Keywords
3D Pharming; Pharmaceutical tablets; 3D Printing
Abbreviations
4-ASA: 4-Aminosalicylic Acid; 5-ASA: 5-Aminosalicylic Acid; CAD: Computer-Aided Design; CJP: Continuous Jet Printing; DSC: Differential Scanning calorqimetry; DOD: Drop On Demand; EGDT: Ethylene Glycoldithiol; Fast Disintegrating/Dissolving Tablet; FDT: FDM: Fused Deposition Modelling; GI: Gastrointestinal; HME: Hot Melt Extrusion; HPMC: Hydroxypropyl Methylcellulose; IBD: Inflammatory Bowel Disease; PETMP: Pentaerythritol Tetrakis (3-mecaptopropionate); PCL: Polycaprolactone; PDMS: Polydimethylsiloxane; PEO: Polyethylene Oxide; PLA: Polylactic Acid; PVA: Polyvinyl Alcohol; USFDA: U.S. Food and Drug Administration; USP: United States Pharmacopeia; XRPD: X-Ray Powder Diffraction
Introduction
Currently, the ten top-grossing drugs in the United States effectively benefit only 4 to 25 percent of the patients that take them [1]. For instance, some drugs have been proven to have higher efficiencies in people with certain genetic variations, while others have been proven harmful to particular ethnic groups [2,3]. More specifically, a person diagnosed with cancer back in 2004 might have received a treatment only effective on ten percent of the population and caused significant side effects. Advances in the field of Pharmacogenomics, the study of how the genetic makeup of a person affects their particular drug response, are providing more precise information about the dosage and choice of drug that would best benefit a specific individual based on their genetic makeup [4,5]. In contrast nowadays, a biopsy tissue of that person could be genetically screened, predicting which treatment would more reliably treat the pathological condition [6].
Personalized medicine aims to provide patients with treatments tailored to their pathophysiology. This is done by coupling a patient’s pharmacogenomics with information about their diet, environment, lifestyle, microbiome, and epigenetics [7]. This new approach for prescription drugs requires technology capable of producing tablets with a variety of dosage strengths in order to satisfy the specific medical needs of each individual. Currently, pharmaceutical companies manufacture tablets with universal predetermined dosage amounts [8]. This method requires large facilities with high production costs, trained personnel for its operation, and involves a variety of processing steps [9]. To make personalized medicine a reality, a paradigm shift in the way oral drug forms are currently manufactured is required. The new strategy should have the ability to reproducibly generate a wide range of dosages and have a short manufacturing time. These features would allow tablet manufacture technology to adapt to the rapid changeover of formulations experienced by scientists within R&D and clinical trial studies, accelerating drug development. Additionally, it should be economically viable, have minimal space and operational training requirements, comply with standards of regulation agencies, and able to be digitally controlled by healthcare staff [10]. 3D printing was first demonstrated in 1996 as a promising candidate to replace conventional tableting techniques [11]. In 2015, the U.S. Food and Drug Administration agency (FDA) granted the approval of Spritam® (levetiracetam), the first 3D printed tablet for the treatment of epileptic seizures [12]. This landmark event marks a milestone in 3D Pharming and motivates further development of this technology towards the fabrication of customized tablets and improved personalized medicine. 3D Pharming promises to enable rapid point-of-care formulations with patient-specific dosages [13]. Furthermore, 3D Pharming provides control over drug release kinetics through methods that precisely manipulate the spatial distribution of multiple drugs within a pill, as well as their diffusion gradients [14]. This potential reduction in the number of tablets prescribed, combined with their improved efficacy, could result in enhanced patient compliance [15]. Finally, the economic benefits of this technology include reduced manufacturing and inventory wastes and the potential to grow to an industrialized scale [16].
The term 3D Pharming encompasses the various 3D printing and 2D material deposition technologies that are used to create personalized dosage forms. This review paper will focus on recent advances in 3D Pharming efforts between 1996 and February 2016. During this period, powder bed inkjet printing and fused deposition modeling (FDM) were 3D printing platforms commonly used, since these material deposition techniques allow for the fabrication of structures with 2D and 3D spatial gradients. In contrast, platforms that build structures through energy deposition, such as stereolithography, cannot produce pointto- point variations in composition of matter without combining with secondary 2D material deposition techniques. A special focus is given to the advantages and limitations of these two techniques, as well as to the different materials utilized among them for immediate and sustained drug delivery applications. Efforts towards the inclusion of multiple drugs and the synthesis of polypills are reviewed. Finally, the challenges ahead and future work required to make 3D Pharming a reality are evaluated.
Powder Bed Inkjet 3D Printing
Inkjet printing technology is based on two main droplet formation techniques: continuous jet (CJ) printing and drop on demand (DOD) printing. CJ printing relies on a pressurized flow to produce a continuous stream of charged droplets. After being released through a nozzle, these droplets are directed by electrostatic plates into the substrate intended for their deposition, or deviated into a waste recirculation line when not needed for the printing process [17]. DOD printing has a more precise and less wasteful execution, producing droplets that are dispensed only when required by the process, with volumes as low as 1-300 pL [18,19] and frequencies of up to 10,000 Hz. [20]. DOD printheads are primarily actuated by thermal and piezoelectric trigger mechanisms. Thermal printheads have embedded resistors that produce heat upon the induction of an electrical current. This heat creates a bubble within the volatile material being printed that mobilizes a small volume out of the nozzle, resulting in droplet formation. Thermal inkjet printing requires the use of high vapor pressure solvents and produces high temperatures that, although short lived, can result in the degradation of heat-liable bioactive compounds. These factors limit the use of thermal printheads for pharmaceutical applications [21]. In contrast, piezoelectric printheads incorporate piezoelectric materials that expand and contract when induced to an electrical current. These physical deflections generate the pressure required to mobilize liquid out of the nozzle in the form of droplets [22]. The capacity of operating at room temperature with less volatile and more biocompatible liquids makes the piezoelectric printing technology more suitable for the development of drug delivery devices [14,23].
Powder bed 3D printing, a technology originated at MIT, makes use of an inkjet printhead to deposit a layer of binder solution onto a powder bed containing the material desired for object construction [24,25]. The object is defined through the use of computer-aided design (CAD) software and digitally sliced in detailed pieces of information that delineate each one of the layers to be printed through the process. After each layer deposition, a piston that supports the powder bed is lowered allowing a subsequent layer of powder to be spread and selectively bound, as depicted in Figure 1 [26]. This process is repeated several times, stacking layers of solidified material until a predetermined 3D geometry is produced. Excess powder not bound is then removed exposing the final product, which can go through further processing to tune its final mechanical and physical properties [27]. This technology allows for direct control over both, the macro and microstructure of objects, enabling the creation of complex biochemical devices. Incorporating patient specific anatomical data into the process have made possible the creation of implants, prosthetics, diagnostic platforms, and drug delivery systems [28]. Based on the literature research done, Wu et al. conducted the first experiments involving 3D Pharming by printing multi-drug delivery devices in 1996 [11]. In this study, the release profiles of methylene blue and alizarin yellow dyes were controlled by manipulating the three -dimensional position of dyes within the device, its microstructure, and chemical composition. A square grid pattern of 5 cells by 5 cells composed of polyethylene oxide (PEO) was printed and dyes were localized in predefined patterns within the squares. A polycaprolactone (PCL) sheet was printed at the top and bottom of this grid to seal it and prevent dye diffusion upon resorption, yielding a twodimensional diffusion profile limited to the plane of the device. In vitro release studies showed a multiphasic release profile of the dyes incorporated.
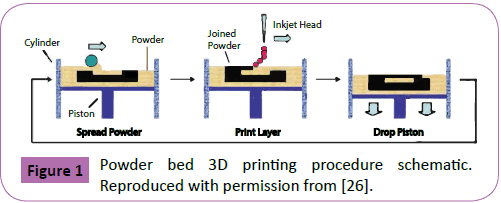
Figure 1: Powder bed 3D printing procedure schematic. Reproduced with permission from [26].
Kastra et al. demonstrated that the drug release mechanisms of these newly conceived devices could be controlled by the chemical properties of the binder utilized and its final concentration within the pill [29]. Eudragit E-100, a cationic methacrylic ester copolymer soluble under acidic conditions below pH 5, was used as a binder to fabricate cellulose tablets with an erosion dominated drug release mechanism. Tablets with diffusion controlled release profiles were made by utilizing Eudragit RLPO as binder. Eudragit RLPO is a permeable and insoluble ammonio-methacrylic acid copolymer and its properties have no dependence on pH. Dissolution studies of these tablets in simulated intestinal fluid demonstrated an increase in drug release time with an increased binder content within the tablet printed. The hardness and friability of the designed drug delivery devices were comparable to commercially available compressed tablets. Moreover, using fluorescein as a model drug, it was shown that this technology can precisely control the dosage of drugs by achieving loads in the pico moles range.
Taking advantage of the control that binders offer over drug release mechanisms, Rowe et al. made use of diverse binders to fabricate tablets with complex drug release profiles [30]. A device with an immediate-extended release profile of the molecule chlorpheniramine was fabricated by using E-100 as a binder for half of the pill and E-RLPO for the second half, as shown in Figure 2A. The immediate release section delivered the full load of chlorpheniramine maleate within the first 30 minutes of the dissolution process. The extended release part maintained a sustained release for a period of 6 hours (Figure 2B). A tablet with a pulse release profile of diclofenac was designed to trigger drug release in both gastric and intestinal fluid by using various binders sensitive to pH values characteristic of these areas. E-100 was used to print a section of the pill sensitive to the low pH found in gastric fluid, whereas Eudragit L-100, an anionic methacrylic ester copolymer sensitive to solutions with pH values above 6, was used to achieve drug release in intestinal fluid. Additionally, breakaway tablets were fabricated to extend the distribution of drugs with low pharmacokinetic transport rates throughout the gastrointestinal wall.
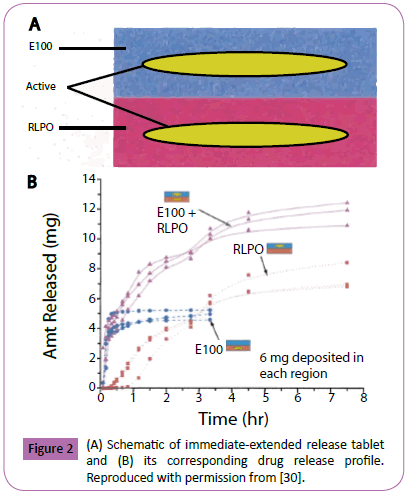
Figure 2: (A) Schematic of immediate-extended release tablet and (B) its corresponding drug release profile. Reproduced with permission from [30].
Wang et al. fabricated cubic drug delivery devices with a nearzero controlled release profile containing pseudoephedrine hydrochloride [31]. The device was composed of hydroxypropyl methylcellulose (HPMC) and Kollidon SR as main materials. The cubic shell portion of the device was printed by utilizing a 15% triethyl citrate solution in ethanol as binder. An inner cubic core was printed with an aqueous binder containing 50% by weight of pseudoephedrine hydrochloride. The system’s drug release mechanism was dominated by diffusion of the drug located at the inner core through the shell layer and out into the dissolution medium. Control of the release profile was shown by the tuning of the HPMC to Kollidon SR ratio, achieving formulations with drug release profile times of 8, 12, and 16 hours as the concentration of HPMC increased, respectively. This near-zero release profile proved to be independent of pH changes in the dissolution medium, paddle stirring rate, or the inclusion of a sinker. To increase the drug load within the tablets, Yu et al. fabricated tablets by pre-mixing the active acetaminophen with the main excipients located in the powder bed, rather than incorporating the drug through the binder [32]. Tablets with acetaminophen concentrations as high as 68% by weight were produced. Furthermore, a zero-order release profile was achieved by printing insoluble layers at the top and bottom of the cylindrical device, resulting in a two-dimensional release profile. Moreover, the devices included a radial gradient of the releaseretardation material ethyl cellulose. This gradient decreased towards the inner part of the tablet, while the void space was gradually increased (Figure 3A). The combination of these factors allowed for a higher drug diffusion as the tablet eroded, causing a constant release rate throughout the dissolution process. Figure 3B shows the erosion process of the device after 0, 1, 3, 5, 7, and 10 hours of dissolution. The incorporation of central holes in compressed tablets has been used to promote zero-order release profiles by maintaining a constant surface area during the simultaneous erosion of its inner aperture and outer layer [33,34]. More recently, Yu et al. fabricated doughnut-shaped acetaminophen tablets and obtained zero-order drug release profiles by printing insoluble and impermeable top and bottom layers, resulting in a 2-dimensional drug release limited to the plane of the device [35]. Other design parameters, such as inner aperture radius, annular thickness, height, and number of binder passes per layer were manipulated. Results showed that the total drug release time increased with decreasing inner radiuses and increasing number of binder passes.
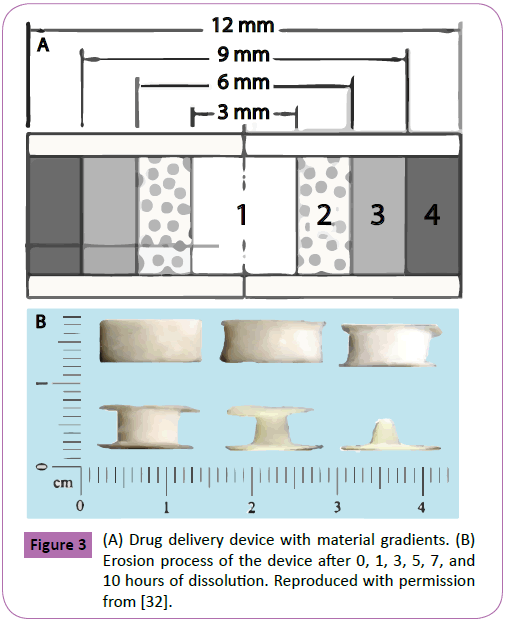
Figure 3: (A) Drug delivery device with material gradients. (B) Erosion process of the device after 0, 1, 3, 5, 7, and 10 hours of dissolution. Reproduced with permission from [32].
Powder bed 3D printing has also been applied towards the fabrication of fast disintegrating/dissolving tablets (FDTs). Yu et al. produced FDTs with average disintegration times of 23.4 seconds [36]. This was achieved by printing tablets with compact top, bottom, and lateral layers, while leaving loose powder in the middle section of the pill resulting in an area of high porosity and permeability (Figure 4). Binder was dispensed in selected areas of the middle section of the pill to increase its mechanical stability. In vitro dissolution tests showed that 98.5% of the active acetaminophen was released within 2 minutes. The FDTs had an acceptable harness value of 63.4 ± 5.4 N/cm2. However, friability studies demonstrated an unsatisfactory mass loss of 3.55 ± 1.16%. This was corrected in a further study by incrementing the number of binder passes through the printing process and not printing selected areas in the middle section of the tablet, resulting in a net weight loss of 0.92 ± 0.14% [37]. Net weight loss values below 1% are considered acceptable based on regulations by the United States Pharmacopeia (USP).
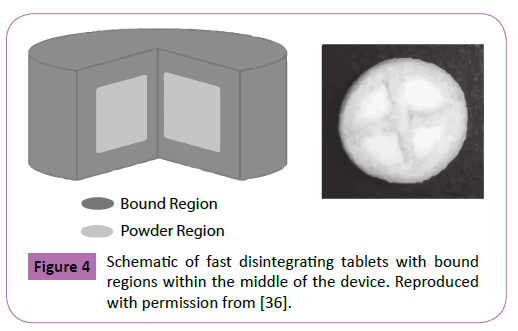
Figure 4: Schematic of fast disintegrating tablets with bound regions within the middle of the device. Reproduced with permission from [36].
In 2015, the FDA approved the first FDT manufactured through powder bed 3D printing [12]. The company Aprecia designed a tablet containing the active levetiracetam, a drug for the treatment of epilepsy, with a dissolution time of about 15 seconds in saliva or 10mL of water [38]. This advancement highlights the potential within this technology for the development of specialized drug forms with features not achievable through compression or other conventional tablet fabrication methods. Nonetheless, prior to its implementation as a definite replacement of current tableting techniques, this technology would require improvements in several areas such as the combination of multiple drugs at high dosages, printing time, and the production of porous, hollow, and more complex architectures for the further regulation of drug release profiles.
Fused Deposition Modelling (FDM)
Fused deposition modelling (FDM) was patented in 1989 by Scott Crump, co-founder of Stratasys Ltd, and developed as an alternative to the inherent limitations of powder bed 3D printing [16,39]. This technique involves the melting, extrusion, and layer by layer deposition of materials that after solidification result in objects with predetermined structures (Figure 5) [40]. To control the pore size and the configuration of the object, variables such as raster angle and thickness, space between rasters, and the extrusion tip diameter can be manipulated. The appropriate heat transfer characteristics and rheological properties are the most critical material qualities evaluated for FDM use. Molten metals, self-hardening waxes, and thermoplastic materials such as nylon, acrylonitrile butadiene styrene, and polyvinyl chloride have been utilized successfully [16,28].
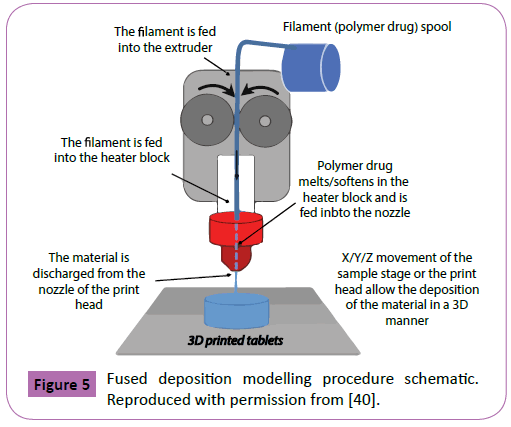
Figure 5: Fused deposition modelling procedure schematic. Reproduced with permission from [40].
Among the advantages of FDM are its lower costs, the ability to print multiple polymers in a single structure, and the capacity to create hollow and porous objects with good mechanical strengths [28]. These characteristics enable FDM as a suitable technique for the manufacturing of personalized tablets and their subsequent discharge at dispense/point-of-care locations. Challenges of this process include the limited amount of thermoplastic materials with appropriate rheological properties and the possible degradation of incorporated drugs, caused by the exposure of active ingredients to high temperatures. These factors combine to severely limit the choice of extrusion materials for tablet printing. The concept of extruding a material containing an active drug for 3D Pharming was first used by Khaled et al. in 2014 [41]. The authors printed bi -layer tablets loaded with the active guaifenesin, an expectorant used to reduce chest congestion. The fabricated tablets contained an immediate release compartment composed of HPMC 2910 as binder, in combination with microcrystalline cellulose and sodium starch glycolate as disintegrants. The other half of the pill featured a sustained release section constituted of HPMC 2208 and poly(acrylic acid) as hydrophilic matrix. These materials were processed separately and combined with the active, resulting in the synthesis of two viscous pastes that were used as feedstock for the printing process. A dissolution analysis of the tablets was performed where the pills were exposed to an acidic medium representative of the stomach for a period of 2 hours, followed by exposure to a 0.2 M trisodium phosphate dodecahydrate solution with a pH of 6.8, representative of the small intestine. The authors reported complete depletion of the drug in the immediate release compartment within the first 30 minutes of dissolution, while maintaining a sustained release for a period of 12 hours. It was demonstrated that the drug release rate at the sustained release section could be controlled by tuning the concentration of HPMC 2208 in the paste, showing a decrease in release rate as the HPMC 2208 was increased. Release profiles were similar to commercially available guaifenesin tablets.
Even though Khaled et al. demonstrated the extrusion of excipients containing actives for the printing of pharmaceutical tablets, their procedure was carried at room temperature and the materials were not melted prior to extrusion, both intrinsic characteristics of FMD. FDM per se was first applied for 3D Pharming when Goyanes et al. printed fluorescein-loaded polyvinyl alcohol (PVA) filaments in 2014 [42]. The authors loaded fluorescein by swelling the polymer filaments in a fluorescent-ethanol solution. The amount of fluorescein incorporated into the filaments was 0.29% w/w, mainly located at the surface of the filaments due to a slow diffusion of the drug into the polymer. Tablets with different infill percentages (Figure 6) were printed by extruding the drug loaded filaments at a temperature of 220°C. Dissolution tests carried out in a bicarbonate buffer at pH 6.8 demonstrated that the drug release rate could be tuned by changing the infill percentage of the tablets, with lower percentages resulting in faster release rates.
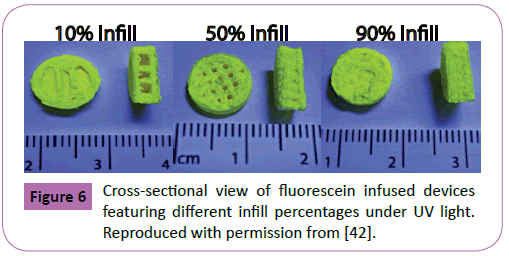
Figure 6: Cross-sectional view of fluorescein infused devices featuring different infill percentages under UV light. Reproduced with permission from [42].
The team later demonstrated the importance of adequate drug selection by the incorporation of two isomeric molecules [43]. The aminosalicylates 5-aminosalicylic acid (5-ASA) and 4-aminosalicylic acid (4-ASA) were incorporated into separate PVA filaments resulting in tablets with drug loads of 0.063 ± 0.001% w/w and 0.236 ± 0.004% w/w, respectively. Even though these molecules are isomers, 5-ASA had a faster release rate than 4-ASA. Moreover, differential scanning calorimetry (DSC) analysis of the 4 -ASA tablet after printing showed a drug degradation of 50%, stating the limitation of the technique regarding thermally labile molecules.
Showrya et al. used FDM to print ellipse-shaped tablets loaded with the steroid prednisolone and demonstrated the weight and dosage accuracy that can be achieved through the FMD technique [10]. PVA filaments were immersed in a methanol solution containing prednisolone, achieving a drug load of 1.9% w/w. The mass of the pills was manipulated by tuning the volume of the tablets. Tablets with weights of 2, 3, 4, 5, 7.5, and 10 mg were printed at an extrusion temperature of 230°C with a dosage accuracy range of 88.7-107%. Thermal analysis by DSC and x-ray powder diffraction (XRPD) confirmed that the drug loaded existed in the amorphous form within the tablets.
An important aspect considered during the design of pharmaceutical tablets is its shape and its effect on drug release profiles. To evaluate this aspect, tablets with several geometries including cube, pyramid, cylinder, sphere, and torus, were printed and their drug release profiles were analyzed [44]. In an effort to increase the drug content within PVA filaments, the drug paracetamol was incorporated by hot melt extrusion (HME), a technique in which multiple materials are extruded at high temperatures to obtain a homogeneous mixture with uniform shape [45-47]. The drug load achieved in the tablets printed was 3.78% w/w. During dissolution studies, tablets with different geometries and equivalent surface areas resulted in drug release rates in the following order; pyramid > torus > cube > sphere and cylinder. This result indicated that drug release rate is dependent on the surface area/volume ratio of the tablet, with higher ratios producing faster release rates. In this case the pyramid design had the highest surface area/volume ratio (1.169) while the sphere had the lowest (0.634).
HME has also been utilized to create drug loaded filaments made out of methacrylic polymers. Pietrzac et al. incorporated the drug theophylline into Eudragit RL, Eudragit RS, and Eudragit E, and 3D printed tablets with a drug loading of 50% and dose accuracy between 91 and 95 percent [9]. It was demonstrated that the mass of the tablet and its printed volume followed a linear relationship. Moreover, increasing the printing resolution of the process did not affect the final mass loaded into the tablet, but resulted in higher printing times. Goyanes et al. expanded the application of FDM by incorporating fluid bed coating techniques into the pills manufactured, in an effort to develop pH controlled drug release profiles [48]. The drug budesonide, commonly used to treat inflammatory bowel disease (IBD), was embedded into PVA through HME resulting in filaments with a drug load of 4.14 ± 0.273%. Tablets containing 9 mg of budesonide were 3D printed and coated with an Eudragit L100 based solution. Drug release studies demonstrated that budesonide release began at the midsmall intestine and maintained a sustained release up to the distal intestine and colon. FMD has also been utilized to fabricate hollow capsular devices for drug incorporation. Melocchi et al. created hydroxypropyl cellulose filaments and demonstrated the feasibility of FMD for this purpose by comparing the product obtained to capsules manufactured by injection molding [49]. Capsules made through both methods were loaded with 80 mg of acetaminophen and dissolution tests showed similar drug release profiles. This technique features advantages over the powder bed 3D printing technology such as the ability to produce more complex structures, print multiple materials in a single tablet, and a lower costs of equipment. Yet, more efforts towards the reduction of drug degradation due to heat exposure and the development of more materials suitable for FDM are required.
Multiple Drugs Incorporation
Since the first publication on this topic [11], one of the goals of 3D Pharming has been to deliver patient-specific combinations of multiple drugs into a single tablet, customized to the needs of the patient in terms of drug choice and dosage. This advancement would reduce the number of pills consumed by patients on a daily basis and potentially enhance patient compliance [15]. 3D Pharming has been applied within several studies in order to incorporate multiple drugs into one tablet, while controlling their individual release rates, profiles, and release mechanisms. These are critical parameters to take into consideration during the design of a drug delivery device such as pharmaceutical tablets, as they define the location and the time where the drug release occurs within the gastrointestinal (GI) track, as well as the concentration of drug secreted through a defined period of time. Sun et at. demonstrated a novel technique to create customized drug release profiles within a tablet, producing profiles with a constant rate of release, pulsed rate, increased rate, and decreased rate release [50]. In their study, an impermeable polylactic acid (PLA) tablet was 3D printed, leaving an opening at the top of it to allow for drug diffusion, as observed in Figure 7A. To fill the tablet, a pre-polymer solution was casted in polydimethylsiloxane (PDMS) molds with different shapes and cured by exposing the solution to UV light for a period of 10 minutes. The precursor solution was composed of 4-pentenoic anhydride, pentaerythritol tetrakis (3-mercaptopropionate) (PETMP), and/or ethylene glycol dithiol (EGDT; 3,5 -dioxa-1,8- dithioocatne) as crosslinker, using 1-hydroxycyclohexyl phenyl ketone as photoinitiator. After polymerization, the drug loaded material was located inside the tablet and the void spaces were filled by drug-free pre-polymer solution and exposed to UV light, culminating the tablet fabrication. Orange G and Brilliant Blue G were utilized as model drugs. Figure 7B shows how the release profiles of the two dyes are directly dependent on the shape of the polymerized solution introduced. The study showed a novel technique for the release of multiple drugs within a tablet with diverse customized release profiles. Moreover, the release rate could be further modified by manipulating the ratio between PETMP and the crosslinker EGDT, with lower crosslinking ratios resulting in faster drug release rates.
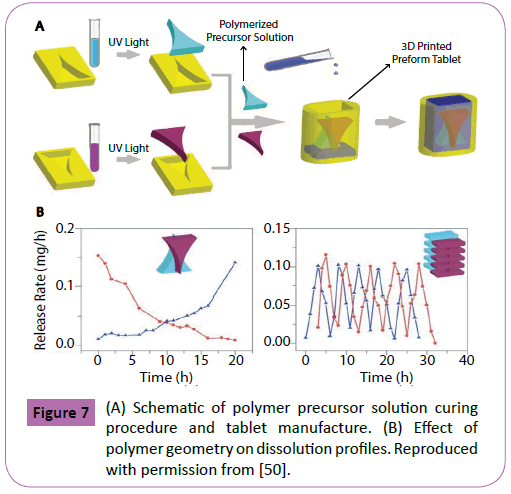
Figure 7: (A) Schematic of polymer precursor solution curing procedure and tablet manufacture. (B) Effect of polymer geometry on dissolution profiles. Reproduced with permission from [50].
In a different study, Goyanes et al. used FDM to manufacture tablets containing the molecules paracetamol and caffeine [51]. The filaments used for the printing process were made by mixing each drug per separate with PVA and applying HME. Filaments with two different drug concentrations were made for each molecule, achieving drug loads of 4.3% and 8.2% for paracetamol and 4.7% and 9.5% for caffeine. In order to obtain diverse drug release profiles, tablets with two different designs were 3D printed. The first design featured 1 mm alternate layers of caffeine and paracetamol, as shown in Figure 8A. The second design, named DuoCaplets (9.0 mm length x 3.34 mm diameter), consisted of a capsule shaped core containing one drug in the inside of the tablet and an outer layer where the opposite drug was located (Figure 8B). Release studies were performed in a bicarbonate buffer at different pH values to simulate various sections of the GI track. Results demonstrated a simultaneous release of both drugs within the model featuring alternate layers, whereas the DuoCaplets model showed release of the drug located at the outer layer followed by the drug located at the inner side of the capsule. It was also demonstrated that the release rate of the drugs increased with an increased drug concentration within the filaments extruded.
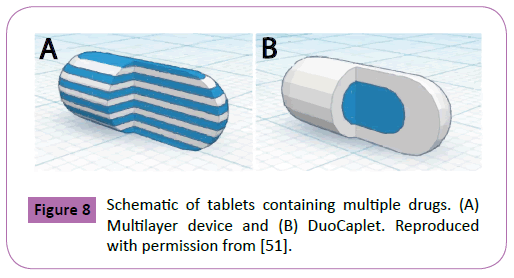
Figure 8: Schematic of tablets containing multiple drugs. (A) Multilayer device and (B) DuoCaplet. Reproduced with permission from [51].
Besides achieving control of the release profile of multiple drugs through adjustments on the tablet’s design, other studies have incorporated diverse drug release mechanisms to regulate this parameter. Khaled et al. designed a polypill containing the drugs captopril, nifedipine, and glipizidine, a combination of drugs used to treat diabetics suffering from hypertension [52]. These drugs were released through two different mechanisms: diffusion and osmosis. The drug captopril was incorporated within an osmotic pump designed by incorporating sodium chloride as an osmogen in the mixture of excipients extruded, which resulted in a porous shell upon dissolution of the sodium chloride. The drugs nifedipine and glipizide were incorporated within HPMC, a material that swells upon exposure to a liquid medium and promotes a sustained release of the drugs encapsulated. Release studies demonstrated that the drug captopril showed a zero order drug release profile, induced by the osmotic pump designed. The drugs nifedipine and glipizidine followed a Kormeyer-Peppas or first order release kinetics that varied with the active/excipient ratio utilized. These pills were printed by extruding pastes of excipients and actives at room temperature, a technique developed by Khaled et al. previously discussed in the Fused Deposition Modelling section [41].
The team subsequently printed a polypill containing 5 drugs: pravastatin, atenolol, ramipril, aspirin, and hydrochlorothiazide [53]. Developed to treat and prevent a multitude of cardiovascular diseases and high blood pressure, the drugs were incorporated and segregated through different compartments in a single tablet (Figure 9). The drugs aspirin and hydrochlorothiazide were located within immediate release compartments containing sodium starch glycolate as disintegrant, which induced the release of 100% of the drug within the first 30 minutes of dissolution. The drugs pravastatin, atenolol, and ramipril were located into compartments containing HMPC, designated to have a sustained release that continued for a period of 720 minutes. This study represents the maximum amount of drugs incorporated into a single 3D printed tablet to date.
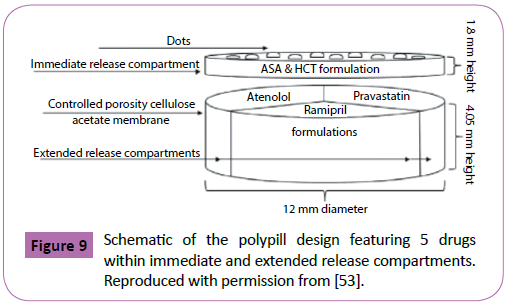
Figure 9: Schematic of the polypill design featuring 5 drugs within immediate and extended release compartments. Reproduced with permission from [53].
Conclusion and Future Directions
The literature is replete with exciting demonstrations of 3D Pharming that can enable personalized medicine by producing patient specific formulations with speed and precision. Additionally, the required equipment is capable of being installed and operated in diverse settings, including traditional pharmacies as well as point of care locations such as hospitals and residential care facilities. Besides being highly scalable and cost effective, the precise amount of drugs and excipients deposited during pill fabrication can be tracked, offering unprecedented access to quality assurance. Most excitingly, the patient specific formulations and dosages can be adjusted according to phenotypic evidence of intended results and undesirable side effects. This information can be loaded into the patient's individual database.
Additional efforts are required in order to increase the speed of production and satisfy the high demand for tablets loaded with multiple drugs at tailored dosages. Besides powder printing and FDM, other technologies that deposit matter through physiological and drug-compatible manners are being developed. PolyJet printing, a technology that dispenses photocurable polymer solutions into a tray, would reduce the manufacturing time of oral drug forms by maximizing the speed capabilities inherent of inkjet printing. More importantly, the engineering of biocompatible materials that maximize drug stability for the application of such technology would provide a novel alternative towards 3D Pharming. Different excipient materials are needed to print hydrophilic/hydrophobic drugs with varying degrees of solubility. In addition, these excipients must be compatible with each other and with the deposition technology.
Beyond the scientific and engineering challenges, there are also regulatory obstacles that need to be addressed for the implementation of this technology. Advantages of depositing drugs drop-by-drop include precise control over dosage, high spatial resolution to create compositional gradients, and ability to monitor with video camera for quality assurance. A common limitation for both CJ and DOD printheads for 3D Pharming is that many drugs are poorly soluble in most biocompatible printable fluids, and they may need to be deposited in dispersions or particulate forms. Practical quality assurance monitoring subsystems that allow real-time and high resolution determination of drug dosing will be needed to ensure patient safety and efficacy.
An analysis of the economical feasibility of this paradigm shift within the pharmaceutical industry is needed regarding equipment expenditures, drug production, and adjustment of current regulations to overview novel protocols and pharmaceutical apparatuses. Currently, a tablet containing a variety of drugs would be considered by the FDA as a new combination drug formulation, requiring extensive clinical trials to assess its effectiveness and guarantee patient safety. Additionally, each location operating a 3D printer for the production and discharge of pharmaceutical prescriptions would require certification as a GMP facility. Efforts from regulating agencies in concert with the scientific community are required to develop regulations that ensure the safety of patients while promoting scientific advancement.
The choice of drug combination and dose that suits a patient’s physiology will come from a combination of clinical phenotypic findings, pharmacogenomics data, and optimization search algorithms. Studies have demonstrated that primary care physicians do not feel confident regarding their ability to analyze data derived from genetic tests [54]. Reforms to medical curriculums, development of specialist training for medical geneticists, and implementation of personalized medicine certifications for on-going physicians are measures required to satisfy the demand of professionals in this new emerging field [55]. Furthermore, efforts to develop the infrastructure required to store the biomedical data acquired and guidelines defining how this information is used to drive the identification and qualification of diverse biomarkers are necessary [56]. Since optimization search algorithms tend to improve with increasing data, guidelines will be needed to balance performance versus sharing of big data.
3D Pharming brings us a step closer to personalized medicine. The numerous cutting edge technologies described in this review are being developed to overcome basic limitations. This powerful transformation must be carefully controlled to protect society and individual privacy, while maximizing safety and efficacy.
Competing and Conflicting Interests
The authors declare that they have no competing or conflicting interests.
References
- Schork NJ (2015) Personalized medicine: Time for one-person trials. Nature 520: 609-611.
- Karapetis CS (2008) K-ras Mutations and Benefit from Cetuximab in Advanced Colorectal Cancer. N Engl J Med 359: 1757-1765.
- Ting S, Schug S (2016) The pharmacogenomics of pain management: prospects for personalized medicine. J Pain Res 9: 49-56.
- Chadwick R (2013) Ethical issues in personalized medicine. Drug Discov Today Ther Strateg 10: e171-e174.
- Burke W, Brown Trinidad S, Press NA (2014) Essential elements of personalized medicine. Urol Oncol 32: 193-197.
- Mirnezami R, Nicholson J, Darzi A (2012) Preparing for Precision Medicine. N Engl J Med 366: 489-491.
- Beebe K, Kennedy AD (2016) Sharpening Precision Medicine by a Thorough Interrogation of Metabolic Individuality. Comput Struct Biotechnol J 14: 97-105.
- Tutton R (2012) Personalizing medicine: Futures present and past. Soc Sci Med 75: 1721-1728.
- Pietrzak K, Isreb A, Alhnan MA (2015) A flexible-dose dispenser for immediate and extended release 3D printed tablets. Eur J Pharm Biopharm 96: 380-387.
- Skowyra J, Pietrzak K, Alhnan M (2015) Fabrication of extended-release patient-tailored prednisolone tablets via fused deposition modelling (FDM) 3D printing. Eur J Pharm Sci 68: 11-17.
- Wu BM, Borland SW, Giordano R, Cima LG, Sachs EM, et al. (1996) Solid free-form fabrication of drug delivery devices. J Control Release 40: 77-87.
- Aprecia_Pharmaceuticals, FDA approves the first 3D printed drug product (2015).
- Choonara YE, du Toit LC, Kumar P, Kondiah PPD, Pillay V (2016)3D-printing and the effect on medical costs: a new era? Expert Rev Pharmacoecon Outcomes Res 16: 23-32.
- Yu DG, Zhu L-M, Brandford-White CJ, Yang XL (2008) Three-Dimensional Printing in Pharmaceutics: Promises and Problems. J Pharm Sci 97: 3666-3690.
- Sleight P, Pouleur H, Zannad F (2006) Benefits, challenges, and registerability of the polypill. Eur Heart J 27: 1651-1656.
- Prasad LK, Smyth H (2015)3D Printing technologies for drug delivery: a review. Drug Dev Ind Pharm 42: 1019-1031.
- Derby B (2010) Inkjet Printing of Functional and Structural Materials: Fluid Property Requirements, Feature Stability, and Resolution. Annu Rev Mater Res 40: 395-414.
- Sekitani T, Noguchi Y, Zschieschang U, Klauk H, Someya T(2008) Organic transistors manufactured using inkjet technology with subfemtoliter accuracy. Proc Natl Acad Sci U S A 105: 4976-4980.
- Singh M, Haverinen HM, Dhagat P, Jabbour GE (2010) Inkjet printing-process and its applications. Adv Mater 22: 673-685.
- Demirci U, Montesano G (2007) Single cell epitaxy by acoustic picolitre droplets. Lab Chip 7: 1139-1145.
- Alomari M, Mohamed FH, Basit AW, Gaisford S (2015) Personalised dosing: Printing a dose of one’s own medicine. Int J Pharm 494: 568-577.
- Tekin E, Smith PJ, Schubert US (2008) Inkjet printing as a deposition and patterning tool for polymers and inorganic particles. Soft Matter 4: 703-713.
- Sumerel J, Lewis J, Doraiswamy A, Deravi LF, Sewell SL, et al. (2006) Piezoelectric ink jet processing of materials for medical and biological applications. Biotechnol J 1: 976-987.
- Cima MJ, Sachs E, Cima LG, Khanujal S, Borland SW, et al. (1994) Computer-derived microstructures by 3D Printing: Bio and Structural Materials. Solid Free Fabr Symp 19: 181-190.
- Griffith LG, Wu B, Cima MJ, Powers MJ, Chaignaud B, et al. (1997) In vitro organogenesis of liver tissue. Ann N Y Acad Sci 831: 382-397.
- Lu Y, Chen SC (2004) Micro and nano-fabrication of biodegradable polymers for drug delivery. Adv Drug Deliv Rev 56: 1621-1633.
- Chia HN, Wu BM (2015) Improved resolution of 3D printed scaffolds by shrinking. J Biomed Mater Res - Part B Appl Biomater 103: 1415-1423.
- Chia HN, Wu BM (2015) Recent advances in 3D printing of biomaterials. J Biol Eng 9: 1–14.
- Katstra WE, Palazzolo RD, Rowe CW, Giritlioglu B, Teung P, et al. (2000) Oral dosage forms fabricated by Three Dimensional Printing. J Control Release 66: 1-9.
- Rowe CW, Katstra WE, Palazzolo RD, Giritlioglu B, Teung P, et al. (2000) Multimechanism oral dosage forms fabricated by three dimensional printing. J Control Release 66: 11-17.
- Wang C-C, Tejwani MMR, Roach WJ, Kay JL, Yoo J, et al. (2006) Development of Near Zero-Order Release Dosage Forms Using Three-Dimensional Printing (3-DPTM) Technology. Drug Dev Ind Pharm 32: 367-376.
- Yu DG, Yang XL, Huang WD, Liu J, Wang YG, Xu H(2007) Tablets with Material Gradients Fabricated by Three-Dimensional Printing. J Pharm Sci 96: 2446-2456.
- Cheng K, Zhu J, Song X, Sun L, Zhang J (1999) Studies of hydroxypropyl methylcellulose donut-shaped tablets. Drug Dev Ind Pharm 25: 1067-1071.
- Sundy E, Paul Danckwerts M (2004) A novel compression-coated doughnut-shaped tablet design for zero-order sustained release. Eur J Pharm Sci 22: 477-485.
- Yu DG, Branford-White C, Ma ZH, Zhu LM, Li XY, et al. (2009) Novel drug delivery devices for providing linear release profiles fabricated by 3DP. Int J Pharm 370: 160-166.
- Yu D-G, Shen X-X, Branford-White C, Zhu L-M, White K, et al. (2009) Novel oral fast-disintegrating drug delivery devices with predefined inner structure fabricated by Three-Dimensional Printing. J Pharm Pharmacol 61: 323-329.
- Yu D-G, Branford-White C, Yang Y-C, Zhu L-M, Welbeck EW, et al. (2009) A novel fast disintegrating tablet fabricated by three-dimensional printing. Drug Dev Ind Pharm 35: 1530-1536.
- Jacob J, Coyle N, West TG (2014) Rapid disperse dosage form containing levetiracetam.
- Van Noort R (2012) The future of dental devices is digital. Dent Mater 28: 3-12.
- Qi S, Craig D (2016) Recent developments in micro- and nanofabrication techniques for the preparation of amorphous pharmaceutical dosage forms. Adv Drug Deliv Rev 100: 67-84.
- Khaled SA, Burley JC, Alexander MR, Roberts CJ (2014) Desktop 3D printing of controlled release pharmaceutical bilayer tablets. Int J Pharm 461: 105-111.
- Goyanes A, Buanz ABM, Basit AW, Gaisford S (2014) Fused-filament 3D printing (3DP) for fabrication of tablets. Int J Pharm 476: 88-92.
- Goyanes A, Buanz ABM, Hatton GB, Gaisford S, Basit AW (2015) 3D printing of modified-release aminosalicylate (4-ASA and 5-ASA) tablets. Eur J Pharm Biopharm 89: 157-162.
- Goyanes A, Robles Martinez P, Buanz A, Basit AW, Gaisford S (2015) Effect of geometry on drug release from 3D printed tablets. Int J Pharm 494: 657-663.
- Breitenbach J (2002) Melt extrusion: from process to drug delivery technology. Eur J Pharm Biopharm 54: 107-117.
- Lang B, McGinity JW, Williams RO (2014) Hot-melt extrusion - basic principles and pharmaceutical applications. Drug Dev Ind Pharm 40: 1133-1155.
- Thiry J, Krier F, Evrard B (2015) A review of pharmaceutical extrusion: Critical process parameters and scaling-up. Int J Pharm 479: 227-240.
- Goyanes A, Chang H, Sedough D, Hatton GB, Wang J, et al. (2015)Fabrication of controlled-release budesonide tablets via desktop (FDM) 3D printing. Int J Pharm 496: 414-420.
- Melocchi A, Parietti F, Loreti G, Maroni A, Gazzaniga A, et al. (2015) 3D printing by fused deposition modeling (FDM) of a swellable/erodible capsular device for oral pulsatile release of drugs. J Drug Deliv Sci Technol 30: 360-367.
- Sun Y, Soh S (2015) Printing Tablets with Fully Customizable Release Profiles for Personalized Medicine. Adv Mater 27: 7847-7853.
- Goyanes A, Wang J, Buanz A, Martinez-Pacheco R, Telford R, et al. (2015) 3D printing of medicines: Engineering novel oral devices with unique design and drug release characteristics. Mol Pharm 12: 4077-4084.
- Khaled SA, Burley JC, Alexander MR, Yang J, Roberts CJ (2015) 3D printing of tablets containing multiple drugs with defined release profiles. Int J Pharm 494: 643-650.
- Khaled SA, Burley JC, Alexander MR, Yang J, Roberts CJ(2015) 3D printing of five-in-one dose combination polypill with defined immediate and sustained release profiles. J Control Release 217: 308-314.
- Powell KP, Cogswell WA, Christianson CA, Dave G, Verma A, et al. (2012) Primary care physicians’ awareness, experience and opinions of direct-to-consumer genetic testing. J Genet Couns 21: 113-126.
- Mcgrath S, Ghersi D (2016) Building towards precision medicine: empowering medical professionals for the next revolution. BMC Medical Genomics 9: 1-6.
- Elefsinioti A, Bellaire T, Wang A, Quast K, Seidel H, et al. (2016) Key factors for successful data integration in biomarker research. Nat Rev Drug Discov 15: 369-370.