Keywords
Electronic health records; EHR systems; EPIC; Health information technology; Meaningful use; Texas medical center
Introduction
Health information technology (HIT) has become fundamental to healthcare improvement and will be a primary strategy for enriching its quality, enhancing patient management, extending/expanding research, and evolving capabilities in healthcare delivery [1-4]. Research has identified more effective HIT as the key to closing quality and safety gaps in the healthcare system [3,5]. Thus, the U.S. federal government has enacted legislation to promote health providers’ and medical practitioners’ “meaningful use” of electronic health record (EHR) systems, with the federal government providing funding incentives for compliance with the “meaningful criteria” [2,6-8]. The federal and state governments have also enacted legislation and regulatory mandates and penalties for not embracing EHRs that are certified “meaningful data producers” [9]. This is because the traditional or legacy EHR was developed strictly as a document storage, management, and retrieval system for provision of clinical care. It was not designed for front-end-to-back-end seamless data extraction, subsequent analyses, or virtually real-time reporting [2,10-13]. Also, legacy EHRs permitted unstandardized and disjointed entries, thereby producing variation in content. Furthermore, this resulted in clinical data housed in multiple disconnected systems, further restraining efficient and meaningful EHR analyses [14].
On-the-spot, commercial EHR systems are increasingly being adopted because of their certified off-the-shelf and instantaneous potential to produce the “meaningful data” required to qualify for financial incentives or avoid penalties for non-compliance [1,3]. Also, it is only common sense for large-scale patient care delivery and academic research systems to acquire the latest technological advances as the industry in general shifts to pursue the power that meaningful data-producing EHRs possess [1,6]. For many small and medium-sized hospitals and healthcare systems, this translated into one vendor, EPIC®, which in the past had widespread adoption among small and medium-sized markets [1,15] and where EPIC “cut its teeth.” EPIC products are not only certified to produce meaningful use data but they also leverage an incredibly powerful electronic connectivity, thereby permitting more rapid and thorough data transfers, expansions, and extensions from and to other EPIC-based systems, as well as more efficient and rigorous data analyses [1].
EPIC previously had held a constant yet commanding EHR market share with approximately a 20% share of the EHR market [16-19]. EPIC is one of the “Big 8” meaningful use EHRs—that offer some similar features as EPIC®. The percentage of academic institutions using EPIC is unknown but is estimated to be substantial and growing [20]. Nevertheless EPIC® is now poised to extend its market reach to large-scale and global hospital/healthcare systems, medical research institutions, and elsewhere. For example, five out of six research hospitals and medical facilities in the world’s largest medical center, the Texas Medical Center in Houston, are adopting EPIC as their EHR system in 2016 [20]. With this and other recent coups, though recent unconfirmed estimates are contentious, it appears EPIC may capture more than 25% of the EHR market share, potentially shifting control of future markets and even other systems its way. Due to its rapid market penetration, EPIC® now exercises vast potential control of healthcare itself through decision support rules, order sets, visualizations, quality measurement, and coordination and control of workflow. This is not nefarious but the reality of substantial software shaping workflow, data, standards, and definitions.
Therefore, it is worth taking a long and hard look at EPIC regarding its benefits and drawbacks in terms of meaningful use through a systematic review of the literature, including standardized data collection, technological somnambulism, time commitments and productivity, real-time data warehousing and (patient-centered) efficient production of outcome measures, enhanced patient safety, patient tracking and follow-up, enduser satisfaction, reminders, patient involvement, potential use in medical education, training, issues for research, and practical experience regarding recent implementation in the Texas Medical Center. (Note: There are other systems similar to EPIC and better or worse; however, this article is not a comparative analysis. Rather, given its recent market ascendency this article’s focus is on what is known about EPIC® in the literature and the positive or negative aspects described are probably not unique only to EPIC).
Method
The findings in this article derive from a systematic, iterative literature review on EPIC that is depicted in Figure 1.
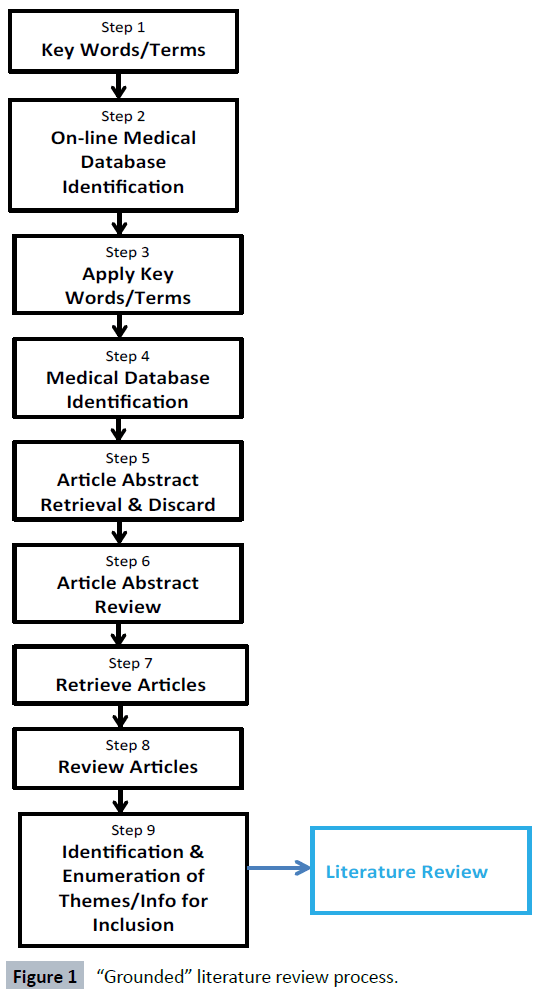
Figure 1: “Grounded” literature review process.
Figure 1 depicts the evidence-based and best practices literature review research process that informed the work reported herein through which open-source peer-reviewed articles were identified then reviewed and conceptual themes generated.
Essentially, Figure 1 describes the steps in this process. Step one involved deriving relevant keywords with which to search for articles. Step two was targeting appropriate peer-reviewed medical/health and open-source subject matter databases. Step three was applying the search terms to online medical databases. Steps four and five were the identification and retrieval of relevant articles and removal of duplicates. Step six was retrieval and review of abstracts or executive summaries. Step seven was gathering the articles and step eight was reviewing their content for relevance. Step nine was identification and enumeration of themes and the retrieval of related information for review until all themes were exhausted with the outcome, and step ten was the review. Given that the process is “theoretically grounded” [21], though the steps are generally sequential and linear, they can be repeated individually or the researcher can cycle back and forth between steps or back through the process. However, the eventual and ultimate aim was the identification, summation, and exhaustion of all themes. The one limitation in this method is that not all possible themes in the universe may have been identified. However, this does not suggest that those identified herein are any less important or meaningful.
Findings
Standardized data collection
EPIC’s potential for improving healthcare lies in its ability to connect information and retrieve standardized data for comparative analysis and because it requires pre-determined data outcome measurements [2,3,11,14,15,22,23]. Grigoryan et al. [24] found EPIC’s Clarity module was essential in terms of identifying low compliance with current medical best practices and misuse of medications that could prove deadly. Specifically, EPIC was able to generate accurate (and timely) reports based on requirements for entry of standardized data codes (e.g., EPIC “hard stops”), in this case diagnosis codes [2,3,23]. These codes can be immediately queried for programmatic evaluation and modification research. However, Koppel and Lehman’s work [15] cautiously insinuates that a disadvantage of monopoly or market dominance and a monoculture is that it maintains antiquated programming and retard responsiveness, de-confliction, flexibility, enhancement, and the ability to evolve. Also, this state of affairs locks purchasers into EPIC® such that any disruption of that unitary system will result in disturbances in nascent data flows, data format standards, and user interface templates [15].
Carberry et al. [3] revealed that incorporating patient-centered standardized measurement tools at the medical condition level required an iterative collaboration and inter-discipline commitment among clinicians, analysts, and data architects, which the EPIC system fostered [25]. They cautioned that this process can be resource and time intensive and risked wasteful duplication of efforts, but the end-product was well worth the trouble. Lindholm et al. [26] found a statistically significant (p<007) difference in that EPIC produced 78% greater identification of potential candidates for tobacco cessation. This was because EPIC allows for modification/inclusion of evidence-based prompts and hard stops for identifying and mandating standardized data entry. Likewise, Katzan et al. [2] noted that EPIC provides “…the additional software layers for easy access to (standardized) clinical information and serves as an accessible, evaluable platform for collecting and analyzing clinical outcomes….” This team noted that EPIC can be conformed to shepherd data entry and pre-identify errors and error patterns at the moment clinicians enter data. Thus, data points can be identified and evaluated virtually in real time, almost immediately enhancing accuracy and quality of data as well as informing medical service adjustments [2,22,23,27-29]. Also, it should be noted that EPIC® improves healthcare by providing high-quality, integrated standardized documentation for ordering medications, therapies, and procedures. Data analytics though important are a secondary outcome of this precision and not the primary reason for its implementation.
One challenge Bornstein [13,14] reported was that when Kaiser-Permanente (KP) transitioned from a ‘legacy document management system’ to EPIC, KP found EPIC ill-suited for backloading data and information in the standard format, which resulted in multiple and expensive remediation efforts. Backloading continued to be a chronic and long-term problem resulting in maintenance and the attendant expense of supporting several different systems that EPIC was supposed to eliminate in the first place. Conversely, Borstein [14] observed that EPIC was easily able to capitalize on its standardized real-time workplace data entry of medical-condition-service-for-fee codes to identify patterns and practices. It permitted non-intrusive, accurate, and virtually realtime identification for analyses that could continuously operate unnoticed in the background [2,22-24,30].
DeBoer et al. [11] were able to leverage EPIC’s standardized data-ready feature to track medical procedures and substantially reduce unplanned outcomes. Also, Sweet et al. [31] used EPIC’s standardized data infrastructure to facilitate genetic counselling for multiple complex diseases and pharmacogenetics as well as clinically based decision support. Bain [13] validated the fact that EPIC’s front-end-back-end standardized data entry and query and data report generator eliminated the expensive, repetitive loading of data into multiple different systems. The old process was a by-product of traditional e-document management systems. The latter process involved by-hand data transfer and was prone to error and duplication of effort by simple virtue of additional and unnecessary steps [2].
Technological somnambulism
Along with hard-stop-enabled standardized data entry come its downside, namely, risk for reflexive and non-reflective technologydriven hypnosis and even sleepwalking [32-36]. Carberry et al. [3] highlight an issue surrounding EPIC that is inherent in all EHRs with “meaningful use” capabilities. Specifically, frontend data collection is shepherded, entailing over-reliance on pre-determined existing (“canned’) forms and templates for information collection—as opposed to producing meaningful data. This can be further complicated by polished and slick-veneer electronic systems. Carberry et al. [3] found that meaningful measurement had to be identified by an outcome measurement team that worked with dedicated vendor-trained analysts. This team’s mission was to build sophisticated customized forms and templates relevant to particular organizations and their missions and designed to capture information throughout the medical care cycle [25].
In this regard, EPIC’s drawback is that it does not permit entering more specific or different information [2], except through the incorporation of add-ons that detract from its overall efficiency. In support of this contention, Makam et al. [1,37] found that with the introduction of EPIC, little extemporaneous dictation exceeded the standardized templates or pre-populated phrases. Interestingly, this team also observed a curved-linear and statistically significant relationship between use of standardized data entry and years after graduation from medical school. Specifically, they found a linear correlation between use of standardized data entry that maxed at 14 years post-medical school graduation and then decreased exponentially. They suggested that this finding might also point to a relationship between familiarity with the technology and the advent of the more recent tech-savvy (i.e., Nintendo) generation that grew up with the technology and take it for granted almost unquestioningly.
Time commitments and productivity
Several issues are incumbent with all “meaningful use” EHRs that turn clinicians into data entry clerks. One is the additional time commitment of entering data loaded onto the already timeintensive commitments of clinical practice [1,13,14,37]. EPIC seems to be no different. Hammoud et al. [32,36] reported that medical students spent a substantial amount of time entering data into EPIC—more so than physicians—and this was a possible distraction from their medical studies. Bornstein [1,14] noted that added documentation in EPIC also added burden on physicians. However, the resulting seamless data analysis was well worth the effort from the physicians’ perspective. Makam et al. [1] also noted a substantial “after hours’ time tax” to enter information and there may not be time-savings over paper charts in terms of clinical visits. They found that on average 43% of clinicians reported an additional 1-3 h spent on EPIC data entry or about 45 minutes for every hour of medical practice. Yet in a case-controlled study conducted by Barnett, Mehorta, Jena, and Newhouse [38] found, despite clinical staff additional time commitments to entry into EHRs, especially EPIC®, there was not adverse effect on patient care.
Carberry et al. [3] observed the aspect of EPIC that makes it truly desirable for outcomes measurement, program evaluation, and research, specifically, its hard stops. However, this also is a severe detraction or Achilles’ heel in that they disrupt smooth work flow and also result in end-use dissatisfaction [14,33]. Nevertheless, Cheriff et al. [13,37] reported that medical providers’ productivity work volume, charges, and work relative to volume units actually increased with EPIC. The caveat was that it took several months of EPIC experience to realize increased productivity. The authors’ ultimate conclusion was that worker apprehension about EPIC adoption due to lost productivity was grossly unfounded and counterproductive.
Real-time data warehousing and (patient-centered) efficient production of outcome measures
EPIC excels when it comes to generating reasonably accurate (and extremely timely) outcome measures, which is the essence of “meaningful use” [1,3,11,13,22-24,30,38-42]. Goldberg et al. [1,11,13,14,39,41,43] found that EPIC was responsible for a dramatic decrease in multi-center decision support systems and time-to-decision. Heidemann et al. [30,37-40] showed that physician use of data output substantially and geometrically improved accurate identification of drug-induced liver disease. However, this was not possible without an add-on program that helped analyze the raw data that the back-end of EPIC produced [30,41].
Bellon et al. [8,14,22] found that EPIC’s patient-centered My Chart data reports feature provided sufficiently accurate data to make evaluation comparisons on prescription practices on which to base policy decisions. My Chart also provides patients with summary medical information on their case in real time. Unni et al. [34] reported that EPIC’s FRAX analysis tool underestimated osteoporosis risk factors and that it underestimated an average 10 years probability of any major risk factors. This was the result of EPIC only supporting passive data collection in terms of risk factors [3]. This study called into disrepute EPIC’s independent ability to collect relevant outcome data. Nevertheless, Steidl and Zimmerman [43] concluded that the disciplined use of EPIC’s electronic medical record (EMR) template was vital to extracting accurate key outcome measures in that data extraction improved pre-post-EPIC 53.3% to 91%, respectively, and accuracy was nearly 100%. They deduced that EPIC was the ideal front-end-toback- end interface between required documentation and clinical research. EPIC far exceeded (non-meaningful) traditional paper and electronic records management systems [14].
Enhanced patient safety
EPIC’s ability to quickly and accurately derive outcome measures is critical in terms of efficient and timely identification of potentially deadly patient hazards and targeting those patients for intervention [23,30,39,42-46]. Flatow et al. argued that EPIC was significantly related to identification of Central Line- Associated Bloodstream Infection rates and preventive reduction of Surgical Intensive Care Unit mortality. Sonstein, Clark et al. [46] reported that the implementation of EPIC resulted in improved adherence to steroid prescription guidelines and best practices for Chronic Obstructive Pulmonary Disease patients and subsequent statistically significant reduction in the dose of corticosteroids administered. Kullar et al. [42] reported EPIC’s potential to reduce emergent antibiotic resistant bacteria through real-time data-driven decision feedback, which was invaluable for improving patient safety.
Similarly, Adelson et al. [45] conducted an evaluation study of EPIC’s BEACON electronic performance ordering platform in terms of measuring evidence-based practices. This study revealed that the rate of evidence adherence was 86% and statistically significant and patient satisfaction surrounding this EPIC feature was 80%. This study concluded that EPIC was a powerful tool to monitor adherence to prescribing best practices, but only with vendor support and rather expensive add-ons with which to conduct analyses and a lot of hard stops interfering with workflows [3,30,33,41]. Likewise, Beck et al. [23] demonstrated the power of EPIC regarding establishing incidence, namely, scapholonate disassociation, in patients with gouty athropathy. However, more importantly, they also reported identification for further subclinical and unidentified disease progression over time.
Patient tracking and follow-up
EPIC’s ability to accurately derive and report information in almost real time to identify patient safety risks also lends itself to excellent patient tracking, monitoring, and follow-up [1,2,11,41]. DeBoer et al. [11] demonstrated that EPIC was an excellent system for electronically tracking patients and their bronchoscopy procedures and documenting complications, risks, and sources of unplanned outcomes. Similarly, Brenn et al. [41] revealed that EPIC provided an excellent data recording system for conducting an inexpensive, continuous four-year longitudinal satisfaction survey for patients of pediatric hospital anesthesia services. Also, it permitted easy aggregation by type and level of complications. However, this was only possible by first feeding EPIC raw data into an expensive add-on program for data analyses.
End-user satisfaction
End-user satisfaction is one area where EPIC scores mediocre or evens a low or failing grade. Makam et al. [1,14] found in a study of primary care physicians that the average end-user satisfaction with EPIC was 70% but varied between 50% and 75% depending on the particular EPIC feature or function (i.e., problem list). The highest satisfaction rates (75%) were for documenting vaccinations and the lowest (50%) were for cancer screenings. These researchers noted extreme dissatisfaction with and thus less than optimal use of some key EPIC functions. Avoidance of these key features essentially rendered EPIC useless for preventive health improvement and chronic disease management. One reason there was less than optimal use of these particular EPIC features was that end-users felt that data entry for them was inefficient and too time-consuming [3,14,32,33].
Reminders
One key feature that resulted in the most end-user dissatisfaction was EPIC’s “Reminder(s)”; they operate much like its hard stops in that they must be addressed before proceeding with workflow [3,14,32,35] This clearly detracts from EPIC’s usefulness in terms of preventive medicine and patient safety. Borstein [14] found that overburdening and overwhelming medical treatment providers with best practices advisories in large numbers generated scores of complaints. There was marked improvement in provider satisfaction when an arbitrary limit was imposed on alerts and then provider adherence to alerts was checked; if there was adherence, further reminders were withheld. Nevertheless, Langsjoen et al. [33,34] suggested that Reminders significantly improved compliance among providers in terms of ordering Human Papillomavirus testing and verification. This may be why EPIC works better than other EMRs that use passive collection in terms of outcome measures. Additionally, Hayek et al. [33,35] demonstrated that EPIC’s Reminders feature was effective in improving the rates of advance directive documentation and adherence.
Patient involvement
EPIC’s connectivity and ability to electronically transmit realtime medical chart information securely over the Internet has vast potential regarding proactive integration of patients in the management of their own healthcare [1,8,14]. Bornstein [14] reported that EPIC’s MY CHART patient secure messaging feature resulted in physicians shifting their patient management practice to more virtual vs. less face-to-face encounters. However, this feature substantially increased patient involvement in that patients were enabled and empowered to easily and smoothly transfer or upload images and documents from outside sources [1,8]. Bornstein [14] concluded that this particular feature alone would revolutionize reporting of patient information, how healthcare is conducted, and inevitably and eventually “virtualize” all of it. EPIC’s MY CHART features have the potential to revolutionize the way in which medical practitioners and their facilities do their work.
Training
One researcher identified the essential need for ongoing training in terms of transitioning and exploiting EPIC’s potential to its fullest [13,14]. Work with EPIC at KP revealed that maintaining patient service and access during the transition to EPIC was challenging. Therefore, KP chose to reduce patient schedules in lieu of intensive EPIC classroom training, with uniformed on-site vendor technical experts troubleshooting during “go live.” At the time of real patient care using the EPIC system, this was both augmented and attenuated with net-based training and vendortrained expert KP workers cast in an extra capacity as “super users.” KP also changed its focus to train-to-workflow and not train-to-function.
Potential use in medical education
Several researchers have explored EPIC regarding potential for medical residents’ education. Hammoud [36] and Buery-Joyner et al. [1,3,47] noted that medical students used EPIC at higher rates than physicians and 68% of medical school programs had adopted EPIC or EPIC-like systems and allowed their students to dictate into them. They contended that their research suggested EPIC and other EMR systems had vast potential as medical education tools. However, they expressed concern about EPIC’s standardized templates and dictation imposing limits on students’ documenting and dictation and thus degrading their medical education.
An issue for research
One area I which EPIC fails miserably is electronic research consent document management, storage, and retrieval [48]. According to Marsolo et al. [48], EPIC’s system will not allow for different signature lines on a document. EPIC treats documents as distinct entities—so there can only be one signature for one document. This is an aspect of the programming. Thus, this prohibits more than one document being added as “active.” So, a research subject can have only one consent active in the EPIC system. The authors described how EPIC was able to develop a complicated and difficult work-around to the problem which involved manually tracking and cleaning or linking to an external non-EPIC document management, storage, and retrieval system. In such a case, this defeated EPIC’s original purpose, which is to produce meaningful use data through one source and not multiple different and disjointed systems. This also reveals a hidden defect in the EPIC system for conducting research: It prevents an efficient registration process for research in the particularly sensitive area of human research subject protections.
Recent implementation in the Texas medical center
As previously noted, an EPIC-powered EHR system has been implemented to transition from a traditional/legacy EHR at some of the largest, global, public-sector medical treatment and research facilities in the Texas Medical Center and in the world. As part of that implementation, issues surrounding the implementation and solutions were posted on an open-source website for employees’ and others’ benefit. Table 1 and Figure 2 list an inventory of enumerated summaries of issues that arose over the course of the first month of implementation. They provide cursory and preliminary insight into the challenges involved in replacing a long-time legacy system that was developed specifically for this institution and its work in lieu of the more generic EPIC system that produces “meaningful use data.” These analyses were conducted to determine whether EPIC carried-over problems from previous similar implementations.
| Rank |
# of postings |
Description of problem or issue or challenge |
| #1 |
317 |
Changed procedures or more advanced/complicated procedures or new information "workflow" processes and ensuring that staff follows new procedures correctly |
| #2 |
55 |
Understanding the new ways of that information is presented or located in the new system |
| #3 |
49 |
New ways for documenting or creating collection of information or existing information in the system |
| #4 |
23 |
Accessing information or new limitations on access |
| #5 |
7 |
Printers no longer available |
| #6 |
3 |
System crashes or the system "locking-up" due to overloads |
| #7 |
3 |
The new system not fully populating or slowly populating information from the old system |
| #8 |
3 |
Hardstops (requirements for info before proceeding) and imposed system algorithms preventing smooth clinical workflow |
| #9 |
2 |
Longer hold times for the Help desk |
| #10 |
1 |
Plans for transitioning "Help Desk" support once the New System support staff leave after one month on-site support |
Table 1: 1 Month post-epic implementation issues rank ordered.
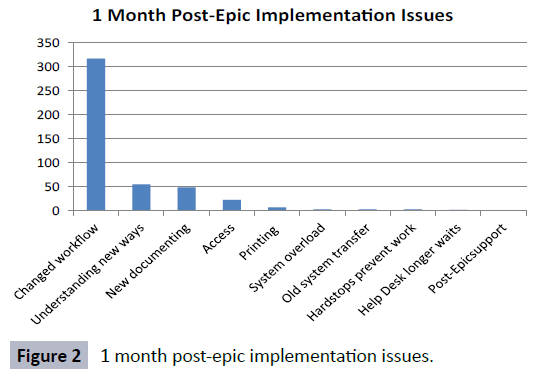
Figure 2: 1 month post-epic implementation issues.
Obviously, the number one issue was changes in procedures that governed clinical work flows in terms of the new EPIC system and corresponding actual medical treatment. Table 1 and Figure 2 reveal that during the transition phase between a legacy and EPIC system, most issues can be resolved with more and better information, training, and greater familiarity with the system. For three months prior to implementation of the EPIC system, EPIC conducted intensive, didactic, and practical training incremented in progressive amounts based on workers’ positions and their anticipated usage of the new system.
Nonetheless, with any new system, there is always a learning curve. Few if any issues mentioned in Table 1 and Figure 2 required software modifications, and none required a major overhaul of the computer program. Note that in all cases the posting had a solution or work-around, whatever the issue, problem, challenge, or barrier, or the matter was being resolved. Also, it would appear that EPIC learned from its previous vetting elsewhere in that few issues that arose earlier at other organizations arose during the TMC “go live” (e.g., hard stops preventing work or old system transfers, too many Reminders). EPIC’s potential for deriving outcome measures and research data is yet to be seen. Overcoming the aforementioned challenges must be the first and most crucial step. Nevertheless, these preliminary findings must be considered not only in terms of the cost-benefit equation of acquisition but also in terms of what must be addressed to transition systems effectively.
Discussion
This paper reported on aspects of EPIC EHR related to its potential to successfully meet criteria for “meaningful use” derived from a systematic, comprehensive review of the medical literature. The review revealed that EPIC provides a rigorous front-endback- end EHR system for the collection and management of inter-connected medical record information that lends itself to routine longitudinal measurement of patient outcome measures and relationships between those measures. Thus, it truly has the potential to enhance and advance the quality and value of patients’ health and medical care. It also has the potential to revolutionize medical practice. Nevertheless, that rigor and accuracy comes at a steep (hidden) price of increased workload on medical practitioners as well as ongoing involvement, coordination, and commitment among cross-functional teams of front-line clinicians, vendor-trained analysts, data system architects, and data specialists. The question posed in the literature was how steep a price is tolerable in terms of the return sought.
Previous researchers’ experience suggests that EPIC provides raw data that can be integrated with analytical system add-ons for further refinement and sophisticated analysis. Vendor support and add-ons also come with hefty price tags. Put differently, as Katzan et al. [2] observed,”… extended software provides much more flexibility than EPIC but cannot replace EPIC’s comprehensive (rigorous and exacting) collection system.” EPIC’s demanding and thorough inter-connected data collection system lends itself to query production that can virtually in real time identify ways to improve medical treatment and risk factors in patients.
Therefore, one of EPIC’s most attractive features is its ability to enhance patient safety and make immediate treatment adjustments, especially through balanced Reminders, hard stops, and tickler systems. Even end-users find these features annoying and disruptive. On the other hand, repeated and ceaseless reminders may be perceived by providers as a distraction, if not outright harassment, and lead to extreme dissatisfaction, frustration, and aggravation by providers who are attending to a myriad of other things. The same might be said of turning healthcare providers into data entry clerks forced to labor away into the wee after-hours traversing and overcoming hard-stop barriers and fill templates satisfactorily to complete their medical record documentation responsibilities on top of substantial clinical practice demands.
However, if used indiscriminately, the benefit of standardized text and pre-designed templates could result in a risk for technological somnambulism, that is, the computer does the leading and driving, not the medical practitioner. Specifically, EPIC favors reliability and consistency and one-click pat answers in canned templates are favored over validity and reality. Thus, there may be a tendency for case reports to eventually reflect little thought and include only information facilitated by EPIC, with no room for discovery or medical insight. Nevertheless, one of the greatest and yet untapped potentials for EPIC’s use is as a teaching tool in medical education. It also has great promise in terms of involving patients in their own medical treatment. As EPIC expands into larger and more research-centric hospital and healthcare systems, its severe limitations in terms of documenting and monitoring human research subject protections are particularly disturbing. The challenge for EPIC in the future will be whether it can overcome the inflexibility of its software to accommodate aspects of research other than just better data collection. These matters constitute avenues of inquiry for future evaluation and research as well as a cross-comparison between EPIC and other similar EHRs on various standards of meaningful use, EPIC’s potential to advance medical education and patient involvement, and how it can be adapted and developed for non-healthcare records information management. A hard stop is a prompt that will not allow an operation to proceed without entering particular data in a standard and correct format.
Declarations
Conflicting interests
None declared.
Funding
N/A.
Ethical approval
N/A, this was a review of open-source documents and analyses of anonymous publically available data.
Guarantor
Ralph J. Johnson.
Contributor-ship
Ralph J. Johnson.
Acknowledgements
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
- Makam AN, Lanham HJ, Batchelor K, Samal L (2013) Use and satisfaction with key functions of a common commercial electronic health record: a survey of primary care providers. BMC Med Inform Decision Making 13: 86.
- Katzan I, Speck M, Dopler C, Urchek J (2011) The knowledge program: an innovative, comprehensive, electronic capture system and warehouse. AMIA Ann Symp Proc 2011: 683-692.
- Carberry K, Landman, Z, Xie M, Feeley T (2016) Incorporating longitudinal pediatric-centered outcome measurement into the clinical workflow using a commercial electronic health record: a step toward increasing value for the patient. J Am Med Inform Ass 23: 88-93.
- Porter ME and Teisberg E (2006) Redefining health care. Boston, MA: Harvard Business Publishing 97-148.
- Tierney WM (2001) Improving clinical decisions and outcomes with information: a review. Int J Med Inform 62: 1-9.
- Blumenthal D, Tavenner M (2010) The “meaningful use” regulation for electronic health records. N Engl J Med 363: 501-504.
- Services CfMM. EHR Incentive Program [online].
- Gerber DE, Lacetti AL, Beibei C, Jingsheng Y (2014) Predictors and intensity of online access to electronic medical records among patients with cancer. Journal of Oncology Practice pp: e307-e312.
- Ferris N (2010) “Meaningful Use” of electronic health records. Health Aff.
- Prokosch HU, Ganslandt T (2009) Perspectives for medical informatics. Reusing the electronic medical record for clinical research. Methods Inf Med 48: 38-44.
- DeBoer EM, Prager JD, Kerby GS, Stillwell PC (2016) Measuring pediatric bronchoscopy outcomes using Electronic Medical Record. Ann Am Thorac Soc 13: 678-683.
- Flatow VH, Ibragimova N, Divino CM, Eshak DS (2015) Quality outcomes in the surgical intensive care unit after electronic health record implementation. Appl Clin Inform 7: 611-618.
- Bain PA (2008) Collaboration saves time. WMJ 107: 380-381.
- Bornstein S (2012) An integrated EHR at Northern California kaiser-permanente. App Clin Inform 3: 318-325.
- Koppel R, Lehmann CU (2015) Implications of an emerging EHR monoculture for hospitals and healthcare systems. Am Med Inform Assoc 22: 465-71.
- https://www.darkdaily.com/wp-content/uploads/ehr-vendors.jpg
- https://www.darkdaily.com/wp-content/uploads/EHR-systems-by-vendor.jpg
- https://www.emrandehr.com/wp-content/uploads/2014/05/Table-IX-40-Plus-Practioners.gif
- https://wac.1a76d.edgecastcdn.net/801A76D/analytics/images/site/attachments/Care_coordination.png
- https://www.epic.com/CareEverywhere/
- Strauss A and Corbin J (1998) Basics of qualitative research – techniques and procedures for developing grounded theory (2nd edn.) London, Sage Publications.
- Bellon JE, Stevans JM, Cohen SM, James AE (2015) Comparing advanced practice providers and physicians as providers of e-visits. Telemed J E Health 21: 1019-1026.
- Beck JD, Deegan JH, Riehl JT, Klena JC (2010) Incidence of scapholunate ligament dissociation in patients with aspiration-confirmed gout. J Hand Surg Am 35: 1938-1942.
- Grigoryan L, Zaroob R, Wang H, Trautner BW (2015) Low concordance with guidelines for treatment of acute cystitis in primary care. Open Forum Infect Dis 26: 4.
- Klehr J, Hafner J, Spelz LM, Steen S (2009) Implementation of standardized nomenclature in the electronic medical record. Int J Nurs Terminol Classif 20: 169-180.
- Lindholm C, Adsit R, Bain P, Reber PM, Smith SS, et al. (2010) A demonstration project for using the electronic health record to identify and treat tobacco users. WMJ 109: 335-340.
- Schleelein L, Vincent AM, Jawad AF, Pruitt EY (2016) Pediatric perioperative adverse events requiring rapid response: a retrospective case-control study. Ped Anesth 26: 734-741.
- Onuha OC, Hatch MB, Miano TA, Fleisher LA (2015) The incidence of un-indicated preoperative testing in tertiary academic ambulatory center: a retrospective cohort study. Periop Med 4: 14.
- Krasowski MD, Wilford JD, Howard W, Dane SK (2016) Implimentation of epic beaker clinical pathology at an academic medical center. J Pathol Inform 7: 7.
- Heidemann L, Law J, Fontana RJ (2015) A text searching tool to identify patients with idiosyncratic drug-induced liver Injury. Dig Dis Sci pp: 1-11.
- Sweet K, Gordon ES, Sturm AC, Schmidlen T (2014) Design and implementation of a randomized controlled trial of genomic counseling for patients with chronic disease. J Pers Med 4: 1-19.
- Chi J, Kugler J, Chu IM, Loftus PD (2014) Medical students and the electronic health record: an epic use of time. Am J Med 127: 891-895.
- Langsjoen J, Goodell C, Castro E, Thomas J (2015) Improving compliance with cervical cancer screening guidelines. Proc (Bayl Univ Med Cent) 28: 450-453.
- Unni S, Yao Y, Milne N, Gunning K, Curtis JR, LaFleur J, et al. (2015) An evaluation of clinical risk factors for estimating fracture risk in postmenopausal osteoporosis using an electronic medical record database. Osteoporos Int 26: 581-587.
- Hayek S, Nieva R, Corrigan F, Zhou A, Massoomi M, et al. (2014) End-of-life care planning: improving documentation of advance directives in the outpatient clinic using electronic medical records. J Palliat Med 17: 1348-1352.
- Hammoud MM, Margo K, Christner JG, Fisher J, Fischer SH, et al. (2012) Opportunities and challenges in integrating electronic health records into undergraduate medical education: a national survey of clerkship directors. Teach Learn Med 24: 219-224.
- Cheriff AD, Kapur AG, Qiu M, Cole CL (2010) Physician productivity and the ambulatory EHR in a large academic multi-specialty physician group. Int J Med Inform 79: 492-500.
- Barnett ML, Mehrota A, Jena AV, Newhouse RL (2016) Adverse inpatient outcomes during the transition to a new electronic health record system: observational study. BMJ 354: 1-5.
- Goldberg HS, Paterno MD, Grundmeier RW, Rocha BH (2016) Use of a remote clinical decision support service for a multicenter trial to implement prediction rules for children with minor blunt head trauma. Int J Med Inform 87: 101-110.
- Han JE, Rabinovich M, Abraham P, Satyanarayana P, Liao TV, et al. (2016) Effect of Electronic Health Record Implementation in Critical Care on Survival and Medication Errors. Am J Med Sci 351: 576-581.
- Brenn BR, Choudhry DK, Sacks K (2016) Outpatient outcomes and satisfaction in pediatric population: data from the postoperative phone call. Paediatr Anaesth 26: 158-163.
- Kullar R, Goff DA, Schulz LT, Fox BC, Rose WE (2013) The "epic" challenge of optimizing antimicrobial stewardship: the role of electronic medical records and technology. Clin Infect Dis 57: 1005-1013.
- Steidl M, Zimmern P (2013) Data for free can an electronic medical record provide outcome data for incontinence/prolapse repair procedures? J Urol 189: 194-199.
- Chima CS, Farmer-Dziak N, Cardwell P (2005) Use of technology to track program outcomes in a diabetes self-management program. J Am Diet Assoc 105: 1933-1938.
- Adelson KB, Qiu YC, Evangelista M, Spencer-Cisek P, Whipple C, et al. (2014) Implementation of electronic chemotherapy ordering: an opportunity to improve evidence-based oncology care. J Oncol Pract 10: e113-e119.
- Sonstein L, Clark C, Seidensticker S, Zeng L, Sharma G (2014) Improving adherence for management of acute exacerbation of chronic obstructive pulmonary disease. Am J Med 127: 1097-1104.
- Buery-Joyner SD, Dalrymple JL, Abbott JF, Craig LB, Wolf A, et al. (2015) Overcoming electronic medical record challenges on the obstetrics and gynecology clerkship. Obstet Gynecol 126: 553-558.
- Marsolo K, Corsmo J, Barnes MG, Pollick C, Ganta R, et al. (2012) Challenges in creating an opt-in biobank with a registrar-based consent process and a commercial EHR. J Am Med Inform Assoc 19: 1115-1118.

