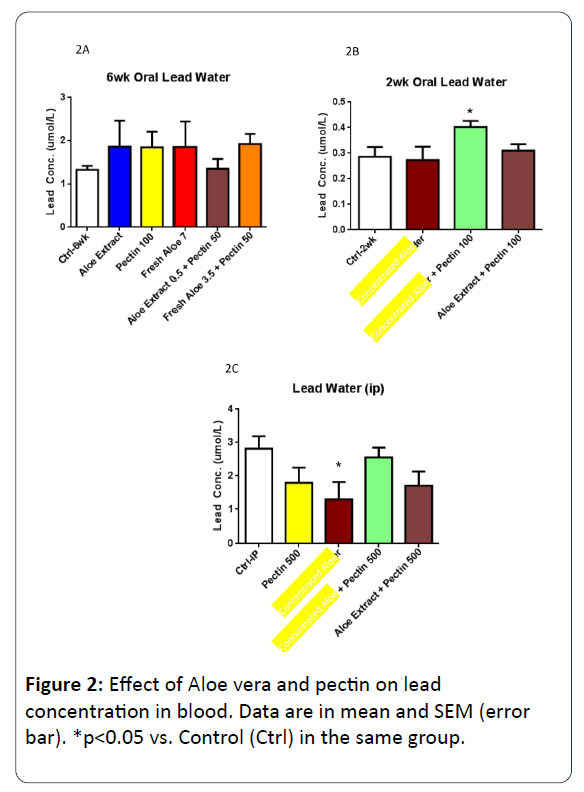
Figure 2: Effect of Aloe vera and pectin on lead concentration in blood. Data are in mean and SEM (error bar). *p<0.05 vs. Control (Ctrl) in the same group.
In the case of acute lead toxication (intraperitoneal high dose), after treatment with high dose A. vera (Conc. Aloe Powder) or pectin, a trend of lead concentration decline was observed. However adding pectin to A. vera gave no additional benefits (Figure 2C).
Effect of A. vera and pectin on lead concentration in Liver: Administration of all A. vera samples or pectin did not reduce the retention of lead in the liver after 6 weeks of prolonged feeding with lead water (Figure 3A). However when lead water feeding continued for only 2 weeks, high dose of aloe as well as combined with high dose pectin, were seen to be effectively lowering the lead concentration (Figure 3B). High dose aloe gave a 44.0% reduction (p=0.042) compared with control. In the case of acute lead toxication, high dose aloe alone gave a 57.3% reduction compared with control (Figure 3C).
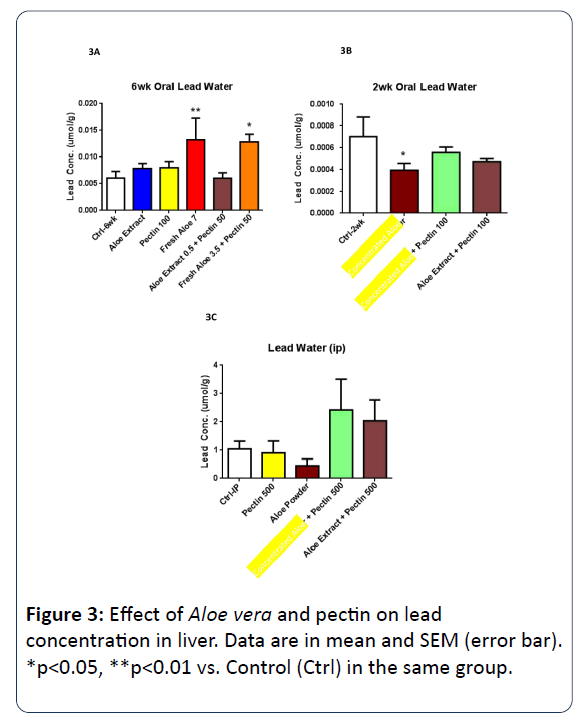
Figure 3: Effect of Aloe vera and pectin on lead concentration in liver. Data are in mean and SEM (error bar). *p<0.05, **p<0.01 vs. Control (Ctrl) in the same group.
Effect of A. vera and pectin on lead concentration in Kidney: 6-weeks’ administration of lead water increased the lead concentration in kidney significantly and in spite of any form of treatment, no decline was observed compared with the control (Figure 4A). After 2 weeks of lead water feeding, high dose of aloe showed a slight trend of decline in lead concentration (Figure 4B). Combination administration of aloe with pectin had no beneficial effects. In the case of acute lead toxication, however, aloe powder alone reduced the lead content by 59.1% (p=0.032) in the kidney in high concentration (Figure 4C).
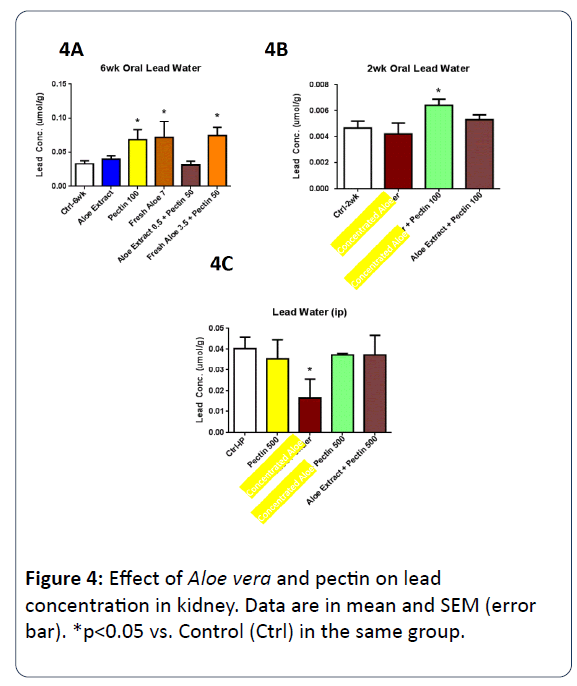
Figure 4: Effect of Aloe vera and pectin on lead concentration in kidney. Data are in mean and SEM (error bar). *p<0.05 vs. Control (Ctrl) in the same group.
Effect of A. vera and pectin on lead concentration in Bone (femur): Most disappointing results were observed in bone tissues. Similar to the observation in kidney, none of the treatment agents showed influence on the lead contents of bone when the lead water feeding was lasted for 6 weeks (Figure 5A). Only a slight decline trend was found when the high dose of aloe was given for the rats received 2-week lead water feeding (Figure 5B). In the situation of acute toxication, only high dose of aloe showed a slight trend of reduction (Figure 5C).
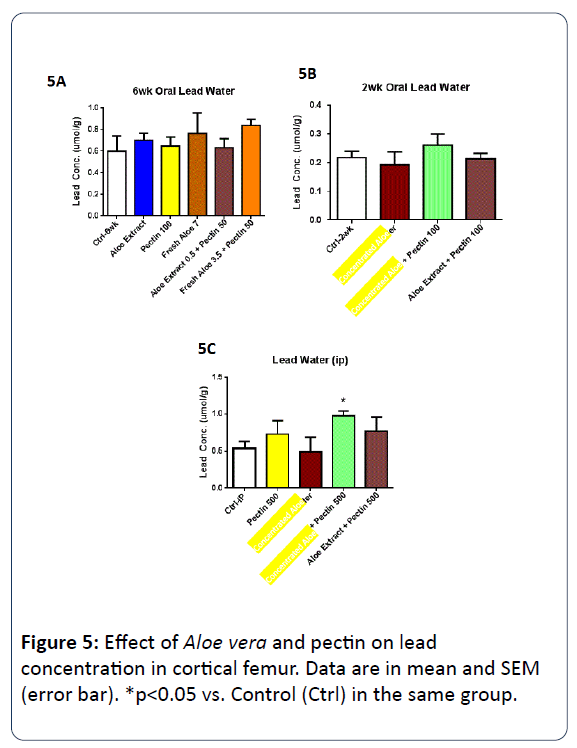
Figure 5: Effect of Aloe vera and pectin on lead concentration in cortical femur. Data are in mean and SEM (error bar). *p<0.05 vs. Control (Ctrl) in the same group.
Discussion
The current study revealed that the pathway and duration of the lead toxication affect the distribution of lead to be accumulated in different tissues. Among the three tissues being analyzed in this study, bone is the one with the highest retention of lead in the animals receiving long term lead toxication orally, whereas liver was the tissue with the lowest lead concentration under this pathway. On the other hand, liver contained the highest concentration of lead among the three tissues when high dose acute lead toxication was induced intraperitoneally. The results also showed that the blood lead concentration increased significantly after the lead toxications. This is similar to one report which stated that blood is the main body compartment that stores lead [14,15]. The results of our study also indicated that lead, once introduced into the body, was difficult to be removed. The lead concentration in blood and tissues of the rats remained at high levels after 4 weeks even though the animal had received only a single dose of lead water intraperitoneally. In fact, the halflife of lead contamination measurable in blood, soft tissues and bone could be in terms of weeks, months or years respectively [15]. In our study, the accumulation of lead in blood and tissues of the rats was much higher among the rats which received 6-weeks oral lead water compared with those receiving only 2-weeks. This reflected well that accumulation was real.
Rats fed with fresh aloe or commercial aloe extract powder did not show decrease in lead contents in blood or organ tissues. However, when the highly concentrated aloe powder (20 times higher than the fresh aloe pulp) was fed, a clear trend of decrease in lead contents was shown in blood and organ tissues.
In spite of many reported data, the lead removal ability of pectin could not be verified in this study. Although, pectin in high concentration (500 mg/kg) could reduce the lead concentration insignificantly in blood of the rats under acute lead toxication. The commercial product or pectin we got provided no information about its quality. The probability of quality defects and contaminations could be the causes of the negative observations. The ability of pectin on lead removal is determined by its esterification [9,10]. Only low esterified pectin was recommended for lead removal. Since the percentage of esterification of our pectin was unknown, we would refrain from further comments on pectin until we get further information or repeat the tests with other favourable choices.
At the start of this study, we assumed that pectin, according to scientific reports, could be the main agent promoting the control of lead contents in blood and organs. Hence if A. vera has the same ability, whether related to pectin or not, it may also enhance the pectin effects. To our disappointment the combination of pectin and aloe failed to demonstrate additional effects. We look forward to further explorations using different supplies of pectin in better arranged experimental protocols.
Conclusion
Lead contamination in drinking water could be regular environmental hazards resulting from illegal industrial dumpings, lead paints and solderings [16]. Although people affected seldom reach the toxic level that requires proper chelating therapy, it has been observed that even the minimal amount of lead absorbed would be accumulative and whether total excretion is possible remains obscure [17]. For those who are known to have lead in their blood, and those who have consumed lead contaminated water or food, although specific treatment is unnecessary, it would be a great blessing if some specific health supplement could be offered, to help eliminating the lead contents, slowly, and effectively.
With this aspiration in mind, we believe that our research on A. vera and pectin, has given sufficient encouragements for us to give more efforts on the development of the supplement [18].
Acknowledgements
Our research team would like to acknowledge Kam Hing Group for their generous financial support and supply of fresh Aloe vera. We would also thank the University Pathology Service, CUHK for their help in the analysis of the lead content in blood and tissues.
Funding
Starting grant as obtained from the Kam Hing Food Factory, Hong Kong.
References
- Paoliello MM, Capitani D (2005) EM Environmental contamination and human exposure to lead in Brazil. Rev Environ Contam Toxicol 184: 59-96.
- Chisolm JJ (2000) Safety and efficacy of meso-2,3-dimercaptosuccinic acid (DMSA) in children with elevated blood lead concentrations. J Toxicol Clin Toxicol 38: 365-375.
- Kosnett MJ (2010) Chelation for heavy metals (arsenic, lead, and mercury): protective or perilous? Clin Pharmacol Ther 88: 412-415.
- Dietrich KN, Ware JH, Salganik M, Radcliffe J, Rogan WJ, et al. (2004) Treatment of Lead-Exposed Children Clinical Trial Group. Effect of chelation therapy on the neuropsychological and behavioral development of lead-exposed children after school entry. Pediatrics 114: 19-26.
- Centers for Disease Control and Prevention (CDC) (2006) Deaths associated with hypocalcemia from chelation therapy--Texas, Pennsylvania, and Oregon, 2003-2005. MMWR Morb Mortal Wkly Rep 55: 204-207.
- Flora G, Gupta D, Tiwari A (2012) Toxicity of lead: A review with recent updates. Interdiscip Toxicol 5: 47-58.
- Margaret E (2013) Sears Chelation: Harnessing and Enhancing Heavy Metal Detoxification-A Review. Sci World J.
- Khotimchenko M, Kovalev V, Khotimchenko Y (2007) Equilibrium studies of sorption of lead(II) ions by different pectin compounds. J Hazard Mater 149: 693-699.
- Serguschenko I, Kolenchenko E, Khotimchenko M (2007) Low esterified pectin accelerates removal of lead ions in rats. Nutr Res 27: 633-639.
- El-Nahal DM (2010) Effect of using pectin on lead toxicity. J Am Sci 6: 541-554.
- Minamisawa M, Minamisawa H, Yoshida S, Takai N (2004) Adsorption behavior of heavy metals on biomaterials. J Agr Food Chem 52: 5606-5611.
- Malik R, Lata S, Singhal S (2015) Removal of heavy metal from waste water by the use of modified Aloe vera leaf powder. Int J Basic Appl Chem Sci 5: 6-17.
- Reinholz MM, Bertics PJ, Miletic V (1999) Chronic exposure to lead acetate affects the development of protein kinase C activity and the distribution of the PKCgamma isozyme in the rat hippocampus. Neurotoxicology 20: 609-617.
- Masci O, Bongarzone R (1995) Toxicity of lead. In: Castellino N, Castellino P, Sannolo N (eds.) Inorganic Lead Exposure: Metabolism and Toxication. Lewis, Boca Raton, FL pp: 203-213.
- Karri SK, Saper RB, Kales SN (2008) Lead encephalopathy due to traditional medicines. Curr Drug Saf 3: 54-59.
- Wan SHM (2016) Editoral: The lead in water epidemic: the oft neglected issue of workers’ health. Occupational Health.
- Centers for Disease Control and Prevention (CDC) (2015) Eductaional intervention for Children affected by lead. Atlanta. US Deparment of Health and Human Services.
- https://www.who.int/ceh/publications/leadguidance.pdf